Vasculitis, ANCA-Related
Monica P. Revelo, MD, PhD
Key Facts
Terminology
Systemic vasculitis involving small to medium-sized vessels associated with or caused by ANCA
Kidney involvement is characterized by prominent crescents and scant or no immunoglobulin deposition
Clinical Issues
Overall, AAV vasculitis is rare in children
Whites and females more commonly involved
MPO ANCA (p-ANCA) is most common in PIGN, MPA and CSS
PR3 ANCA (c-ANCA) is most common in GPA
Microscopic Pathology
Glomerular lesions are similar in all PIGN
Fibrinoid necrosis and capillary basement membrane disruption
Crescents: Cellular/fibrocellular (in active phase) and fibrous (chronic phase) involving most of glomeruli present, usually > 50%
Minimal cellular proliferation (endocapillary/mesangial) may be seen
Bowman capsule rupture and periglomerular inflammation in severe cases
Segmental scars in healing/chronic phase
Segmental/circumferential fibrinoid necrosis and perivascular inflammation
Eosinophils are more prominent in CSS
Ancillary Tests
In all types of PIGN, there are minimal (< 1-2+) or no deposits of immunoglobulins and complement
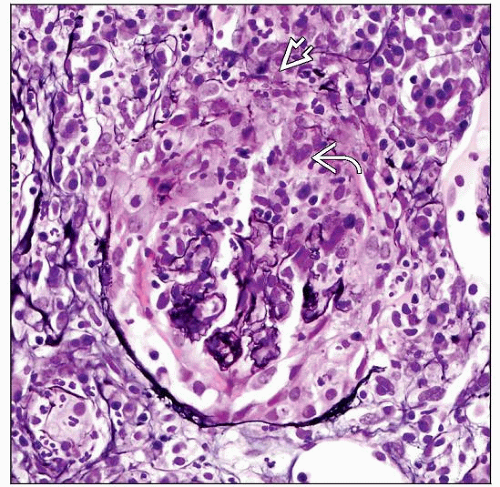 Necrotizing crescentic glomerulonephritis is the finding that characterizes AAV. In this case of GPA, a circumferential cellular crescent  is seen in the Bowman space, and the capsule is ruptured is seen in the Bowman space, and the capsule is ruptured  . . |
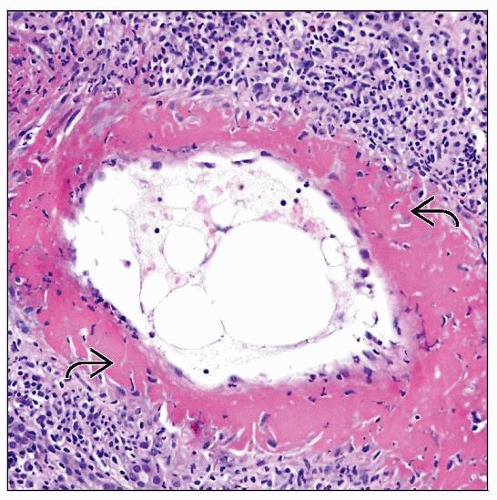 Fibrinoid necrosis  of arteries is commonly seen in AAV, especially in GPA and MPA. In children, the small-/medium-sized arteries in the respiratory tract are more commonly involved than are those in the kidney. of arteries is commonly seen in AAV, especially in GPA and MPA. In children, the small-/medium-sized arteries in the respiratory tract are more commonly involved than are those in the kidney. |
TERMINOLOGY
Abbreviations
Antineutrophil cytoplasmic antibody (ANCA)-associated vasculitis (AAV)
Synonyms
Pauci-immune glomerulonephritis (PIGN)
Pauci-immune crescentic glomerulonephritis
Rapidly progressive glomerulonephritis (RPGN)
Definitions
Systemic vasculitis involving small to medium-sized vessels associated with or caused by ANCA
Kidney involvement is characterized by prominent crescents and scant or no immunoglobulin deposition
Includes: Granulomatosis with polyangiitis (GPA), microscopic polyangiitis (MPA), Churg-Strauss syndrome (CSS), and limited pauci-immune glomerulonephritis
ETIOLOGY/PATHOGENESIS
Autoimmunity
Autoantibodies made to neutrophil lysosomal components (PR3 or MPO)
Antigens expressed on surface of activated neutrophils
ANCA augments neutrophil-mediated cytotoxicity
ANCA initiates signal transduction pathways for cell activation, FcR participation
Neutrophils activate alternative complement pathway
Leukocyte activation and adhesion to primed endothelial cells, resulting in cell damage
Trigger for ANCA production unknown
Presumed immune dysregulation
Evidence of molecular mimicry
Can be precipitated by drugs (propylthiouracil, hydralazine, penicillamine, minocycline)
Cell-mediated immune mechanisms with T-lymphocytes, neutrophils, and histiocytes are necessary for crescentic glomerulonephritis development
CLINICAL ISSUES
Epidemiology
Incidence
Overall, AAV is rare in children
GPA: 3.2:100,000 children/year
GPA > MPA in some studies
CSS very rare in children
Gender
F > M
Ethnicity
Whites more commonly involved
MPA most common small vessel vasculitis in Japan, China, Spain, and Kuwait
Presentation
