

APPROACHES TO STUDYING ANATOMY
Regional Anatomy
Systemic Anatomy
Clinical Anatomy
ANATOMICOMEDICAL TERMINOLOGY
Anatomical Position
Anatomical Planes
Terms of Relationship and Comparison
Terms of Laterality
Terms of Movement
ANATOMICAL VARIATIONS
INTEGUMENTARY SYSTEM
BLUE BOX: Integumentary System. Skin Color Signs in Physical Diagnosis; Skin Incisions and Scarring; Stretch Marks in Skin; Skin Injuries and Wounds
FASCIAS, FASCIAL COMPARTMENTS, BURSAE, AND POTENTIAL SPACES
BLUE BOX: Fascias. Fascial Planes and Surgery
SKELETAL SYSTEM
Cartilage and Bones
Bone Markings and Formations
BLUE BOX: Bones. Accessory (Supernumerary) Bones; Heterotopic Bones; Trauma to Bone and Bone Changes; Osteoporosis; Sternal Puncture; Bone Growth and Assessment of Bone Age; Effects of Disease and Diet on Bone Growth; Displacement and Separation of Epiphyses; Avascular Necrosis
Joints
BLUE BOX: Joints. Joints of Newborn Cranium; Degenerative Joint Disease; Arthroscopy
MUSCLE TISSUE AND MUSCULAR SYSTEM
Types of Muscle (Muscle Tissue)
Skeletal Muscles
TABLE I.1. Types of Muscle (MUSCLE TISSUE)
BLUE BOX: Skeletal Muscles. Muscle Dysfunction and Paralysis; Absence of Muscle Tone; Muscle Soreness and “Pulled” Muscles; Growth and Regeneration of Skeletal Muscle; Muscle Testing
Cardiac Striated Muscle
Smooth Muscle
BLUE BOX: Cardiac and Smooth Muscle. Hypertrophy of the Myocardium and Myocardial Infarction; Hypertrophy and Hyperplasia of Smooth Muscle
CARDIOVASCULAR SYSTEM
Vascular Circuits
Blood Vessels
BLUE BOX: Cardiovascular System. Arteriosclerosis: Ischemia and Infarction; Varicose Veins
LYMPHOID SYSTEM
BLUE BOX: Lymphoid System. Spread of Cancer; Lymphangitis, Lymphadenitis, and Lymphedema
NERVOUS SYSTEM
Central Nervous System
Peripheral Nervous System
BLUE BOX: Central and Peripheral Nervous System. Damage to the CNS; Rhizotomy; Nerve Degeneration and Ischemia of Nerves
Somatic Nervous System
Autonomic Nervous System (Ans)
TABLE I.2. Functions of Autonomic Nervous System (Ans)
MEDICAL IMAGING TECHNIQUES
Conventional Radiography
Computed Tomography
Ultrasonography
Magnetic Resonance Imaging
Nuclear Medicine Imaging
APPROACHES TO STUDYING ANATOMY
Anatomy is the setting (structure) in which the events (functions) of life occur. This book deals mainly with functional human gross anatomy—the examination of structures of the human that can be seen without a microscope. The three main approaches to studying anatomy are regional, systemic, and clinical (or applied), reflecting the body’s organization and the priorities and purposes for studying it.
Regional Anatomy
Regional anatomy (topographical anatomy) considers the organization of the human body as major parts or segments (Fig. I.1): a main body, consisting of the head, neck, and trunk (subdivided into thorax, abdomen, back, and pelvis/perineum), and paired upper limbs and lower limbs. All the major parts may be further subdivided into areas and regions. Regional anatomy is the method of studying the body’s structure by focusing attention on a specific part (e.g., the head), area (the face), or region (the orbital or eye region); examining the arrangement and relationships of the various systemic structures (muscles, nerves, arteries, etc.) within it; and then usually continuing to study adjacent regions in an ordered sequence. Outside of this Introduction, the regional approach is followed in this book, with each chapter addressing the anatomy of a major part of the body. This is the approach usually followed in anatomy courses that have a laboratory component involving dissection. When studying anatomy by this approach, it is important to routinely put the regional anatomy into the context of that of adjacent regions, parts, and of the body as a whole.

FIGURE I.1. Major parts of the body and regions of the lower limb. Anatomy is described relative to the anatomical position illustrated here.
