Pancreatic Neuroendocrine Tumor A well-circumscribed solid mass in the pancreas is typical of low-grade neuroendocrine tumors.
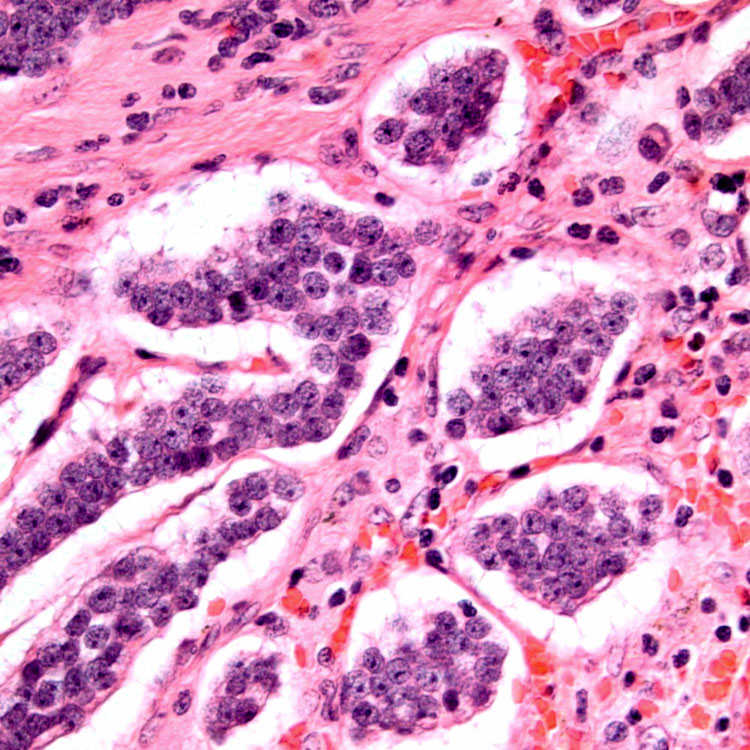
Nested Architecture The tumor cells show a nested pattern of growth. The individual tumor cells have uniform nuclei, small nucleoli, and lack prominent nuclear atypia, mitoses, or necrosis.
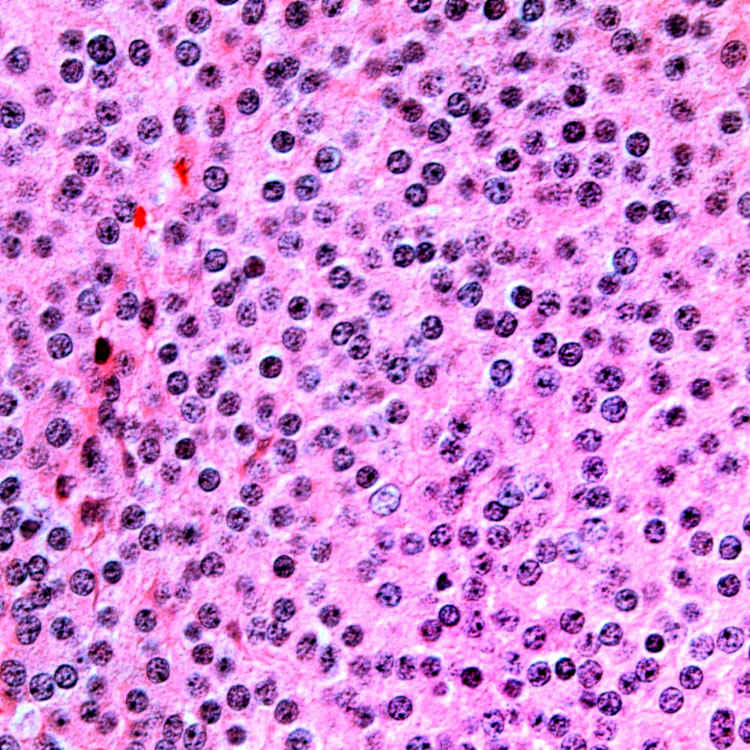
Solid Growth Pattern The solid growth pattern and round monotonous nuclei support pancreatic neuroendocrine tumors, but immunohistochemistry is required to distinguish them from solid pseudopapillary tumors and acinar cell carcinomas.
