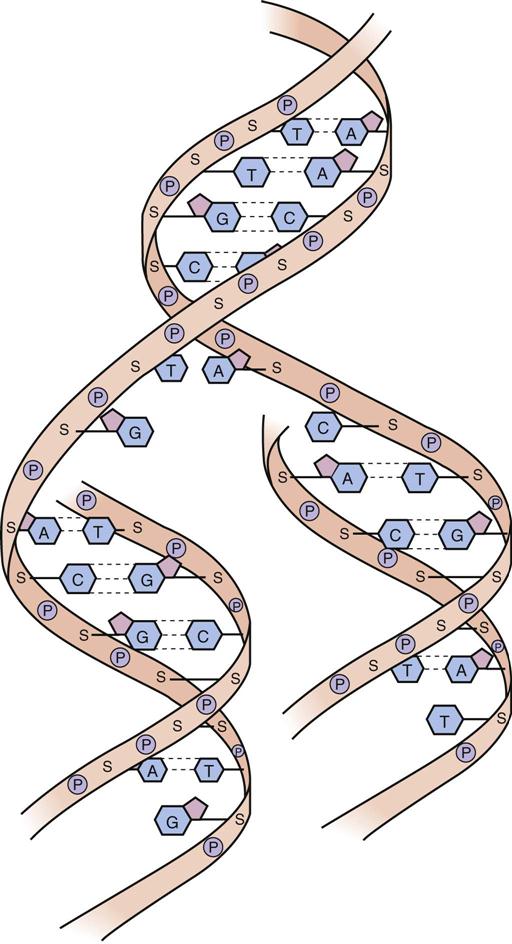
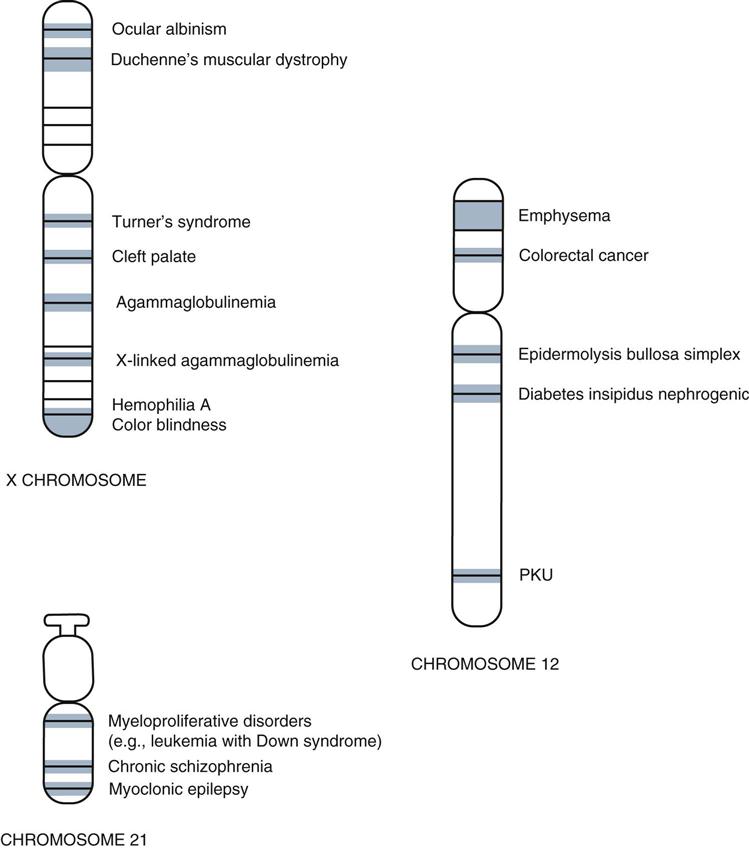
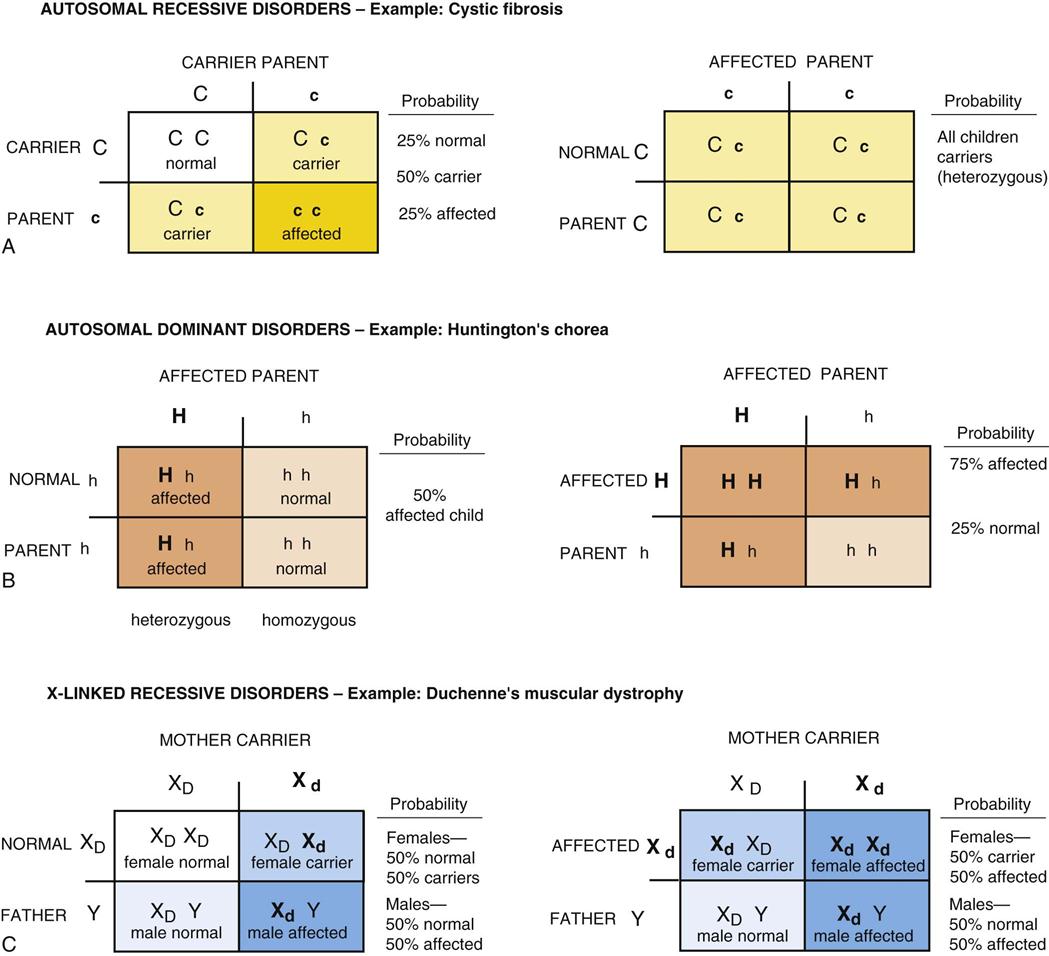
After studying this chapter, the student is expected to: 1. Define congenital, genetic, chromosomal, developmental, and multifactorial disorders. 3. Explain the common causes of developmental disorders and their relationship to fetal development. 4. Discuss the importance of proteomics in the development of treatments for genetic disorders. 5. Describe the benefits and risks of genetic screening programs and prenatal testing. 6. Discuss the purposes of genetic engineering and current concerns. allele amniocentesis anomaly autosomes expression gene penetration genotype heterozygous homozygous incomplete dominant karyotype meiosis mitosis mutation neonates organogenesis phenotype polygenic teratogenic trisomy Genetic information for each cell is stored on chromosomes, of which there are 23 pairs in each human cell. Twenty-two pairs are autosomes, and they are numbered when arranged by size and shape in a diagnostic graphic termed a karyotype (Fig. 21-1). The 23rd pair consists of the pair of sex chromosomes; males have XY, and females have XX chromosomes. A male child receives the X chromosome from his mother and a Y chromosome from his father. A female child receives an X chromosome from each parent. During meiosis in humans, each sperm and each ovum receive only 23 chromosomes, that is, one chromosome from each pair. When the ovum is fertilized by the sperm, the resulting zygote has 46 chromosomes, or 23 pairs containing an assortment of genetic information inherited from the parents. Because so many combinations of genes are possible, it is most unlikely that any two persons other than identical twins will have the same genes and sequence of DNA (deoxyribonucleic acid). Therefore, DNA is considered a unique identifying characteristic for an individual (Fig. 21-2). Chromosomes are made up of many genes, which are matched for a function (allele) at a specific location on the paired chromosomes. A gene is a DNA “file” that contains information about protein synthesis in the cell. All cells in an individual’s body contain the same chromosomes and genes for the same traits (genotype), although not all genes are active in each cell. This limited activity is referred to as gene expression. Usually only a small group of genes is controlling protein synthesis in a particular cell at any particular time; gene expression is related