Regional anatomy also recognizes the body’s organization by layers: skin, subcutaneous tissue, and deep fascia covering the deeper structures of muscles, skeleton, and cavities, which contain viscera (internal organs). Many of these deeper structures are partially evident beneath the body’s outer covering and may be studied and examined in living individuals via surface anatomy.
Surface anatomy is an essential part of the study of regional anatomy. It is specifically addressed in this book in “surface anatomy sections” (orange background) that provide knowledge of what lies under the skin and what structures are perceptible to touch (palpable) in the living body at rest and in action. We can learn much by observing the external form and surface of the body and by observing or feeling the superficial aspects of structures beneath its surface. The aim of this method is to visualize (recall distinct mental images of) structures that confer contour to the surface or are palpable beneath it and, in clinical practice, to distinguish any unusual or abnormal findings. In short, surface anatomy requires a thorough understanding of the anatomy of the structures beneath the surface. In people with stab wounds, for example, a physician must be able to visualize the deep structures that may be injured. Knowledge of surface anatomy can also decrease the need to memorize facts because the body is always available to observe and palpate.
Physical examination is the clinical application of surface anatomy. Palpation is a clinical technique, used with observation and listening for examining the body. Palpation of arterial pulses, for instance, is part of a physical examination. Students of many of the health sciences will learn to use instruments to facilitate examination of the body (such as an ophthalmoscope for observation of features of the eyeballs) and to listen to functioning parts of the body (a stethoscope to auscultate the heart and lungs).
Regional study of deep structures and abnormalities in a living person is now also possible by means of radiographic and sectional imaging and endoscopy. Radiographic and sectional imaging (radiographic anatomy) provides useful information about normal structures in living individuals, demonstrating the effect of muscle tone, body fluids and pressures, and gravity that cadaveric study does not. Diagnostic radiology reveals the effects of trauma, pathology, and aging on normal structures. In this book, most radiographic and many sectional images are integrated into the chapters where appropriate. The medical imaging sections at the end of each chapter provide an introduction to the techniques of radiographic and sectional imaging and include series of sectional images that apply to the chapter. Endoscopic techniques (using a insertable flexible fiber optic device to examine internal structures, such as the interior of the stomach) also demonstrate living anatomy. The detailed and thorough learning of the three-dimensional anatomy of deep structures and their relationships is best accomplished initially by dissection. In clinical practice, surface anatomy, radiographic and sectional images, endoscopy, and your experience from studying anatomy will combine to provide you with knowledge of your patient’s anatomy.
The computer is a useful adjunct in teaching regional anatomy because it facilitates learning by allowing interactivity and manipulation of two- and three-dimensional graphic models. Prosections, carefully prepared dissections for the demonstration of anatomical structures, are also useful. However, learning is most efficient and retention is highest when didactic study is combined with the experience of first-hand dissection—that is, learning by doing. During dissection you observe, palpate, move, and sequentially reveal parts of the body. In 1770, Dr. William Hunter, a distinguished Scottish anatomist and obstetrician, stated: “Dissection alone teaches us where we may cut or inspect the living body with freedom and dispatch.”
Systemic Anatomy
Systemic anatomy is the study of the body’s organ systems that work together to carry out complex functions. The basic systems and the field of study or treatment of each (in parentheses) are:
• The integumentary system (dermatology) consists of the skin (L. integumentum, a covering) and its appendages—hairs, nails, and sweat glands, for example—and the subcutaneous tissue just beneath it. The skin, an extensive sensory organ, forms the body’s outer, protective covering and container.
• The skeletal system (osteology) consists of bones and cartilage; it provides our basic shape and support for the body and is what the muscular system acts on to produce movement. It also protects vital organs such as the heart, lungs, and pelvic organs.
• The articular system (arthrology) consists of joints and their associated ligaments, connecting the bony parts of the skeletal system and providing the sites at which movements occur.
• The muscular system (myology) consists of skeletal muscles that act (contract) to move or position parts of the body (e.g., the bones that articulate at joints), or smooth and cardiac muscle that propels, expels, or controls the flow of fluids and contained substance.
• The nervous system (neurology) consists of the central nervous system (brain and spinal cord) and the peripheral nervous system (nerves and ganglia, together with their motor and sensory endings). The nervous system controls and coordinates the functions of the organ systems, enabling the body’s responses to and activities within its environment. The sense organs, including the olfactory organ (sense of smell), eye or visual system (ophthalmology), ear (sense of hearing and balance—otology), and gustatory organ (sense of taste), are often considered with the nervous system in systemic anatomy.
