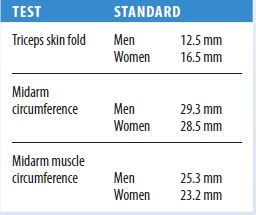
Standard anthropometric measurements vary according to the patient’s age and sex and can be found in a chart of normal anthropometric values. The abridged chart below lists standard arm measurements for adult men and women.
A triceps or subscapular skinfold measurement below 60% of the standard value indicates severe depletion of fat reserves, measurement between 60% and 90% indicates moderate to mild depletion, and above 90% indicates significant fat reserves. A midarm circumference of less than 90% of the standard value indicates caloric deprivation; greater than 90% indicates adequate or ample muscle and fat. A midarm muscle circumference of less than 90% indicates protein depletion; greater than 90% indicates adequate or ample protein reserves.
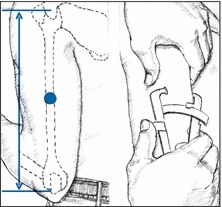
To measure the triceps skin fold, locate the midpoint of the patient’s upper arm, using a nonstretch tape measure. Mark the midpoint with a felt-tip pen. Then, grasp the skin with your thumb and forefinger about 1 cm above the midpoint. Place the calipers at the midpoint, and squeeze them for about 3 seconds. Record the measurement registered on the handle gauge to the nearest 0.5 mm. Take two more readings, and average all three to compensate for any measurement error.
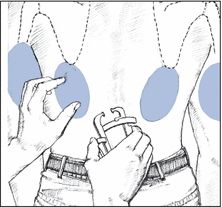
To measure the subscapular skin fold, use your thumb and forefinger to grasp the skin just below the angle of the scapula, in line with the natural cleavage of the skin. Apply the calipers, and proceed as you would when measuring the triceps skin fold. Both subscapular and triceps skinfold measurements are reliable measurements of fat loss or gain during hospitalization.
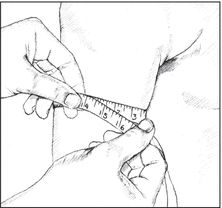
To measure midarm circumference, return to the midpoint you marked on the patient’s upper arm. Then, use a tape measure to determine the arm circumference at this point. This measurement reflects both skeletal muscle and adipose tissue mass and helps evaluate protein and calorie reserves. To calculate midarm muscle circumference, multiply the triceps skinfold thickness (in centimeters) by 3.143, and subtract this figure from the midarm circumference. Midarm muscle circumference reflects muscle mass alone, providing a more sensitive index of protein reserves.
- Metabolic syndrome. Excessive weight gain, particularly the accumulation of fat around the midsection or a disproportionate waist-hip ratio (apple shape), is a risk factor of this disease. Other risk factors include increased blood pressure, elevated glucose and insulin levels, and abnormal cholesterol, triglyceride, and high-density lipoprotein levels. It’s estimated that more than 50 million people in the United States have metabolic syndrome. Implementing a healthier lifestyle, incorporating better eating habits, losing weight, and increasing physical activity are ways to decrease or delay the risks associated with metabolic syndrome.
- Nephrotic syndrome. With nephrotic syndrome, weight gain results from edema. In severe cases, anasarca develops — increasing body weight up to 50%. Related effects include abdominal distention, orthostatic hypotension, and lethargy.
- Pancreatic islet cell tumor. Pancreatic islet cell tumor causes excessive hunger, which leads to weight gain. Other findings include emotional lability, weakness, malaise, fatigue, restlessness, diaphoresis, palpitations, tachycardia, visual disturbances, and syncope.
- Preeclampsia. With preeclampsia, rapid weight gain (exceeding the normal weight gain of pregnancy) may accompany nausea and vomiting, epigastric pain, elevated blood pressure, and visual blurring or double vision.
- Sheehan’s syndrome. Most common in women who experience severe obstetric hemorrhage, Sheehan’s syndrome may cause weight gain.
Other Causes
- Drugs. Corticosteroids, phenothiazines, and tricyclic antidepressants cause weight gain from fluid retention and increased appetite. Other drugs that can lead to weight gain include hormonal contraceptives, which cause fluid retention; cyproheptadine, which increases appetite; and lithium, which can induce hypothyroidism.
