5
Pelvis and Perineum
Ischio-anal fossae and their anterior recesses
ADDITIONAL LEARNING RESOURCES FOR CHAPTER 5, PELVIS AND PERINEUM, ON STUDENT CONSULT (www.studentconsult.com)
 Image Library—illustrations of pelvic and perineal anatomy, Chapter 5
Image Library—illustrations of pelvic and perineal anatomy, Chapter 5
 Self-Assessment (scored)—National Board style multiple-choice questions, Chapter 5
Self-Assessment (scored)—National Board style multiple-choice questions, Chapter 5
 Short Questions (not scored)—National Board style multiple-choice questions, Chapter 5
Short Questions (not scored)—National Board style multiple-choice questions, Chapter 5
 Interactive Surface Anatomy—interactive surface animations, Chapter 5
Interactive Surface Anatomy—interactive surface animations, Chapter 5
 Medical Clinical Case Studies
Medical Clinical Case Studies Clinical Cases
Clinical CasesLeft common iliac artery obstruction
Regional anatomy
The pelvis and perineum are interrelated regions associated with the pelvic bones and the terminal parts of the vertebral column. The pelvis is divided into two regions (Fig. 5.1):
 The superior region related to upper parts of the pelvic bones and lower lumbar vertebrae is the false pelvis (greater pelvis) and is generally considered part of the abdomen.
The superior region related to upper parts of the pelvic bones and lower lumbar vertebrae is the false pelvis (greater pelvis) and is generally considered part of the abdomen. The true pelvis (lesser pelvis) is related to the inferior parts of the pelvic bones, sacrum, and coccyx, and has an inlet and an outlet.
The true pelvis (lesser pelvis) is related to the inferior parts of the pelvic bones, sacrum, and coccyx, and has an inlet and an outlet.
Fig. 5.1 Pelvis and perineum.
The bowl-shaped pelvic cavity (Fig. 5.1) enclosed by the true pelvis consists of the pelvic inlet, walls, and floor. This cavity is continuous superiorly with the abdominal cavity and contains and supports elements of the urinary, gastrointestinal, and reproductive systems.
The perineum (Fig. 5.1) is inferior to the floor of the pelvic cavity; its boundaries form the pelvic outlet. The perineum contains and supports the external genitalia and external openings of the genitourinary and gastrointestinal systems.
PELVIS
Bones
The bones of the pelvis consist of the right and left pelvic (hip) bones, the sacrum, and the coccyx. The sacrum articulates superiorly with vertebra LV at the lumbosacral joint. The pelvic bones articulate posteriorly with the sacrum at the sacro-iliac joints and with each other anteriorly at the pubic symphysis.
Pelvic bone
The pelvic bone is irregular in shape and has two major parts separated by an oblique line on the medial surface of the bone (Fig. 5.2A):
 The pelvic bone above this line represents the lateral wall of the false pelvis, which is part of the abdominal cavity.
The pelvic bone above this line represents the lateral wall of the false pelvis, which is part of the abdominal cavity. The pelvic bone below this line represents the lateral wall of the true pelvis, which contains the pelvic cavity.
The pelvic bone below this line represents the lateral wall of the true pelvis, which contains the pelvic cavity.
Fig. 5.2 Right pelvic bone. A. Medial view. B. Lateral view.
The linea terminalis is the lower two-thirds of this line and contributes to the margin of the pelvic inlet.
The lateral surface of the pelvic bone has a large articular socket, the acetabulum, which together with the head of the femur, forms the hip joint (Fig. 5.2B).
Inferior to the acetabulum is the large obturator foramen, most of which is closed by a flat connective tissue membrane, the obturator membrane. A small obturator canal remains open superiorly between the membrane and adjacent bone, providing a route of communication between the lower limb and the pelvic cavity.
The posterior margin of the bone is marked by two notches separated by the ischial spine (Fig. 5.2):
 the greater sciatic notch, and
the greater sciatic notch, and
 the lesser sciatic notch.
the lesser sciatic notch.The posterior margin terminates inferiorly as the large ischial tuberosity.
The irregular anterior margin of the pelvic bone is marked by the anterior superior iliac spine, the anterior inferior iliac spine, and the pubic tubercle.
Components of the pelvic bone
Each pelvic bone is formed by three elements: the ilium, pubis, and ischium. At birth, these bones are connected by cartilage in the area of the acetabulum; later, at between 16 and 18 years of age, they fuse into a single bone (Fig. 5.3).

Fig. 5.3 Ilium, ischium, and pubis.
Of the three components of the pelvic bone, the ilium is the most superior in position.
The ilium is separated into upper and lower parts by a ridge on the medial surface (Fig. 5.4A).
 Posteriorly, the ridge is sharp and lies immediately superior to the surface of the bone that articulates with the sacrum. This sacral surface has a large L-shaped facet for articulating with the sacrum and an expanded, posterior roughened area for the attachment of the strong ligaments that support the sacro-iliac joint (Fig. 5.4).
Posteriorly, the ridge is sharp and lies immediately superior to the surface of the bone that articulates with the sacrum. This sacral surface has a large L-shaped facet for articulating with the sacrum and an expanded, posterior roughened area for the attachment of the strong ligaments that support the sacro-iliac joint (Fig. 5.4).
 Anteriorly, the ridge separating the upper and lower parts of the ilium is rounded and termed the arcuate line (Fig. 5.4).
Anteriorly, the ridge separating the upper and lower parts of the ilium is rounded and termed the arcuate line (Fig. 5.4).