• The circulatory system (angiology) consists of the cardiovascular and lymphatic systems, which function in parallel to transport the body’s fluids.
• The cardiovascular system (cardiology) consists of the heart and blood vessels that propel and conduct blood through the body, delivering oxygen, nutrients, and hormones to cells and removing their waste products.
• The lymphatic system is a network of lymphatic vessels that withdraws excess tissue fluid (lymph) from the body’s interstitial (intercellular) fluid compartment, filters it through lymph nodes, and returns it to the bloodstream.
• The alimentary or digestive system (gastroenterology) consists of the digestive tract from the mouth to the anus, with all its associated organs and glands that function in ingestion, mastication (chewing), deglutition (swallowing), digestion, and absorption of food and the elimination of the solid waste (feces) remaining after the nutrients have been absorbed.
• The respiratory system (pulmonology) consists of the air passages and lungs that supply oxygen to the blood for cellular respiration and eliminate carbon dioxide from it. The diaphragm and larynx control the flow of air through the system, which may also produce tone in the larynx that is further modified by the tongue, teeth, and lips into speech.
• The urinary system (urology) consists of the kidneys, ureters, urinary bladder, and urethra, which filter blood and subsequently produce, transport, store, and intermittently excrete urine (liquid waste).
• The genital (reproductive) system (gynecology for females; andrology for males) consists of the gonads (ovaries and testes) that produce oocytes (eggs) and sperms, the ducts that transport them, and the genitalia that enable their union. After conception, the female reproductive tract nourishes and delivers the fetus.
• The endocrine system (endocrinology) consists of specialized structures that secrete hormones, including discrete ductless endocrine glands (such as the thyroid gland), isolated and clustered cells of the gut and blood vessel walls, and specialized nerve endings. Hormones are organic molecules that are carried by the circulatory system to distant effector cells in all parts of the body. The influence of the endocrine system is thus as broadly distributed as that of the nervous system. Hormones influence metabolism and other processes, such as the menstrual cycle, pregnancy, and parturition (childbirth).
None of the systems functions in isolation. The passive skeletal and articular systems and the active muscular system collectively constitute a supersystem, the locomotor system or apparatus (orthopedics), because they must work together to produce locomotion of the body. Although the structures directly responsible for locomotion are the muscles, bones, joints, and ligaments of the limbs, other systems are indirectly involved as well. The brain and nerves of the nervous system stimulate them to act; the arteries and veins of the circulatory system supply oxygen and nutrients to and remove waste from these structures; and the sensory organs (especially vision and equilibrium) play important roles in directing their activities in a gravitational environment.
In this Introduction, an overview of several systems significant to all parts and regions of the body will be provided before Chapters 1 through 8 cover regional anatomy in detail. Chapter 9 also presents systemic anatomy in reviewing the cranial nerves.
Clinical Anatomy
Clinical anatomy (applied anatomy) emphasizes aspects of bodily structure and function important in the practice of medicine, dentistry, and the allied health sciences. It incorporates the regional and systemic approaches to studying anatomy and stresses clinical application.
Clinical anatomy often involves inverting or reversing the thought process typically followed when studying regional or systemic anatomy. For example, instead of thinking, “The action of this muscle is to …,” clinical anatomy asks, “How would the absence of this muscle’s activity be manifest?” Instead of noting, “The … nerve provides innervation to this area of skin,” clinical anatomy asks, “Numbness in this area indicates a lesion of which nerve?”
Clinical anatomy is exciting to learn because of its role in solving clinical problems. The clinical correlation boxes (popularly called “blue boxes,” appearing on a blue background) throughout this book describe practical applications of anatomy. “Case studies,” such as those on the Clinically Oriented Anatomy website (http://thePoint.lww.com/COA7e), are integral parts of the clinical approach to studying anatomy.
The Bottom Line
STUDYING ANATOMY
Anatomy is the study of the structure of the human body. ♦ Regional anatomy considers the body as organized into segments or parts. ♦ Systemic anatomy sees the body as organized into organ systems. ♦ Surface anatomy provides information about structures that may be observed or palpated beneath the skin. ♦ Radiographic, sectional, and endoscopic anatomy allows appreciation of structures in living people, as they are affected by muscle tone, body fluids and pressures, and gravity. ♦ Clinical anatomy emphasizes application of anatomical knowledge to the practice of medicine.