Special Considerations
Psychological counseling may be necessary for patients with weight gain, particularly when it results from emotional problems or when uneven weight distribution alters body image. If the patient is obese or has a cardiopulmonary disorder, any exercises should be monitored closely. Further study to rule out possible secondary causes should include serum thyroid-stimulating hormone determination and dexamethasone suppression testing. Laboratory test results of all patients ideally include cardiac risk factors: serum cholesterol, triglyceride, and glucose levels.
Patient Counseling
Discuss the importance of weight control, and provide guidance in appropriate exercise. Also, explain the importance of behavior modification and dietary compliance.
Pediatric Pointers
Weight gain in children can result from an endocrine disorder, such as hypercortisolism. Other causes include inactivity caused by Prader-Willi syndrome, Down syndrome, Werdnig-Hoffmann disease, late stages of muscular dystrophy, and severe cerebral palsy.
Nonpathologic causes include poor eating habits, sedentary recreation, and emotional problems, especially among adolescents. Regardless of the cause, discourage fad diets and provide a balanced weight loss program. The incidence of obesity is increasing among children.
Geriatric Pointers
Desired weights (associated with lowest mortality rates) increase with age.
REFERENCES
Buttaro, T. M., Tybulski, J., Bailey, P. P., & Sandberg-Cook, J. (2008). Primary care: A collaborative practice (pp. 444–447). St. Louis, MO: Mosby Elsevier.
Colyar, M. R. (2003). Well-child assessment for primary care providers. Philadelphia, PA: F.A. Davis.
Lehne, R. A. (2010). Pharmacology for nursing care (7th ed.). St. Louis, MO: Saunders Elsevier.
McCance, K. L., Huether, S. E., Brashers, V. L., & Rote, N. S. (2010). Pathophysiology: The biologic basis for disease in adults and children. Maryland Heights, MO: Mosby Elsevier.
Schuiling, K. D. (2013). Women’s gynecologic health. Burlington, MA: Jones & Bartlett Learning.
Sommers, M. S., & Brunner, L. S. (2012). Pocket diseases. Philadelphia, PA: F.A. Davis.
Weight Loss, Excessive
Weight loss can reflect decreased food intake, decreased food absorption, increased metabolic requirements, or a combination of the three. Its causes include endocrine, neoplastic, GI, and psychiatric disorders; nutritional deficiencies; infections; and neurologic lesions that cause paralysis and dysphagia. However, weight loss may accompany conditions that prevent sufficient food intake, such as painful oral lesions, ill-fitting dentures, and loss of teeth. It may be the metabolic effect of poverty, fad diets, excessive exercise, or certain drugs.
Weight loss may occur as a late sign in such chronic diseases as heart failure and renal disease. In these diseases, however, it’s the result of anorexia. (See Anorexia, pages 49 to 52.)
History and Physical Examination
Begin with a thorough diet history because weight loss almost always is caused by inadequate caloric intake. If the patient hasn’t been eating properly, try to determine why. Ask him about previous weight and if the recent loss was intentional. Be alert to lifestyle or occupational changes that may be a source of anxiety or depression. For example, has he gotten separated or divorced? Has a family member or friend died recently? Has he recently changed jobs?
Inquire about recent changes in bowel habits, such as diarrhea or bulky, floating stools. Has the patient had nausea, vomiting, or abdominal pain, which may indicate a GI disorder? Has he had excessive thirst, excessive urination, or heat intolerance, which may signal an endocrine disorder? Take a careful drug history, noting especially any use of diet pills and laxatives.
Carefully check the patient’s height and weight, and ask about his previous weight. Take his vital signs, and note his general appearance: Is he well nourished? Do his clothes fit? Is muscle wasting evident? Ask about exact weight changes (with approximate dates).
Next, examine the patient’s skin for turgor and abnormal pigmentation, especially around the joints. Does he have pallor or jaundice? Examine his mouth, including the condition of his teeth or dentures. Look for signs of infection or irritation on the roof of the mouth, and note any hyperpigmentation of the buccal mucosa. Also, check the patient’s eyes for exophthalmos and his neck for swelling; evaluate his lungs for adventitious sounds. Inspect his abdomen for signs of wasting, and palpate for masses, tenderness, and an enlarged liver.
Conventional laboratory and radiologic investigations such as complete blood count, serum albumin levels, urinalysis, chest X-ray, and upper GI series usually reveal the cause. Almost all physical causes are clinically evident during the initial evaluation. Cancer, GI disorders, and depression are the most common pathologic causes.