Systemic manifestations
Malaise, fever, weight loss (89%)
Lung symptoms
Shortness of breath, chronic cough, hemoptysis/alveolar hemorrhage, nodules, abnormal pulmonary function, fixed pulmonary infiltrates (80%)
Ear, nose, and throat symptoms
Nasal involvement, sinusitis, otitis/mastoiditis, subglottic involvement, hearing loss, oral ulcers (80%)
Renal symptoms
Abnormal urinalysis (hematuria, proteinuria), biopsy-proven pauci-immune crescentic glomerulonephritis, elevated serum creatinine (75.4%)
Other symptoms
Conjunctivitis, scleritis, palpable purpura, abdominal pain, arthralgias/myalgia, arthritis, severe headache, dizziness
Laboratory Tests
Positive ANCA test by indirect immunofluorescence and ELISA
Myeloperoxidase (MPO) ANCA (p-ANCA) is most common in PIGN, MPA, and CSS
Proteinase 3 (PR3) ANCA (c-ANCA) is most common in GPA
Natural History
With treatment, clinical remission is possible, but relapses are common
Progression to end-stage renal disease may occur (˜ 10%)
Treatment
Surgical approaches
Renal transplantation
Drugs
Induction treatment
Pulse of methylprednisolone and cyclophosphamide
Plasma exchange
Maintenance treatment; although no validated studies are available, the following drugs have been used
Steroids
Azathioprine/mycophenolate mofetil
Methotrexate
Relapse
Pulse of methylprednisolone and cyclophosphamide
Rituximab
Prognosis
Remission of kidney and systemic manifestations can be accomplished with current therapy
Reported remission rate: 80-84%
Low mortality
Relapses are common after discontinuation of therapy
Prognostic factors of poor outcome include
Decreased glomerular filtration rate at presentation
Chronic lesions in renal biopsy
Nephrotic range proteinuria
Serum creatinine has been inversely correlated with kidney survival
Diagnostic Criteria for GPA (EULAR/PRINTO/PRES)
At least 3 criteria are necessary for diagnosis of GPA in childhood
Upper airway involvement
Laryngeo-tracheal-bronchial stenoses
Pulmonary involvement
Renal involvement
Granulomatous inflammation within arterial wall or perivascular/extravascular area
ANCA positivity
MICROSCOPIC PATHOLOGY
Histologic Features
Glomerular lesions are similar in all PIGN
Fibrinoid necrosis and capillary basement membrane disruption
Crescents: Cellular/fibrocellular (in active phase) and fibrous (chronic phase) involving most of glomeruli present, usually > 50%
Neutrophils can be seen within capillary loops
Minimal cellular proliferation (endocapillary/mesangial) may be seen
Bowman capsule rupture and periglomerular inflammation in severe cases
Segmental scars in healing/chronic phase
Tubules and interstitium
Significant mixed interstitial inflammatory infiltrate (neutrophils, mononuclear cells, and eosinophils) in acute phase
In GPA, interstitial inflammation may show granulomatous features
True granulomas are unusual in kidney biopsies, but their presence favors GPA
Eosinophils are more prominent in CSS and less prominent in MPA
Interstitial hemorrhage
Tubular necrosis with tubulitis may be seen
Vessels
Type of vessel involved
Interlobular/small arteries, arterioles, capillaries, and venules are affected in GPA
Arteries, arterioles, and capillaries in MPA
Arteries, arterioles, and, rarely, capillaries in CCS
Segmental/circumferential fibrinoid necrosis and perivascular inflammation
Eosinophils are more prominent in CSS
Progressive vascular sclerosis with loss of elastic in healing phase
Renal medullary capillaritis can be seen in GPA and MPA
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