to the cell’s specific function. Genes are composed of DNA strands, which determine the function of all cells in the body. RNA (ribonucleic acid) provides the communication link with DNA during the actual synthesis of proteins and helps to maintain control of cell activity. During embryonic and fetal development, when cells are undergoing mitosis (somatic cell division), the chromosomes replicate, and each daughter cell receives a copy of DNA identical to that in the parent cell. Therefore the same genetic information is carried forward. Changes can occur because of an error in the process of meiosis or mitosis, but these are relatively rare. Such a mutation or alteration in genetic material may be spontaneous or may result from exposure to harmful substances such as radiation, chemicals, or drugs. Research has been directed toward “mapping” all the genes on particular chromosomes and identifying the role of each gene (Fig. 21-3). The International Human Genome Project (HGP) is a worldwide project conducted by geneticists that aims to identify and map all the genes on every chromosome. The first stage was completed in 2003, listing millions of base pairs in the human DNA strand. Not all genes have been sequenced in the genome to date. Although it was originally estimated that there are a total of 50,000 to 100,000 protein-coding genes in the human chromosome, current knowledge has reduced this figure to approximately 20,000 to 25,000. In addition, some DNA sequences act as regulators or “on/off switches” for gene activity, whereas other sequences have unknown functions and have been termed junk DNA. Repeats of base pairs in this so-called junk DNA have been identified as abnormalities leading to disease. As more information becomes available, it becomes easier to decode the DNA sequences and clarify problem areas. Now the refining, verifying, and analysis of data, and identification and functional determination of individual genes continue. When a specific gene for a pathologic condition is identified, a DNA analysis follows, leading, to the development of a simple blood test to screen individuals for the presence of that specific gene. The genetic link to a disease may lead to improved treatment, a cure, or prevention. Many genetic conditions have been determined so far, as well as a large number of genes related to cancer and cardiovascular disease. Every year, a few more disease-causing genes are located. For some disorders, more than one