ANATOMICOMEDICAL TERMINOLOGY
Anatomical terminology introduces and makes up a large part of medical terminology. To be understood, you must express yourself clearly, using the proper terms in the correct way. Although you are familiar with common, colloquial terms for parts and regions of the body, you must learn the international anatomical terminology (e.g., axillary fossa instead of armpit and clavicle instead of collarbone) that enables precise communication among healthcare professionals and scientists worldwide. Health professionals must also know the common and colloquial terms people are likely to use when they describe their complaints. Furthermore, you must be able to use terms people will understand when explaining their medical problems to them.
The terminology in this book conforms to the new International Anatomical Terminology. Terminologia Anatomica (TA) and Terminologia Embryologica (TE) list terms both in Latin and as English equivalents (e.g., the common shoulder muscle is musculus deltoideus in Latin and deltoid in English). Most terms in this book are English equivalents. Official terms are available at www.unifr.ch/ifaa. Unfortunately, the terminology commonly used in the clinical arena may differ from the official terminology. Because this discrepancy may be a source of confusion, this text clarifies commonly confused terms by placing the unofficial designations in parentheses when the terms are first used—for example, pharyngotympanic tube (auditory tube, eustachian tube) and internal thoracic artery (internal mammary artery). Eponyms, terms incorporating the names of people, are not used in the new terminology because they give no clue about the type or location of the structures involved. Further, many eponyms are historically inaccurate in terms of identifying the original person to describe a structure or assign its function, and do not conform to an international standard. Notwithstanding, commonly used eponyms appear in parentheses throughout the book when these terms are first used—such as sternal angle (angle of Louis)—since you will surely encounter them in your clinical years. Note that eponymous terms do not help to locate the structure in the body. The Clinically Oriented Anatomy website (http://thePoint.lww.com/COA7e) provides a list of eponymous terms.
Structure of terms. Anatomy is a descriptive science and requires names for the many structures and processes of the body. Because most terms are derived from Latin and Greek, medical language may seem difficult at first; however, as you learn the origin of terms, the words make sense. For example, the term gaster is Latin for stomach or belly. Consequently, the esophagogastric junction is the site where the esophagus connects with the stomach, gastric acid is the digestive juice secreted by the stomach, and a digastric muscle is a muscle divided into two bellies.
Many terms provide information about a structure’s shape, size, location, or function or about the resemblance of one structure to another. For example, some muscles have descriptive names to indicate their main characteristics. The deltoid muscle, which covers the point of the shoulder, is triangular, like the symbol for delta, the fourth letter of the Greek alphabet. The suffix -oid means “like”; therefore, deltoid means like delta. Biceps means two-headed and triceps means three-headed. Some muscles are named according to their shape—the piriformis muscle, for example, is pear shaped (L. pirum, pear + L. forma, shape or form). Other muscles are named according to their location. The temporal muscle is in the temporal region (temple) of the cranium (skull). In some cases, actions are used to describe muscles—for example, the levator scapulae elevates the scapula (L. shoulder blade). Anatomical terminology applies logical reasons for the names of muscles and other parts of the body, and if you learn their meanings and think about them as you read and dissect, it will be easier to remember their names.
Abbreviations. Abbreviations of terms are used for brevity in medical histories and in this and other books, such as in tables of muscles, arteries, and nerves. Clinical abbreviations are used in discussions and descriptions of signs and symptoms. Learning to use these abbreviations also speeds note taking. Common anatomical and clinical abbreviations are provided in this text when the corresponding term is introduced—for example, temporomandibular joint (TMJ). The Clinically Oriented Anatomy website (http://thePoint.lww.com/COA7e) provides a list of commonly used anatomical abbreviations. More extensive lists of common medical abbreviations may be found in the appendices of comprehensive medical dictionaries (e.g., Stedman’s Medical Dictionary, 28th ed.).
Anatomical Position
All anatomical descriptions are expressed in relation to one consistent position, ensuring that descriptions are not ambiguous (Figs. I.1 and I.2). One must visualize this position in the mind when describing patients (or cadavers), whether they are lying on their sides, supine (recumbent, lying on the back, face upward), or prone (lying on the abdomen, face downward). The anatomical position refers to the body position as if the person were standing upright with the:
• head, gaze (eyes), and toes directed anteriorly (forward),
• arms adjacent to the sides with the palms facing anteriorly, and
• lower limbs close together with the feet parallel.