Fig. 5.4 Components of the pelvic bone. A. Medial surface. B. Lateral surface.
The arcuate line forms part of the linea terminalis and the pelvic brim.
The portion of the ilium lying inferiorly to the arcuate line is the pelvic part of the ilium and contributes to the wall of the lesser or true pelvis.
The upper part of the ilium expands to form a flat, fan-shaped “wing,” which provides bony support for the lower abdomen, or false pelvis (Fig. 5.4). This part of the ilium provides attachment for muscles functionally associated with the lower limb. The anteromedial surface of the wing is concave and forms the iliac fossa. The external (gluteal surface) of the wing is marked by lines and roughenings and is related to the gluteal region of the lower limb (Fig. 5.4B).
The entire superior margin of the ilium is thickened to form a prominent crest (the iliac crest), which is the site of attachment for muscles and fascia of the abdomen, back, and lower limb and terminates anteriorly as the anterior superior iliac spine and posteriorly as the posterior superior iliac spine (Fig. 5.4).
A prominent tubercle, tuberculum of iliac crest, projects laterally near the anterior end of the crest; the posterior end of the crest thickens to form the iliac tuberosity (Fig. 5.4).
Inferior to the anterior superior iliac spine of the crest, on the anterior margin of the ilium, is a rounded protuberance called the anterior inferior iliac spine (Fig 5.4). This structure serves as the point of attachment for the rectus femoris muscle of the anterior compartment of the thigh and the iliofemoral ligament associated with the hip joint. A less prominent posterior inferior iliac spine (Fig 5.4) occurs along the posterior border of the sacral surface of the ilium, where the bone angles forward to form the superior margin of the greater sciatic notch.
Clinical app
Bone marrow biopsy
In certain diseases (e.g., leukemia), a sample of bone marrow must be obtained to assess the stage and severity of the problem. The iliac crest is often used for such bone marrow biopsies. The iliac crest lies close to the surface, is palpable, and is easily accessed.
The anterior and inferior part of the pelvic bone is the pubis (Fig. 5.4). It has a body and two arms (rami).
 The body is flattened dorsoventrally and articulates with the body of the pubic bone on the other side at the pubic symphysis. The body has a rounded pubic crest on its superior surface that ends laterally as the prominent pubic tubercle.
The body is flattened dorsoventrally and articulates with the body of the pubic bone on the other side at the pubic symphysis. The body has a rounded pubic crest on its superior surface that ends laterally as the prominent pubic tubercle. The superior pubic ramus projects posterolaterally from the body and joins with the ilium and ischium at its base, which is positioned toward the acetabulum. The sharp superior margin of this triangular surface is termed the pecten pubis (pectineal line), which forms part of the linea terminalis of the pelvic bone and the pelvic inlet. Anteriorly, this line is continuous with the pubic crest, which also is part of the linea terminalis and pelvic inlet. The superior pubic ramus is marked on its inferior surface by the obturator groove, which forms the upper margin of the obturator canal.
The superior pubic ramus projects posterolaterally from the body and joins with the ilium and ischium at its base, which is positioned toward the acetabulum. The sharp superior margin of this triangular surface is termed the pecten pubis (pectineal line), which forms part of the linea terminalis of the pelvic bone and the pelvic inlet. Anteriorly, this line is continuous with the pubic crest, which also is part of the linea terminalis and pelvic inlet. The superior pubic ramus is marked on its inferior surface by the obturator groove, which forms the upper margin of the obturator canal. The inferior ramus projects laterally and inferiorly to join with the ramus of the ischium.
The inferior ramus projects laterally and inferiorly to join with the ramus of the ischium.
The ischium is the posterior and inferior part of the pelvic bone (Fig. 5.4). It has:
 a large body that projects superiorly to join with the ilium and the superior ramus of the pubis; and
a large body that projects superiorly to join with the ilium and the superior ramus of the pubis; and a ramus that projects anteriorly to join with the inferior ramus of the pubis.
a ramus that projects anteriorly to join with the inferior ramus of the pubis.
The posterior margin of the bone is marked by a prominent ischial spine (Fig. 5.4) that separates the lesser sciatic notch, below, from the greater sciatic notch, above.
The most prominent feature of the ischium is a large tuberosity (the ischial tuberosity) on the posteroinferior aspect of the bone (Fig. 5.4). This tuberosity is an important site for the attachment of lower limb muscles and for supporting the body when sitting.
Sacrum
The sacrum, which has the appearance of an inverted triangle, is formed by the fusion of the five sacral vertebrae (Fig. 5.5). The base of the sacrum articulates with vertebra LV, and its apex articulates with the coccyx. Each of the lateral surfaces of the bone bears a large L-shaped facet for articulation with the ilium of the pelvic bone. Posterior to the facet is a large roughened area for the attachment of ligaments that support the sacro-iliac joint. The superior surface of the sacrum is characterized by the superior aspect of the body of vertebra SI and is flanked on each side by an expanded winglike transverse process termed the ala (Fig. 5.5A). The anterior edge of the vertebral body projects forward as the promontory. The anterior surface of the sacrum is concave; the posterior surface is convex. Because the transverse processes of adjacent sacral vertebrae fuse laterally to the position of the intervertebral foramina and laterally to the bifurcation of spinal nerves into posterior and anterior rami, the posterior and anterior rami of spinal nerves S1 to S4 emerge from the sacrum through separate foramina. There are four pairs of anterior sacral foramina on the anterior surface of the sacrum for anterior rami (Fig. 5.5A), and four pairs of posterior sacral foramina on the posterior surface for the posterior rami (Fig. 5.5B). The sacral canal is a continuation of the vertebral canal that terminates as the sacral hiatus.