gene may be responsible; for example, each of four different genes causes four different types of Fanconi’s anemia. Genes control all physical characteristics, such as eye color or color blindness, and all metabolic processes. The effects, such as shade of eye color, vary with the gene penetration or frequency of expression of the gene among individuals carrying the gene. Inheritance of many genes for both normal characteristics and disease characteristics follows specific patterns of inheritance termed Mendelian laws or patterns. Mendelian inheritance includes recessive and dominant patterns and results can be predicted using algebra or Punnett squares (Fig. 21-4). Traditionally recessive genes are represented by lowercase letters and dominant genes by capital letters. Many traits such as eye color and blood type are polygenic, meaning that more than one allele determines the genotype and thus the phenotype of the individual. 21-1 Think about Congenital anomalies refer to disorders present at birth. Such defects include genetic or inherited disorders as well as developmental disorders. • Genetic disorders may result from a single-gene trait or from a chromosomal defect, or they may be multifactorial. A few examples are listed in Box 21-1. Developmental defects may be spontaneous errors or may result from exposure to environmental factors in utero. The DNA of the embryonic cells may be altered easily because rapid mitosis and differentiation take place during the first months of embryonic development. During this period replication of DNA occurs frequently and the possibility of damage is significant. Maternal nutrition may also affect development. For example, low folic acid levels in the mother are a factor in the occurrence of spina bifida in the embryo. Genetic disorders have social and psychological implications. Decisions about whether or not to bear children when there is a risk of such disorders frequently create ethical dilemmas for families. Social implications of the birth of a child with a genetic disease who requires specialized care and treatment is also of concern. Parents often have difficulty in adjusting to the birth of a child with an unanticipated disorder and may need continued assistance with the care of the child and any associated feelings of guilt. Social resources for the care and education of children who are disabled by a genetic disorder may not be readily available in the community or may be prohibitively expensive.