This position is adopted globally for anatomicomedical descriptions. By using this position and appropriate terminology, you can relate any part of the body precisely to any other part. It should also be kept in mind, however, that gravity causes a downward shift of internal organs (viscera) when the upright position is assumed. Since people are typically examined in the supine position, it is often necessary to describe the position of the affected organs when supine, making specific note of this exception to the anatomical position.
Anatomical Planes
Anatomical descriptions are based on four imaginary planes (median, sagittal, frontal, and transverse) that intersect the body in the anatomical position (Fig. I.2):
• The median plane (median sagittal plane), the vertical plane passing longitudinally through the body, divides the body into right and left halves. The plane defines the midline of the head, neck, and trunk where it intersects the surface of the body. Midline is often erroneously used as a synonym for the median plane.
• Sagittal planes are vertical planes passing through the body parallel to the median plane. Parasagittal is commonly used but is unnecessary because any plane parallel to and on either side of the median plane is sagittal by definition. However, a plane parallel and near to the median plane may be referred to as a paramedian plane.
• Frontal (coronal) planes are vertical planes passing through the body at right angles to the median plane, dividing the body into anterior (front) and posterior (back) parts.
• Transverse planes are horizontal planes passing through the body at right angles to the median and frontal planes, dividing the body into superior (upper) and inferior (lower) parts. Radiologists refer to transverse planes as transaxial, which is commonly shortened to axial planes.
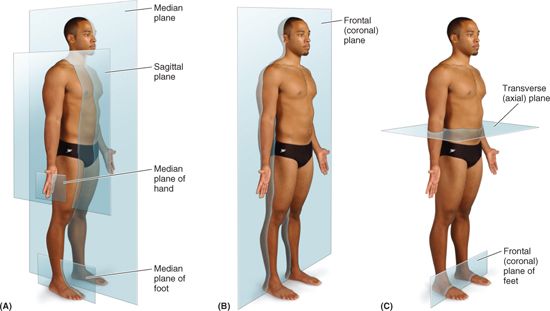
FIGURE I.2. Anatomical planes. The main planes of the body are illustrated.
Since the number of sagittal, frontal, and transverse planes is unlimited, a reference point (usually a visible or palpable landmark or vertebral level) is necessary to identify the location or level of the plane, such as a “transverse plane through the umbilicus” (Fig. I.2C). Sections of the head, neck, and trunk in precise frontal and transverse planes are symmetrical, passing through both the right and left members of paired structures, allowing some comparison.
The main use of anatomical planes is to describe sections (Fig. I.3):
• Longitudinal sections run lengthwise or parallel to the long axis of the body or of any of its parts, and the term applies regardless of the position of the body. Although median, sagittal, and frontal planes are the standard (most commonly used) longitudinal sections, there is a 180° range of possible longitudinal sections.
• Transverse sections, or cross sections, are slices of the body or its parts that are cut at right angles to the longitudinal axis of the body or of any of its parts. Because the long axis of the foot runs horizontally, a transverse section of the foot lies in the frontal plane (Fig. I.2C).
• Oblique sections are slices of the body or any of its parts that are not cut along the previously listed anatomical planes. In practice, many radiographic images and anatomical sections do not lie precisely in sagittal, frontal, or transverse planes; often they are slightly oblique.

FIGURE I.3. Sections of the limbs. Sections may be obtained by anatomical sectioning or medical imaging techniques.
Anatomists create sections of the body and its parts anatomically, and clinicians create them by planar imaging technologies, such as computerized tomography (CT), to describe and display internal structures.
Terms of Relationship and Comparison
Various adjectives, arranged as pairs of opposites, describe the relationship of parts of the body or compare the position of two structures relative to each other (Fig. I.4). Some of these terms are specific for comparisons made in the anatomical position, or with reference to the anatomical planes:

FIGURE I.4. Terms of relationship and comparison. These terms describe the position of one structure relative to another.
Superior refers to a structure that is nearer the vertex, the topmost point of the cranium (Mediev. L., skull). Cranial relates to the cranium and is a useful directional term, meaning toward the head or cranium. Inferior refers to a structure that is situated nearer the sole of the foot. Caudal (L. cauda, tail) is a useful directional term that means toward the feet or tail region, represented in humans by the coccyx (tail bone), the small bone at the inferior (caudal) end of the vertebral column.
Posterior (dorsal) denotes the back surface of the body or nearer to the back. Anterior (ventral) denotes the front surface of the body. Rostral is often used instead of anterior when describing parts of the brain; it means toward the rostrum (L. for beak); however, in humans it denotes nearer the anterior part of the head (e.g., the frontal lobe of the brain is rostral to the cerebellum).