Fig. 5.5 LV vertebra, sacrum, and coccyx. A. Anterior view. B. Posterior view. C. Lateral view.
Coccyx
The small terminal part of the vertebral column is the coccyx, which consists of four fused coccygeal vertebrae (Fig. 5.5A) and, like the sacrum, has the shape of an inverted triangle. The base of the coccyx is directed superiorly. The superior surface bears a facet for articulation with the sacrum and two horns, or cornua, one on each side, that project upward to articulate or fuse with similar downward-projecting cornua from the sacrum. These processes are modified superior and inferior articular processes that are present on other vertebrae. Each lateral surface of the coccyx has a small rudimentary transverse process, extending from the first coccygeal vertebra. Vertebral arches are absent from coccygeal vertebrae; therefore no bony vertebral canal is present in the coccyx.
Joints
Lumbosacral joints
The sacrum articulates superiorly with the lumbar part of the vertebral column. The lumbosacral joints are formed between vertebra LV and the sacrum and consist of (Fig. 5.6A):
 the two zygapophyseal joints, which occur between adjacent inferior and superior articular processes; and
the two zygapophyseal joints, which occur between adjacent inferior and superior articular processes; and an intervertebral disc that joins the bodies of vertebrae LV and SI.
an intervertebral disc that joins the bodies of vertebrae LV and SI.
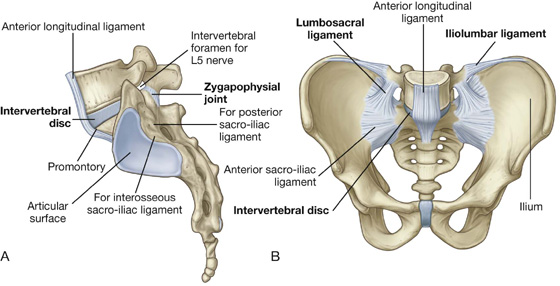
Fig. 5.6 Lumbosacral joints and associated ligaments. A. Lateral view. B. Anterior view.
These joints are similar to those between other vertebrae, with the exception that the sacrum is angled posteriorly on vertebra LV. As a result, the anterior part of the intervertebral disc between the two bones is thicker than the posterior part.
The lumbosacral joints are reinforced by strong iliolumbar and lumbosacral ligaments that extend from the expanded transverse processes of vertebra LV to the ilium and the sacrum, respectively (Fig. 5.6B).
Sacro-iliac joints
The sacro-iliac joints transmit forces from the lower limbs to the vertebral column. They are synovial joints between the L-shaped articular facets on the lateral surfaces of the sacrum and similar facets on the iliac parts of the pelvic bones (Figs. 5.6A, 5.7A). The joint surfaces have an irregular contour and interlock to resist movement. The joints often become fibrous with age and may become completely ossified.
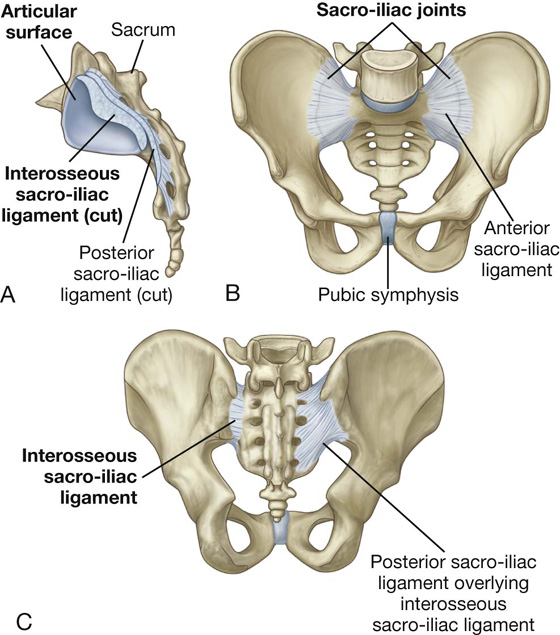
Fig. 5.7 Sacro-iliac joints and associated ligaments. A. Lateral view. B. Anterior view. C. Posterior view.
Each sacro-iliac joint is stabilized by three ligaments:
 the anterior sacro-iliac ligament, which is a thickening of the fibrous membrane of the joint capsule and runs anteriorly and inferiorly to the joint (Figs. 5.6B, 5.7B);
the anterior sacro-iliac ligament, which is a thickening of the fibrous membrane of the joint capsule and runs anteriorly and inferiorly to the joint (Figs. 5.6B, 5.7B);
 the interosseus sacro-iliac ligament, which is the largest, strongest ligament of the three, is positioned immediately posterosuperior to the joint and attaches to adjacent expansive roughened areas on the ilium and sacrum, thereby filling the gap between the two bones (Fig. 5.7A and 5.7C); and
the interosseus sacro-iliac ligament, which is the largest, strongest ligament of the three, is positioned immediately posterosuperior to the joint and attaches to adjacent expansive roughened areas on the ilium and sacrum, thereby filling the gap between the two bones (Fig. 5.7A and 5.7C); and
 the posterior sacro-iliac ligament, which covers the interosseus sacro-iliac ligament (Fig. 5.7C).
the posterior sacro-iliac ligament, which covers the interosseus sacro-iliac ligament (Fig. 5.7C).
Clinical app
Common problems with the sacro-iliac joints
The sacro-iliac joints have both fibrous and synovial components, and as with many weight-bearing joints, degenerative changes may occur and cause pain and discomfort in the sacro-iliac region. In addition, disorders associated with the major histocompatibility complex antigen HLA B27, such as rheumatoid arthritis, psoriasis, and inflammatory bowel disease, can produce specific inflammatory changes within these joints.
Pubic symphysis joint
The pubic symphysis lies anteriorly between the adjacent surfaces of the pubic bones (Fig. 5.8). Each of the joint’s surfaces is covered by hyaline cartilage and is linked across the midline to adjacent surfaces by fibrocartilage. The joint is surrounded by interwoven layers of collagen fibers and the two major ligaments associated with it are (Fig. 5.8):
 the superior pubic ligament, located above the joint; and
the superior pubic ligament, located above the joint; and
 the inferior pubic ligament, located below it.
the inferior pubic ligament, located below it.

Fig. 5.8 Pubic symphysis and associated ligaments.
Orientation
In the anatomical position, the pelvis is oriented so that the front edge of the top of the pubic symphysis and the anterior superior iliac spines lie in the same vertical plane (Fig. 5.9). As a consequence, the pelvic inlet, which marks the entrance to the pelvic cavity, is tilted to face anteriorly, and the bodies of the pubic bones and the pubic arch are positioned in a nearly horizontal plane facing the ground.