Congenital and Genetic Disorders
Learning Objectives
Key Terms
Review of Genetic Control
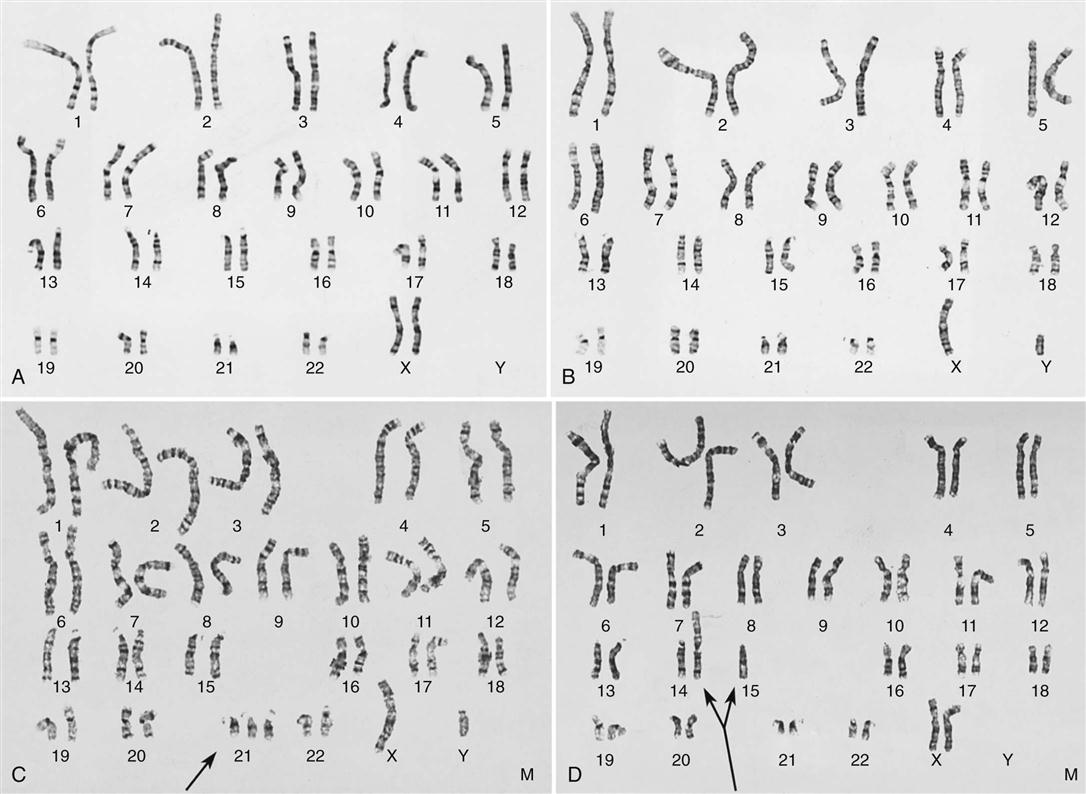
A, Normal female (46, XX). B, Normal male (46, XY). C, Male with Down syndrome or trisomy 21 (47, XY, + 21). D, Female with translocation involving chromosomes 14 and 15 (45, XX, t (14q15q) ). (Courtesy of Cytogenetics Laboratory, North York General Hospital, Toronto, Ontario, Canada.)

Congenital Anomalies
Congenital and Genetic Disorders