Patient Story
A 26-year-old man was given trimethoprim-sulfamethoxazole for sinusitis and broke out in hives 1 week later. The hives were all over his trunk and arms (Figures 150-1 and 150-2). He had no airway compromise and had only urticaria without angioedema. His sinus symptoms were mostly resolved, so he was told to stop the antibiotic and take an oral antihistamine. The H1-blocker gave him relief of symptoms and the wheals disappeared over the next 2 days.


Introduction
Urticaria and angioedema are a heterogeneous group of diseases that cause swelling of the skin and other soft tissues. They both result from a large variety of underlying causes, are elicited by a great diversity of factors, and present clinically in a highly variable way.1 Standard hives with transient wheals is the most common manifestation of urticaria.
Epidemiology
- It is estimated that 15% to 25% of the population may have urticaria sometime during their lifetime.2
- Urticaria affects 6% to 7% of preschool children and 17% of children with atopic dermatitis.2
- Among all age groups, approximately 50% have both urticaria and angioedema, 40% have isolated urticaria, and 10% have angioedema alone.2
- Acute urticaria is defined as less than 6 weeks’ duration. A specific cause is more likely to be identified in acute urticaria.2
- The cause of chronic urticaria (>6 weeks’ duration) is determined in less than 20% of cases.2
- Chronic urticaria is twice as common in women as in men.3
- Chronic urticaria predominantly affects adults.3
- Up to 40% of patients with chronic urticaria of more than 6 months’ duration still have urticaria 10 years later.3
Etiology and Pathophysiology
- The pathophysiology of angioedema and urticaria can be immunoglobulin (Ig) E mediated, complement mediated, related to physical stimuli, autoantibody mediated, or idiopathic.
- These mechanisms lead to mast cell degranulation resulting in the release of histamine. The histamine and other inflammatory mediators produce the wheals, edema, and pruritus.
- Urticaria is a dynamic process in which new wheals evolve as old ones resolve. These wheals result from localized capillary vasodilation, followed by transudation of protein-rich fluid into the surrounding skin. The wheals resolve when the fluid is slowly reabsorbed.
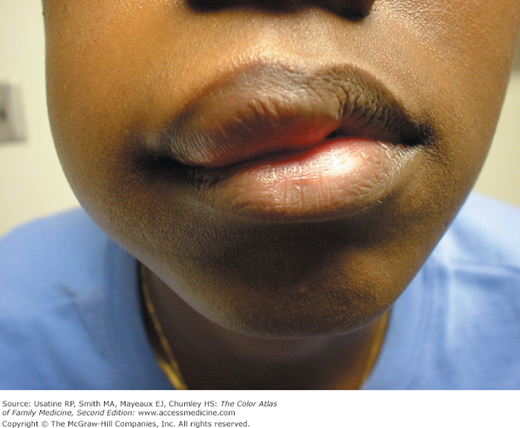
- Angioedema is an edematous area that involves transudation of fluid into the dermis and subcutaneous tissue (Figures 150-3 and 150-4).

- Immunologic—IgE mediated, complement mediated. Occurs more often in patients with an atopic background. Antigens are most commonly foods or medications. The most common foods are milk, nuts, wheat, and shellfish.
- Physical urticaria—Dermatographism, cold, cholinergic, solar, pressure, vibratory urticaria (Figures 150-5 and 150-6).
- Urticaria caused by mast cell-releasing agents—Mastocytosis, urticaria pigmentosa (Figures 150-7 and 150-8).
- Urticaria associated with vascular/connective tissue autoimmune disease.
- Hereditary angioedema is a potentially life-threatening disorder that is inherited in an autosomal dominant manner. In this disease, angioedema occurs without urticaria (Figure 150-9).




Figure 150-9
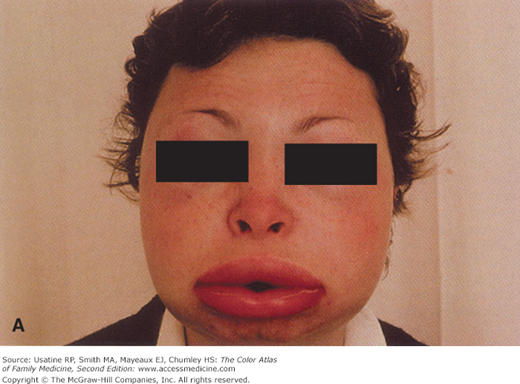
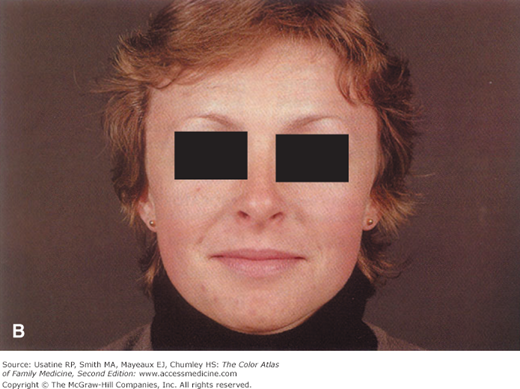
Hereditary angioedema. A. Severe edema of the face during an episode, leading to grotesque disfigurement. B. Angioedema will subside within hours. The patient had a positive family history and had multiple similar episodes including colicky abdominal pain. (With permission from Fitzpatrick’s Color Atlas and Synopsis of Clinical Dermatology, 5th ed. New York, NY: McGraw-Hill; 2005.)
Diagnosis
- Symptoms include itching, burning, and stinging.
- Wheals vary in size from small, 2-mm papules of cholinergic urticaria (Figure 150-6) to giant hives where a single wheal may cover a large portion of the trunk.
- The wheal may be all red or white, or the border may be red with the remainder of the surface white.
- Wheals may be annular (Figures 150-10 and 150-11).
- If dermatographism is present, one can write on the skin and be able to see the resulting words or shapes (Figure 150-5

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