Fig. 5.9 Orientation of the pelvis (anatomical position).
Gender differences
The pelvises of women and men differ in a number of ways, many of which have to do with the passing of a baby through a woman’s pelvic cavity during childbirth.
 The pelvic inlet in women is circular (Fig. 5.10A) compared with the more heart-shaped pelvic inlet (Fig. 5.10B) in men. The more circular shape is partly caused by the less distinct promontory and broader alae in women.
The pelvic inlet in women is circular (Fig. 5.10A) compared with the more heart-shaped pelvic inlet (Fig. 5.10B) in men. The more circular shape is partly caused by the less distinct promontory and broader alae in women.

 The angle formed by the two arms of the pubic arch is larger in women (80° to 85°) than it is in men (50° to 60°) (Fig. 5.10).
The angle formed by the two arms of the pubic arch is larger in women (80° to 85°) than it is in men (50° to 60°) (Fig. 5.10).
 The ischial spines generally do not project as far medially into the pelvic cavity in women as they do in men.
The ischial spines generally do not project as far medially into the pelvic cavity in women as they do in men.True pelvis
The true pelvis is cylindrical and has an inlet, a wall, and an outlet. The inlet is open, whereas the pelvic floor closes the outlet and separates the pelvic cavity, above, from the perineum, below.
Pelvic inlet
The pelvic inlet is the circular opening between the abdominal cavity and the pelvic cavity through which structures traverse between the abdomen and pelvic cavity. It is completely surrounded by bones and joints (Fig. 5.11). The promontory of the sacrum protrudes into the inlet, forming its posterior margin in the midline. On either side of the promontory, the margin is formed by the alae of the sacrum. The margin of the pelvic inlet then crosses the sacro-iliac joint and continues along the linea terminalis (i.e., the arcuate line, the pecten pubis, or pectineal line, and the pubic crest) to the pubic symphysis.
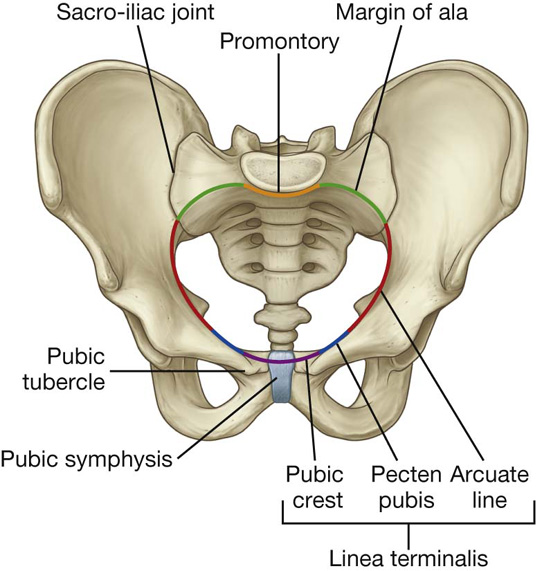
Fig. 5.11 Pelvic inlet.
Pelvic wall
The walls of the pelvic cavity consist of the sacrum, the coccyx, the pelvic bones inferior to the linea terminalis, two ligaments, and two muscles.
Clinical app
Pelvic fracture
The pelvis can be viewed as a series of anatomical rings. There are three bony rings and four fibro-osseous rings. The major bony pelvic ring consists of parts of the sacrum, ilium, and pubis, which forms the pelvic inlet. Two smaller subsidiary bony rings are the obturator foraminae. The greater and lesser sciatic foraminae, formed by the greater and lesser sciatic notches and the sacrospinous and sacrotuberous ligaments form the four fibro-osseous rings. It is not possible to break one side of a bony ring without breaking the other side of the ring, which in clinical terms means that if a fracture is demonstrated on one side, a second fracture should always be suspected.
Ligaments of the pelvic wall
The sacrospinous and sacrotuberous ligaments (Fig. 5.12A) are major components of the lateral pelvic walls that help define the apertures between the pelvic cavity and adjacent regions through which structures pass.

 The smaller of the two, the sacrospinous ligament, is triangular, with its apex attached to the ischial spine and its base attached to the related margins of the sacrum and the coccyx (Fig. 5.12A).
The smaller of the two, the sacrospinous ligament, is triangular, with its apex attached to the ischial spine and its base attached to the related margins of the sacrum and the coccyx (Fig. 5.12A).
 The sacrotuberous ligament is also triangular and is superficial to the sacrospinous ligament. Its base has a broad attachment that extends from the posterior superior iliac spine of the pelvic bone, along the dorsal aspect and the lateral margin of the sacrum, and onto the dorsolateral surface of the coccyx. Laterally, the apex of the ligament is attached to the medial margin of the ischial tuberosity (Fig. 5.12A).
The sacrotuberous ligament is also triangular and is superficial to the sacrospinous ligament. Its base has a broad attachment that extends from the posterior superior iliac spine of the pelvic bone, along the dorsal aspect and the lateral margin of the sacrum, and onto the dorsolateral surface of the coccyx. Laterally, the apex of the ligament is attached to the medial margin of the ischial tuberosity (Fig. 5.12A).
These ligaments stabilize the sacrum on the pelvic bones by resisting the upward tilting of the inferior aspect of the sacrum (Fig. 5.12B). They also convert the greater and lesser sciatic notches of the pelvic bone into foramina (Fig. 5.12A, B).
 The greater sciatic foramen lies superior to the sacrospinous ligament and the ischial spine.
The greater sciatic foramen lies superior to the sacrospinous ligament and the ischial spine.
 The lesser sciatic foramen lies inferior to the ischial spine and sacrospinous ligament between the sacrospinous and sacrotuberous ligaments.
The lesser sciatic foramen lies inferior to the ischial spine and sacrospinous ligament between the sacrospinous and sacrotuberous ligaments.Muscles of the pelvic wall
Two muscles, the obturator internus and the piriformis, contribute to the lateral walls of the pelvic cavity. These muscles originate in the pelvic cavity but attach peripherally to the femur (Table 5.1, Fig. 5.13).
Table 5.1 Muscles of the pelvic walls (spinal segments in bold are the major segments innervating the muscle)