Medial is used to indicate that a structure is nearer to the median plane of the body. For example, the 5th digit of the hand (little finger) is medial to the other digits. Conversely, lateral stipulates that a structure is farther away from the median plane. The 1st digit of the hand (thumb) is lateral to the other digits.
Dorsum usually refers to the superior aspect of any part that protrudes anteriorly from the body, such as the dorsum of the tongue, nose, penis, or foot. It is also used to describe the posterior surface of the hand, opposite the palm. Because the term dorsum may refer to both superior and posterior surfaces in humans, the term is easier to understand if one thinks of a quadripedal plantigrade animal that walks on its palms and soles, such as a bear. The sole is the inferior aspect or bottom of the foot, opposite the dorsum, much of which is in contact with the ground when standing barefoot. The surface of the hands, the feet, and the digits of both corresponding to the dorsum is the dorsal surface, the surface of the hand and fingers corresponding to the palm is the palmar surface, and the surface of the foot and toes corresponding to the sole is the plantar surface.
Combined terms describe intermediate positional arrangements: inferomedial means nearer to the feet and median plane—for example, the anterior parts of the ribs run inferomedially; superolateral means nearer to the head and farther from the median plane.
Other terms of relationship and comparisons are independent of the anatomical position or the anatomical planes, relating primarily to the body’s surface or its central core:
Superficial, intermediate, and deep describe the position of structures relative to the surface of the body or the relationship of one structure to another underlying or overlying structure.
External means outside of or farther from the center of an organ or cavity, while internal means inside or closer to the center, independent of direction.
Proximal and distal are used when contrasting positions nearer to or farther from the attachment of a limb or the central aspect of a linear structure, respectively.
Terms of Laterality
Paired structures having right and left members (e.g., the kidneys) are bilateral, whereas those occurring on one side only (e.g., the spleen) are unilateral. Designating whether you are referring specifically to the right or left member of bilateral structures can be critical, and is a good habit to begin at the outset of one’s training to become a health professional. Something occurring on the same side of the body as another structure is ipsilateral; the right thumb and right great (big) toe are ipsilateral, for example. Contralateral means occurring on the opposite side of the body relative to another structure; the right hand is contralateral to the left hand.
Terms of Movement
Various terms describe movements of the limbs and other parts of the body (Fig. I.5). Most movements are defined in relationship to the anatomical position, with movements occurring within, and around axes aligned with, specific anatomical planes. While most movements occur at joints where two or more bones or cartilages articulate with one another, several non-skeletal structures exhibit movement (e.g., tongue, lips, eyelids). Terms of movement may also be considered in pairs of oppositing movements:


FIGURE I.5. Terms of movement. These terms describe movements of the limbs and other parts of the body; most movements take place at joints, where two or more bones or cartilages articulate with one another.
Flexion and extension movements generally occur in sagittal planes around a transverse axis (Fig. I.5A & B). Flexion indicates bending or decreasing the angle between the bones or parts of the body. For most joints (e.g., elbow), flexion involves movement in an anterior direction. Extension indicates straightening or increasing the angle between the bones or parts of the body. Extension usually occurs in a posterior direction. The knee joint, rotated 180° to other joints, is exceptional in that flexion of the knee involves posterior movement and extension involves anterior movement. Dorsiflexion describes flexion at the ankle joint, as occurs when walking uphill or lifting the front of the foot and toes off the ground (Fig. I.5I). Plantarflexion bends the foot and toes toward the ground, as when standing on your toes. Extension of a limb or part beyond the normal limit—hyperextension (overextension)—can cause injury, such as “whiplash” (i.e., hyperextension of the neck during a rear-end automobile collision).
Abduction and adduction movements generally occur in a frontal plane around an anteroposterior axis (Fig. I.5E & G). Except for the digits, abduction means moving away from the median plane (e.g., when moving an upper limb laterally away from the side of the body) and adduction means moving toward it. In abduction of the digits (fingers or toes), the term means spreading them apart—moving the other fingers away from the neutrally positioned 3rd (middle) finger or moving the other toes away from the neutrally positioned 2nd toe. The 3rd finger and 2nd toe medially or laterally abduct away from the neutral position. Adduction of the digits is the opposite—bringing the spread fingers or toes together, toward the neutrally positioned 3rd finger or 2nd toe. Right and left lateral flexion (lateral bending) are special forms of abduction for only the neck and trunk (Fig. I.5J). The face and upper trunk are directed anteriorly as the head and/or shoulders tilt to the right or left side, causing the midline of the body itself to become bent sideways. This is a compound movement occurring between many adjacent vertebrae.