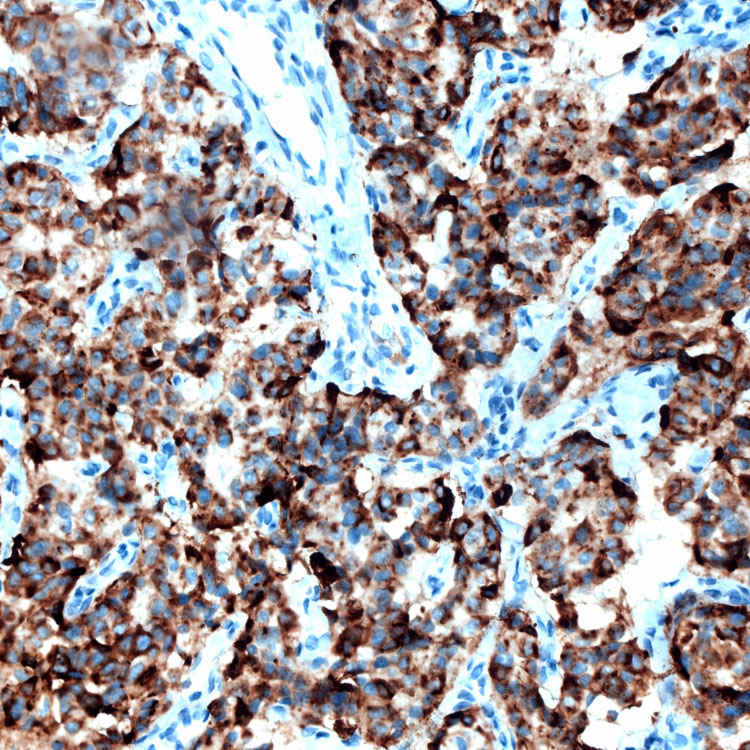
Chromogranin Stain Diffuse positive staining is shown. Absence of reactivity for neuroendocrine markers (chromogranin/synaptophysin) should prompt reevaluation of the diagnosis.
TERMINOLOGY
Abbreviations
• Neuroendocrine tumor (NET)
Synonyms
• Pancreatic NET
• Pancreatic endocrine tumor
• Islet cell tumor
Definitions
• Low- to intermediate-grade NET of pancreas
ETIOLOGY/PATHOGENESIS
Syndromic
• Multiple endocrine neoplasia syndrome
• von Hippel-Lindau syndrome
• Tuberous sclerosis
Sporadic
• Majority of cases are nonsyndromic and sporadic
CLINICAL ISSUES
Presentation
• Epidemiology
Peak incidence between 30-60 years
No significant gender predilection
• Presenting symptoms
Abdominal pain, jaundice
Asymptomatic, detected by imaging
– Such incidentally detected pancreatic NETs are increasingly common
• Endocrine function
Functioning tumors
– Insulinoma
– Glucagonoma
– Somatostatinoma
– Gastrinoma
– Vipomas
Nonfunctional tumors
– More common than functional tumors
Treatment
• Surgical approaches
Surgical resection remains mainstay of therapy for tumors confined to pancreas
Enucleation is restricted to small tumors (typically < 2 cm)
• Options for tumors metastatic to liver
Resection of primary and surgical debulking of metastatic tumor
Long-acting somatostatin analogs (octreotide and lanreotide)
Liver-directed therapy, including embolization, chemoembolization, radiofrequency ablation
Novel agents, such as inhibitor of VEGF, inhibitor of tyrosine kinase, and mTOR pathway
Prognosis
• Outcome is variable
• Histological and immunohistochemical features help estimate risk of aggressive behavior
• Features associated with adverse outcome include
Size > 2 cm
Tumor necrosis
Mitoses > 2/10 HPF
Vascular invasion
Perineural invasion
High Ki-67 index
CK19 positivity
IMAGING
CT Findings
• Solid, or less commonly, solid and cystic, well-circumscribed, enhancing lesion
MACROSCOPIC
General Features
• Solid, round to oval, well-circumscribed mass
• ∼ 5% of tumors are cystic
Either multilocular or unicystic
Size
• Tumors < 0.5 cm are termed microadenomas
MICROSCOPIC
Histologic Features
• Monotonous population of round cells
• Nuclear chromatin is typically coarse with salt and pepper appearance
• Large nucleoli may be present
• Less common cytoplasmic variations include oncocytic, vacuolated lipid-rich variant, and rhabdoid
Only gold members can continue reading. Log In or Register to continue