Fig. 5.13 Obturator internus and piriformis muscles (medial view of right side of pelvis).
Apertures in the pelvic wall
Each lateral pelvic wall has three major apertures through which structures pass between the pelvic cavity and other regions (Fig. 5.14):
 the obturator canal,
the obturator canal, the greater sciatic foramen, and
the greater sciatic foramen, and
 the lesser sciatic foramen.
the lesser sciatic foramen.
Fig. 5.14 Apertures in the pelvic wall.
At the top of the obturator foramen is the obturator canal, which is bordered by the obturator membrane, the associated obturator muscles, and the superior pubic ramus (Fig. 5.14). The obturator nerve and vessels pass from the pelvic cavity to the thigh through this canal.
The greater sciatic foramen is a major route of communication between the pelvic cavity and the lower limb (Fig. 5.14). It is formed by the greater sciatic notch in the pelvic bone, the sacrotuberous and the sacrospinous ligaments, and the spine of the ischium.
The piriformis muscle passes through the greater sciatic foramen, dividing it into two parts.
 The superior gluteal nerves and vessels pass through the foramen above the piriformis.
The superior gluteal nerves and vessels pass through the foramen above the piriformis.
 Passing through the foramen below the piriformis are the inferior gluteal nerves and vessels, the sciatic nerve, the pudendal nerve, the internal pudendal vessels, the posterior femoral cutaneous nerves, and the nerves to the obturator internus and quadratus femoris muscles.
Passing through the foramen below the piriformis are the inferior gluteal nerves and vessels, the sciatic nerve, the pudendal nerve, the internal pudendal vessels, the posterior femoral cutaneous nerves, and the nerves to the obturator internus and quadratus femoris muscles.The lesser sciatic foramen is formed by the lesser sciatic notch of the pelvic bone, the ischial spine, the sacrospinous ligament, and the sacrotuberous ligament (Fig. 5.14). The tendon of the obturator internus muscle passes through this foramen to enter the gluteal region of the lower limb.
Because the lesser sciatic foramen is positioned below the attachment of the pelvic floor, it acts as a route of communication between the perineum and the gluteal region. The pudendal nerve and internal pudendal vessels pass between the pelvic cavity (above the pelvic floor) and the perineum (below the pelvic floor), by first passing out of the pelvic cavity through the greater sciatic foramen, then looping around the ischial spine and sacrospinous ligament to pass through the lesser sciatic foramen to enter the perineum.
Pelvic outlet
The pelvic outlet is diamond shaped, with the anterior part of the diamond defined predominantly by bone and the posterior part mainly by ligaments (Fig. 5.15). In the midline anteriorly, the boundary of the pelvic outlet is the pubic symphysis.

Fig. 5.15 Pelvic outlet.
From the ischial tuberosities, the boundaries continue posteriorly and medially along the sacrotuberous ligament on both sides to the coccyx.
Terminal parts of the urinary and gastrointestinal tracts and the vagina pass through the pelvic outlet.
Clinical app
Pelvic measurements in obstetrics
Accurate measurements of a women’s pelvic inlet and outlet can help in predicting the likelihood of a successful vaginal delivery during childbirth. These measurements include:
 the sagittal inlet (between the promontory and the top of the pubic symphysis);
the sagittal inlet (between the promontory and the top of the pubic symphysis);
 the maximum transverse diameter of the inlet;
the maximum transverse diameter of the inlet;
 the bispinous outlet (the distance between ischial spines); and
the bispinous outlet (the distance between ischial spines); and
 the sagittal outlet (the distance between the tip of the coccyx and the inferior margin of the pubic symphysis).
the sagittal outlet (the distance between the tip of the coccyx and the inferior margin of the pubic symphysis).The area enclosed by the boundaries of the pelvic outlet and below the pelvic floor is the perineum.
Pelvic floor
The pelvic floor is formed by the pelvic diaphragm and, in the anterior midline, the perineal membrane and the muscles in the deep perineal pouch. The pelvic diaphragm is formed by the levator ani and the coccygeus muscles from both sides. The pelvic floor separates the pelvic cavity, above, from the perineum, below.
The pelvic diaphragm
The pelvic diaphragm is the muscular part of the pelvic floor. Shaped like a bowl or funnel and attached superiorly to the pelvic walls, it consists of the levator ani and the coccygeus muscles (Table 5.2, Fig. 5.16).
Table 5.2 Muscles of the pelvic diaphragm