Medical Causes
- Adrenal insufficiency. Weight loss occurs with adrenal insufficiency, along with anorexia, weakness, fatigue, irritability, syncope, nausea, vomiting, abdominal pain, and diarrhea or constipation. Hyperpigmentation may occur at the joints, belt line, palmar creases, lips, gums, tongue, and buccal mucosa.
- Anorexia nervosa. Anorexia nervosa is a psychogenic disorder, most common in young women, and is characterized by a severe, self-imposed weight loss ranging from 10% to 50% of premorbid weight, which typically was normal or not more than 5 lb (2.3 kg) over ideal weight. Related findings include skeletal muscle atrophy, loss of fatty tissue, hypotension, constipation, dental caries, susceptibility to infection, blotchy or sallow skin, cold intolerance, hairiness on the face and body, dryness or loss of scalp hair, and amenorrhea. The patient usually demonstrates restless activity and vigor and may also have a morbid fear of becoming fat. Self-induced vomiting or use of laxatives or diuretics may lead to dehydration or to metabolic alkalosis or acidosis.
- Cancer. Weight loss is often a sign of cancer. Other findings reflect the type, location, and stage of the tumor and can include fatigue, pain, nausea, vomiting, anorexia, abnormal bleeding, and a palpable mass.
- Crohn’s disease. Weight loss occurs with chronic cramping, abdominal pain, and anorexia. Other signs and symptoms include diarrhea, nausea, fever, tachycardia, abdominal tenderness and guarding, hyperactive bowel sounds, abdominal distention, and pain. Perianal lesions and a palpable mass in the right or left lower quadrant may also be present.
- Cryptosporidiosis. Weight loss may occur with cryptosporidiosis, an opportunistic protozoan infection. Other findings include profuse watery diarrhea, abdominal cramping, flatulence, anorexia, malaise, fever, nausea, vomiting, and myalgia.
- Depression. Weight loss or weight gain may occur with severe depression, along with insomnia or hypersomnia, anorexia, apathy, fatigue, and feelings of worthlessness. Indecisiveness, incoherence, and suicidal thoughts or behavior may also occur.
- Diabetes mellitus. Weight loss may occur with diabetes mellitus, despite increased appetite. Other findings include polydipsia, weakness, fatigue, and polyuria with nocturia.
- Esophagitis. Painful inflammation of the esophagus leads to temporary avoidance of eating and subsequent weight loss. Intense pain in the mouth and anterior chest occurs, along with hypersalivation, dysphagia, tachypnea, and hematemesis. If a stricture develops, dysphagia and weight loss will recur.
- Gastroenteritis. Malabsorption and dehydration cause weight loss in gastroenteritis. The loss may be sudden in acute viral infections or reactions or gradual in parasitic infection. Other findings include poor skin turgor, dry mucous membranes, tachycardia, hypotension, diarrhea, abdominal pain and tenderness, hyperactive bowel sounds, nausea, vomiting, fever, and malaise.
- Leukemia. Acute leukemia causes progressive weight loss accompanied by severe prostration; high fever; swollen, bleeding gums; and bleeding tendencies. Dyspnea, tachycardia, palpitations, and abdominal or bone pain may occur. As the disease progresses, neurologic symptoms may eventually develop.
Chronic leukemia, which occurs insidiously in adults, causes progressive weight loss with malaise, fatigue, pallor, enlarged spleen, bleeding tendencies, anemia, skin eruptions, anorexia, and fever.
- Lymphoma. Hodgkin’s disease and non-Hodgkin’s lymphoma cause gradual weight loss. Associated findings include fever, fatigue, night sweats, malaise, hepatosplenomegaly, and lymphadenopathy. Scaly rashes and pruritus may develop.
- Pulmonary tuberculosis. Pulmonary tuberculosis causes gradual weight loss, along with fatigue, weakness, anorexia, night sweats, and low-grade fever. Other clinical effects include a cough with bloody or mucopurulent sputum, dyspnea, and pleuritic chest pain. Examination may reveal dullness on percussion, crackles after coughing, increased tactile fremitus, and amphoric breath sounds.
- Stomatitis. Inflammation of the oral mucosa (usually red, swollen, and ulcerated) in stomatitis causes weight loss due to decreased eating. Associated findings include fever, increased salivation, malaise, mouth pain, anorexia, and swollen, bleeding gums.
- Thyrotoxicosis. With thyrotoxicosis, increased metabolism causes weight loss. Other characteristic signs and symptoms include nervousness, heat intolerance, diarrhea, increased appetite, palpitations, tachycardia, diaphoresis, fine tremor, and possibly an enlarged thyroid and exophthalmos. A ventricular or atrial gallop may be heard.