As you can see by noticing the way the thumbnail faces (laterally instead of posteriorly in the anatomical position), the thumb is rotated 90° relative to the other digits (Fig. I.5F). Therefore, the thumb flexes and extends in the frontal plane and abducts and adducts in the sagittal plane.
Circumduction is a circular movement that involves sequential flexion, abduction, extension, and adduction (or in the opposite order) in such a way that the distal end of the part moves in a circle (Fig. I.5H). Circumduction can occur at any joint at which all the above-mentioned movements are possible (e.g., the shoulder and hip joints).
Rotation involves turning or revolving a part of the body around its longitudinal axis, such as turning one’s head to face sideways (Fig. I.5G). Medial rotation (internal rotation) brings the anterior surface of a limb closer to the median plane, whereas lateral rotation (external rotation) takes the anterior surface away from the median plane.
Pronation and supination are the rotational movements of the forearm and hand that swing the distal end of the radius (the lateral long bone of the forearm) medially and laterally around and across the anterior aspect of the ulna (the other long bone of the forearm) while the proximal end of the radius rotates in place (Fig. I.5D). Pronation rotates the radius medially so that the palm of the hand faces posteriorly and its dorsum faces anteriorly. When the elbow joint is flexed, pronation moves the hand so that the palm faces inferiorly (e.g., placing the palms flat on a table). Supination is the opposite rotational movement, rotating the radius laterally and uncrossing it from the ulna, returning the pronated forearm to the anatomical position. When the elbow joint is flexed, supination moves the hand so that the palm faces superiorly. (Memory device: You can hold soup in the palm of your hand when the flexed forearm is supinated but are prone [likely] to spill it if the forearm is then pronated!)
Eversion moves the sole of the foot away from the median plane, turning the sole laterally (Fig. I.5I). When the foot is fully everted it is also dorsiflexed. Inversion moves the sole of the foot toward the median plane (facing the sole medially). When the foot is fully inverted it is also plantarflexed. Pronation of the foot actually refers to a combination of eversion and abduction that results in lowering of the medial margin of the foot (the feet of an individual with flat feet are pronated), and supination of the foot generally implies movements resulting in raising the medial margin of the foot, a combination of inversion and adduction.
Opposition is the movement by which the pad of the 1st digit (thumb) is brought to another digit pad (Fig. I.5C). This movement is used to pinch, button a shirt, and lift a teacup by the handle. Reposition describes the movement of the 1st digit from the position of opposition back to its anatomical position.
Protrusion is a movement anteriorly (forward) as in protruding the mandible (chin), lips, or tongue (Fig. I.5L). Retrusion is a movement posteriorly (backward), as in retruding the mandible, lips, or tongue. The similar terms protraction and retraction are used most commonly for anterolateral and posteromedial movements of the scapula on the thoracic wall, causing the shoulder region to move anteriorly and posteriorly (Fig. I.5M).
Elevation raises or moves a part superiorly, as in elevating the shoulders when shrugging, the upper eyelid when opening the eye, or the tongue when pushing it up against the palate (roof of mouth) (Fig. I.5K). Depression lowers or moves a part inferiorly, as in depressing the shoulders when standing at ease, the upper eyelid when closing the eye, or pulling the tongue away from the palate.
The Bottom Line
ANATOMICOMEDICAL TERMINOLOGY
Anatomical terms are descriptive terms standardized in an international reference guide, Terminologia Anatomica (TA). These terms, in English or Latin, are used worldwide. ♦ Colloquial terminology is used by—and to communicate with—lay people. ♦ Eponyms are often used in clinical settings but are not recommended because they do not provide anatomical context and are not standardized. ♦ Anatomical directional terms are based on the body in the anatomical position. ♦ Four anatomical planes divide the body, and sections divide the planes into visually useful and descriptive parts. ♦ Other anatomical terms describe relationships of parts of the body, compare the positions of structures, and describe laterality and movement.
ANATOMICAL VARIATIONS
Anatomy books describe (initially, at least) the structure of the body as it is usually observed in people—that is, the most common pattern. However, occasionally a particular structure demonstrates so much variation within the normal range that the most common pattern is found less than half the time! Beginning students are frequently frustrated because the bodies they are examining or dissecting do not conform to the atlas or text they are using (Bergman et al., 1988). Often students ignore the variations or inadvertently damage them by attempting to produce conformity. Therefore, you should expect anatomical variations when you dissect or inspect prosected specimens.