Fig. 5.16 Pelvic diaphragm.
The pelvic diaphragm’s circular line of attachment to the cylindrical pelvic wall passes, on each side, between the greater sciatic foramen and the lesser sciatic foramen. Thus:
 the greater sciatic foramen is situated above the level of the pelvic floor and is a route of communication between the pelvic cavity and the gluteal region of the lower limb; and
the greater sciatic foramen is situated above the level of the pelvic floor and is a route of communication between the pelvic cavity and the gluteal region of the lower limb; and the lesser sciatic foramen is situated below the pelvic floor, providing a route of communication between the gluteal region of the lower limb and the perineum.
the lesser sciatic foramen is situated below the pelvic floor, providing a route of communication between the gluteal region of the lower limb and the perineum.The two levator ani muscles originate from each side of the pelvic wall, course medially and inferiorly, and join together in the midline. The attachment to the pelvic wall follows the circular contour of the wall and includes (Fig. 5.16):
 the posterior aspect of the body of the pubic bone,
the posterior aspect of the body of the pubic bone,
 a linear thickening called the tendinous arch in the fascia covering the obturator internus muscle, and
a linear thickening called the tendinous arch in the fascia covering the obturator internus muscle, and the spine of the ischium.
the spine of the ischium.At the midline, the muscles blend together posterior to the vagina in women and around the anal aperture in both sexes. Posterior to the anal aperture, the muscles come together as a ligament or raphe called the anococcygeal ligament (anococcygeal body) and attaches to the coccyx (Fig. 5.16). Anteriorly, the muscles are separated by a U-shaped defect or gap termed the urogenital hiatus. The margins of this hiatus merge with the walls of the associated viscera and with muscles in the deep perineal pouch below. The hiatus allows the urethra (in both men and women), and the vagina (in women), to pass through the pelvic diaphragm (Fig. 5.16).
The levator ani muscles are divided into at least three collections of muscle fibers, based on site of origin and relationship to viscera in the midline: the pubococcygeus, the puborectalis, and the iliococcygeus muscles (Fig. 5.16).
 The pubococcygeus originates from the body of the pubis and courses posteriorly to attach along the midline as far back as the coccyx. This part of the muscle is further subdivided on the basis of association with structures in the midline into the puboprostaticus (levator prostatae), the pubovaginalis, and the puboanalis muscles.
The pubococcygeus originates from the body of the pubis and courses posteriorly to attach along the midline as far back as the coccyx. This part of the muscle is further subdivided on the basis of association with structures in the midline into the puboprostaticus (levator prostatae), the pubovaginalis, and the puboanalis muscles. A second major collection of muscle fibers, the puborectalis portion of the levator ani muscles, originates, in association with the pubococcygeus muscle, from the pubis and passes inferiorly on each side to form a sling around the terminal part of the gastrointestinal tract. This muscular sling maintains an angle or flexure, called the perineal flexure, at the anorectal junction. This angle functions as part of the mechanism that keeps the end of the gastrointestinal system closed.
A second major collection of muscle fibers, the puborectalis portion of the levator ani muscles, originates, in association with the pubococcygeus muscle, from the pubis and passes inferiorly on each side to form a sling around the terminal part of the gastrointestinal tract. This muscular sling maintains an angle or flexure, called the perineal flexure, at the anorectal junction. This angle functions as part of the mechanism that keeps the end of the gastrointestinal system closed. The final part of the levator ani muscle is the iliococcygeus. This part of the muscle originates from the fascia that covers the obturator internus muscle. It joins the same muscle on the other side in the midline to form a ligament or raphe that extends from the anal aperture to the coccyx.
The final part of the levator ani muscle is the iliococcygeus. This part of the muscle originates from the fascia that covers the obturator internus muscle. It joins the same muscle on the other side in the midline to form a ligament or raphe that extends from the anal aperture to the coccyx.The levator ani muscles help support the pelvic viscera and maintain closure of the rectum and vagina.
Clinical app
Defecation
At the beginning of defecation, closure of the larynx stabilizes the diaphragm and intra-abdominal pressure is increased by contraction of abdominal wall muscles. As defecation proceeds, the puborectalis muscle surrounding the anorectal junction relaxes, which straightens the anorectal angle. Both the internal and the external anal sphincters also relax to allow feces to move through the anal canal. Normally, the puborectal sling maintains an angle of about 90° between the rectum and the anal canal and acts as a “pinch valve” to prevent defecation. When the puborectalis muscle relaxes, the anorectal angle increases to about 130° to 140°.
The fatty tissue of the ischio-anal fossa allows for changes in the position and size of the anal canal and anus during defecation. During evacuation, the anorectal junction moves down and back and the pelvic floor usually descends slightly.
During defecation, the circular muscles of the rectal wall undergo a wave of contraction to push feces toward the anus. As feces emerge from the anus, the longitudinal muscles of the rectum and levator ani bring the anal canal back up, the feces are expelled, and the anus and rectum return to their normal positions.
The perineal membrane and deep perineal pouch
The perineal membrane is a thick fascial, triangular structure attached to the bony framework of the pubic arch (Fig. 5.17A). It is oriented in the horizontal plane and has a free posterior margin. Anteriorly, there is a small gap between the membrane and the inferior pubic ligament (a ligament associated with the pubic symphysis).

Fig. 5.17 Perineal membrane and deep perineal pouch. A. Inferior view. B. Superolateral view. C. Medial view.
The perineal membrane is related above to a thin space called the deep perineal pouch (deep perineal space) (Fig. 5.17B), which contains a layer of skeletal muscle and various neurovascular elements.
The deep perineal pouch is open above and is not separated from more superior structures by a distinct layer of fascia. The parts of perineal membrane and structures in the deep perineal pouch, enclosed by the urogenital hiatus above, therefore contribute to the pelvic floor and support elements of the urogenital system in the pelvic cavity, even though the perineal membrane and deep perineal pouch are usually considered parts of the perineum.
The perineal membrane and adjacent pubic arch provide attachment for the roots of the external genitalia and the muscles associated with them (Fig. 5.17C).
The urethra penetrates vertically through a circular hiatus in the perineal membrane as it passes from the pelvic cavity, above, to the perineum, below. In women, the vagina also passes through a hiatus in the perineal membrane just posterior to the urethral hiatus.
Within the deep perineal pouch, a sheet of skeletal muscle functions as a sphincter, mainly for the urethra, and as a stabilizer of the posterior edge of the perineal membrane (Table 5.3, Fig. 5.18).
Table 5.3 Muscles within the deep perineal pouch