Other Causes
- Drugs. Amphetamines and inappropriate dosage of thyroid preparations commonly lead to weight loss. Laxative abuse may cause a malabsorptive state that leads to weight loss. Chemotherapeutic agents cause stomatitis or nausea and vomiting, which, when severe, causes weight loss.
Special Considerations
Refer your patient for psychological counseling if weight loss negatively affects his body image. If the patient has a chronic disease, administer hyperalimentation or tube feedings to maintain nutrition and to prevent edema, poor healing, and muscle wasting. Take daily calorie counts, and weigh him weekly. Consult a nutritionist to determine an appropriate diet and nutritional supplements with adequate calories.
Patient Counseling
Provide guidance in proper diet and keeping a food diary. Instruct the patient in good oral hygiene. Provide a referral to psychological counseling, if appropriate.
Pediatric Pointers
In infants, weight loss may be caused by failure-to-thrive syndrome. In children, severe weight loss may be the first indication of diabetes mellitus. Chronic, gradual weight loss occurs in children with marasmus — nonedematous protein-calorie malnutrition.
Weight loss may also occur as a result of child abuse or neglect; an infection causing high fevers; hand-foot-and-mouth disease, which causes painful oral sores; a GI disorder causing vomiting and diarrhea; or celiac disease.
Geriatric Pointers
Some elderly patients experience mild, gradual weight loss due to changes in body composition, such as loss of height and lean body mass, and lower basal metabolic rate, leading to decreased energy requirements. Rapid, unintentional weight loss, however, is highly predictive of morbidity and mortality in the elderly. Other nondisease causes of weight loss in this group include tooth loss, difficulty chewing, and social isolation. Alcoholism may also cause weight loss.
REFERENCES
Buttaro, T. M., Tybulski, J., Bailey, P. P., & Sandberg-Cook, J. (2008). Primary care: A collaborative practice (pp. 444–447). St. Louis, MO: Mosby Elsevier.
Colyar, M. R. (2003). Well-child assessment for primary care providers. Philadelphia, PA: F.A. Davis.
Lehne, R. A. (2010). Pharmacology for nursing care (7th ed.). St. Louis, MO: Saunders Elsevier.
McCance, K. L., Huether, S. E., Brashers, V. L., & Rote, N. S. (2010). Pathophysiology: The biologic basis for disease in adults and children. Maryland Heights, MO: Mosby Elsevier.
Sommers, M. S., & Brunner, L. S. (2012). Pocket diseases. Philadelphia, PA: F.A. Davis.
Wheezing[Sibilant Rhonchi]
Wheezes are adventitious breath sounds with a high-pitched, musical, squealing, creaking, or groaning quality. They are caused by air flowing at a high velocity through a narrowed airway. When they originate in the large airways, they can be heard by placing an unaided ear over the chest wall or at the mouth. When they originate in smaller airways, they can be heard by placing a stethoscope over the anterior or posterior chest. Unlike crackles and rhonchi, wheezes can’t be cleared by coughing.
Usually, prolonged wheezing occurs during expiration when bronchi are shortened and narrowed. Causes of airway narrowing include bronchospasm; mucosal thickening or edema; partial obstruction from a tumor, a foreign body, or secretions; and extrinsic pressure, as in tension pneumothorax or goiter. With airway obstruction, wheezing occurs during inspiration.
 EMERGENCY INTERVENTIONS
EMERGENCY INTERVENTIONS
Examine the degree of the patient’s respiratory distress. Is he responsive? Is he restless, confused, anxious, or afraid? Are his respirations abnormally fast, slow, shallow, or deep? Are they irregular? Can you hear wheezing through his mouth? Does he exhibit increased use of accessory muscles; increased chest wall motion; intercostal, suprasternal, or supraclavicular retractions; stridor; or nasal flaring? Take his other vital signs, noting hypotension or hypertension and decreased oxygen saturation or an irregular, weak, rapid, or slow pulse.
Help the patient relax, administer humidified oxygen by face mask, and encourage him to take slow, deep breaths. Have endotracheal intubation and emergency resuscitation equipment readily available. Call the respiratory therapy department to supply intermittent positive pressure breathing and nebulization treatments with bronchodilators. Insert an I.V. line for administration of drugs, such as diuretics, steroids, bronchodilators, and sedatives. Perform the abdominal thrust maneuver, as indicated, for airway obstruction.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