Fig. 5.18 Muscles in the deep perineal pouch. A. In women. B. In men.
 Anteriorly, a group of muscle fibers surround the urethra and collectively form the external urethral sphincter (Fig. 5.18).
Anteriorly, a group of muscle fibers surround the urethra and collectively form the external urethral sphincter (Fig. 5.18).
 Two additional groups of muscle fibers are associated with the urethra and vagina in women (Fig. 5.18A). One group forms the sphincter urethrovaginalis, which surrounds the urethra and vagina as a unit. The second group forms the compressor urethrae, on each side, which originate from the ischiopubic rami and meet anterior to the urethra. Together with the external urethral sphincter, the sphincter urethrovaginalis and compressor urethrae facilitate closing of the urethra.
Two additional groups of muscle fibers are associated with the urethra and vagina in women (Fig. 5.18A). One group forms the sphincter urethrovaginalis, which surrounds the urethra and vagina as a unit. The second group forms the compressor urethrae, on each side, which originate from the ischiopubic rami and meet anterior to the urethra. Together with the external urethral sphincter, the sphincter urethrovaginalis and compressor urethrae facilitate closing of the urethra.
 In both men and women, a deep transverse perineal muscle on each side parallels the free margin of the perineal membrane and joins with its partner at the midline. These muscles are thought to stabilize the position of the perineal body, which is a midline structure along the posterior edge of the perineal membrane.
In both men and women, a deep transverse perineal muscle on each side parallels the free margin of the perineal membrane and joins with its partner at the midline. These muscles are thought to stabilize the position of the perineal body, which is a midline structure along the posterior edge of the perineal membrane.Perineal body
The perineal body is an ill-defined but important connective tissue structure into which muscles of the pelvic floor and the perineum attach (Fig. 5.19). It is positioned in the midline along the posterior border of the perineal membrane, to which it attaches. The posterior end of the urogenital hiatus in the levator ani muscles is also connected to it.

Fig. 5.19 Perineal body.
The deep transverse perineal muscles intersect at the perineal body; in women, the sphincter urethrovaginalis also attaches to the perineal body. Other muscles that connect to the perineal body include the external anal sphincter, the superficial transverse perineal muscles, and the bulbospongiosus muscles of the perineum.
Clinical app
Episiotomy
During childbirth the perineal body may be stretched and torn. Traditionally it was felt that if a perineal tear is likely, the obstetrician may proceed with an episiotomy. This is a procedure in which an incision is made in the perineal body to allow the head of the fetus to pass through the vagina. There are two types of episiotomies: a median episiotomy cuts through the perineal body, while a mediolateral episiotomy is an incision 45° from the midline. The maternal benefits of this procedure have been thought to be less trauma to the perineum and decreased pelvic floor dysfunction. However, more recent evidence suggests that an episiotomy should not be performed routinely. Review of data has failed to show a decrease in pelvic floor damage with routine use of episiotomies.
Viscera
The pelvic viscera include parts of the gastrointestinal system, the urinary system, and the reproductive system. The viscera are arranged in the midline, from front to back; the neurovascular supply is through branches that pass medially from vessels and nerves associated with the pelvic walls.
Gastrointestinal system
Pelvic parts of the gastrointestinal system consist mainly of the rectum and the anal canal, although the terminal part of the sigmoid colon is also in the pelvic cavity (Fig. 5.20).


Fig. 5.20 Rectum and anal canal. A. Left pelvic bone removed. B. Longitudinal section.
Rectum
The rectum is continuous:
 above, with the sigmoid colon at about the level of vertebra SIII; and
above, with the sigmoid colon at about the level of vertebra SIII; and
 below, with the anal canal as this structure penetrates the pelvic floor and passes through the perineum to end as the anus.
below, with the anal canal as this structure penetrates the pelvic floor and passes through the perineum to end as the anus.The rectum, the most posterior element of the pelvic viscera, is immediately anterior to, and follows the concave contour of the sacrum (Fig. 5.20A).
The anorectal junction is pulled forward (perineal flexure) by the action of the puborectalis part of the levator ani muscle, so the anal canal moves in a posterior direction as it passes inferiorly through the pelvic floor.
In addition to conforming to the general curvature of the sacrum in the anteroposterior plane, the rectum has three lateral curvatures; the upper and lower curvatures to the right and the middle curvature to the left. The lower part of the rectum is expanded to form the rectal ampulla. Finally, unlike the colon, the rectum lacks distinct taeniae coli muscles, omental appendices, and sacculations (haustra of the colon).
Digital rectal examination
A digital rectal examination (DRE) is performed by placing the gloved and lubricated index finger into the rectum through the anus. The anal mucosa can be palpated for abnormal masses, and in women, the posterior wall of the vagina and the cervix can be palpated. In men, the prostate can be evaluated for any extraneous nodules or masses.
Anal canal
The anal canal begins at the terminal end of the rectal ampulla where it narrows at the pelvic floor (Fig. 5.20B). It terminates as the anus after passing through the perineum. As it passes through the pelvic floor, the anal canal is surrounded along its entire length by the internal and external anal sphincters, which normally keep it closed (Fig. 5.20B).
The lining of the anal canal bears a number of characteristic structural features that reflect the approximate position of the anococcygeal membrane in the fetus (which closes the terminal end of the developing gastrointestinal system in the fetus) and the transition from gastrointestinal mucosa to skin in the adult (Fig. 5.20B).
 The upper part of the anal canal is lined by mucosa similar to that lining the rectum and is distinguished by a number of longitudinally oriented folds known as anal columns, which are united inferiorly by crescentic folds termed anal valves. Superior to each valve is a depression termed an anal sinus. The anal valves together form a circle around the anal canal at a location known as the pectinate line, which marks the approximate position of the anal membrane in the fetus.
The upper part of the anal canal is lined by mucosa similar to that lining the rectum and is distinguished by a number of longitudinally oriented folds known as anal columns, which are united inferiorly by crescentic folds termed anal valves. Superior to each valve is a depression termed an anal sinus. The anal valves together form a circle around the anal canal at a location known as the pectinate line, which marks the approximate position of the anal membrane in the fetus. Inferior to the pectinate line is a transition zone known as the anal pecten, which is lined by nonkeratinized stratified squamous epithelium. The anal pecten ends inferiorly at the anocutaneous line (“white line”), or where the lining of the anal canal becomes true skin.
Inferior to the pectinate line is a transition zone known as the anal pecten, which is lined by nonkeratinized stratified squamous epithelium. The anal pecten ends inferiorly at the anocutaneous line (“white line”), or where the lining of the anal canal becomes true skin.Clinical app
Carcinoma of the colon and rectum
Carcinoma of the colon and rectum (colorectum) is a common disease.
Given the position of the colon and rectum in the abdominopelvic cavity and its proximity to other organs, it is extremely important to accurately stage colorectal tumors: a tumor in the pelvis, for example, could invade the uterus or bladder.
Urinary system
The pelvic parts of the urinary system consist of the terminal parts of the ureters, the bladder, and the proximal part of the urethra (Fig. 5.21).

Fig. 5.21 Pelvic parts of the urinary system.
Ureters
The ureters enter the pelvic cavity from the abdomen by passing through the pelvic inlet (Fig. 5.21). On each side, the ureter crosses the pelvic inlet and enters the pelvic cavity in the area anterior to the bifurcation of the common iliac artery. From this point, it continues along the pelvic wall and floor to join the base of the bladder.
In the pelvis, the ureter is crossed by:
 the ductus deferens in men, and
the ductus deferens in men, and
 the uterine artery in women.
the uterine artery in women.Bladder
The bladder is the most anterior element of the pelvic viscera. Although it is entirely situated in the pelvic cavity when empty, it expands superiorly into the abdominal cavity when full (see Fig. 5.21).
The empty bladder is shaped like a three-sided pyramid that has tipped over to lie on one of its margins (see Fig. 5.22A). It has an apex, a base, a superior surface, and two inferolateral surfaces (see Fig. 5.22A).
 The apex of the bladder is directed toward the top of the pubic symphysis; a structure known as the median umbilical ligament (a remnant of the embryological urachus that contributes to the formation of the bladder) continues from it superiorly up the anterior abdominal wall to the umbilicus.
The apex of the bladder is directed toward the top of the pubic symphysis; a structure known as the median umbilical ligament (a remnant of the embryological urachus that contributes to the formation of the bladder) continues from it superiorly up the anterior abdominal wall to the umbilicus. The base of the bladder is shaped like an inverted triangle and faces posteroinferiorly. The two ureters enter the bladder at each of the upper corners of the base, and the urethra drains inferiorly from the lower corner of the base (Fig. 5.22A, B). Inside, the mucosal lining on the base of the bladder is smooth and firmly attached to the underlying smooth muscle coat of the wall—unlike elsewhere in the bladder where the mucosa is folded and loosely attached to the wall. The smooth triangular area between the openings of the ureters and urethra on the inside of the bladder is known as the trigone (Fig. 5.22B).
The base of the bladder is shaped like an inverted triangle and faces posteroinferiorly. The two ureters enter the bladder at each of the upper corners of the base, and the urethra drains inferiorly from the lower corner of the base (Fig. 5.22A, B). Inside, the mucosal lining on the base of the bladder is smooth and firmly attached to the underlying smooth muscle coat of the wall—unlike elsewhere in the bladder where the mucosa is folded and loosely attached to the wall. The smooth triangular area between the openings of the ureters and urethra on the inside of the bladder is known as the trigone (Fig. 5.22B).
 The inferolateral surfaces of the bladder are cradled between the levator ani muscles of the pelvic diaphragm and the adjacent obturator internus muscles above the attachment of the pelvic diaphragm. The superior surface is slightly domed when the bladder is empty; it balloons upward as the bladder fills.
The inferolateral surfaces of the bladder are cradled between the levator ani muscles of the pelvic diaphragm and the adjacent obturator internus muscles above the attachment of the pelvic diaphragm. The superior surface is slightly domed when the bladder is empty; it balloons upward as the bladder fills.
The neck of the bladder surrounds the origin of the urethra at the point where the two inferolateral surfaces and the base intersect (see Fig. 5.21).
The neck is the most inferior part of the bladder and also the most “fixed” part. It is anchored into position by a pair of tough fibromuscular bands, which connect the neck and pelvic part of the urethra to the posteroinferior aspect of each pubic bone.
 In women, these fibromuscular bands are termed pubovesical ligaments (Fig. 5.23A). Together with the perineal membrane and associated muscles, the levator ani muscles, and the pubic bones, these ligaments help support the bladder.
In women, these fibromuscular bands are termed pubovesical ligaments (Fig. 5.23A). Together with the perineal membrane and associated muscles, the levator ani muscles, and the pubic bones, these ligaments help support the bladder.

 In men, the paired fibromuscular bands are known as puboprostatic ligaments because they blend with the fibrous capsule of the prostate, which surrounds the neck of the bladder and adjacent part of the urethra (Fig. 5.23B).
In men, the paired fibromuscular bands are known as puboprostatic ligaments because they blend with the fibrous capsule of the prostate, which surrounds the neck of the bladder and adjacent part of the urethra (Fig. 5.23B).
Although the bladder is considered to be pelvic in the adult, it has a higher position in children. At birth, the bladder is almost entirely abdominal; the urethra begins approximately at the upper margin of the pubic symphysis. With age, the bladder descends until after puberty when it assumes the adult position.
Clinical app
Bladder cancer
Bladder cancer is the most common tumor of the urinary tract and is usually a disease of the sixth and seventh decades, although there is an increasing trend for younger patients to develop this disease.
Bladder tumors may spread through the bladder wall and invade local structures, including the rectum, uterus (in women), and the lateral walls of the pelvic cavity. Prostatic involvement is not uncommon in male patients.
Large bladder tumors may produce complications, including invasion and obstruction of the ureters. Ureteric obstruction can then obstruct the kidneys and induce kidney failure.
Bladder stones
In some patients, small calculi (stones) form in the kidneys. These may pass down the ureter, causing ureteric obstruction, and into the bladder, where insoluble salts further precipitate on these small calculi to form larger calculi. Often, these patients develop (or may already have) problems with bladder emptying, which leaves residual urine in the bladder. This urine may become infected and alter the pH of the urine, permitting further precipitation of insoluble salts.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