In a random group of people, individuals differ from each other in physical appearance. The bones of the skeleton vary not only in their basic shape but also in lesser details of surface structure. A wide variation is found in the size, shape, and form of the attachments of muscles. Similarly, considerable variation exists in the patterns of branching of veins, arteries, and nerves. Veins vary the most and nerves the least. Individual variation must be considered in physical examination, diagnosis, and treatment.
Most descriptions in this text assume a normal range of variation. However, the frequency of variation often differs among human groups, and variations collected in one population may not apply to members of another population. Some variations, such as those occurring in the origin and course of the cystic artery to the gallbladder, are clinically important (see Chapter 2), and any surgeon operating without knowledge of them is certain to have problems. Clinically significant variations are described in clinical correlation (blue) boxes identified with an Anatomical Variation icon (at left).
 Apart from racial and sexual differences, humans exhibit considerable genetic variation, such as polydactyly (extra digits). Approximately 3% of newborns show one or more significant birth defects (Moore et al, 2012). Other defects (e.g., atresia or blockage of the intestine) are not detected until symptoms occur. Discovering variations and congenital anomalies in cadavers is actually one of the many benefits of firsthand dissection, because it enables students to develop an awareness of the occurrence of variations and a sense of their frequency.
Apart from racial and sexual differences, humans exhibit considerable genetic variation, such as polydactyly (extra digits). Approximately 3% of newborns show one or more significant birth defects (Moore et al, 2012). Other defects (e.g., atresia or blockage of the intestine) are not detected until symptoms occur. Discovering variations and congenital anomalies in cadavers is actually one of the many benefits of firsthand dissection, because it enables students to develop an awareness of the occurrence of variations and a sense of their frequency.
The Bottom Line
ANATOMICAL VARIATIONS
Anatomical variations are common and students should expect to encounter them during dissection. It is important to know how such variations may influence physical examinations, diagnosis, and treatment.
INTEGUMENTARY SYSTEM
Because the skin (L. integumentum, a covering) is readily accessible and is one of the best indicators of general health, careful observation of it is important in physical examinations. It is considered in the differential diagnosis of almost every disease. The skin provides:
• Protection of the body from environmental effects, such as abrasions, fluid loss, harmful substances, ultraviolet radiation, and invading microorganisms.
• Containment for the body’s structures (e.g., tissues and organs) and vital substances (especially extracellular fluids), preventing dehydration, which may be severe when extensive skin injuries (e.g., burns) are experienced.
• Heat regulation through the evaporation of sweat and/or the dilation or constriction of superficial blood vessels.
• Sensation (e.g., pain) by way of superficial nerves and their sensory endings.
• Synthesis and storage of vitamin D.
The skin, the body’s largest organ, consists of the epidermis, a superficial cellular layer, and the dermis, a deep connective tissue layer (Fig. I.6).

FIGURE I.6. Skin and some of its specialized structures.
The epidermis is a keratinized epithelium—that is, it has a tough, horny superficial layer that provides a protective outer surface overlying its regenerative and pigmented deep or basal layer. The epidermis has no blood vessels or lymphatics. The avascular epidermis is nourished by the underlying vascularized dermis. The dermis is supplied by arteries that enter its deep surface to form a cutaneous plexus of anastomosing arteries. The skin is also supplied with afferent nerve endings that are sensitive to touch, irritation (pain), and temperature. Most nerve terminals are in the dermis, but a few penetrate the epidermis.
The dermis is a dense layer of interlacing collagen and elastic fibers. These fibers provide skin tone and account for the strength and toughness of skin. The dermis of animals is removed and tanned to produce leather. Although the bundles of collagen fibers in the dermis run in all directions to produce a tough felt-like tissue, in any specific location most fibers run in the same direction. The predominant pattern of collagen fibers determines the characteristic tension and wrinkle lines in the skin.
The tension lines (also called cleavage lines or Langer lines) tend to spiral longitudinally in the limbs and run transversely in the neck and trunk (Fig. I.7). Tension lines at the elbows, knees, ankles, and wrists are parallel to the transverse creases that appear when the limbs are flexed. The elastic fibers of the dermis deteriorate with age and are not replaced; consequently, in older people, the skin wrinkles and sags as it loses its elasticity.

FIGURE I.7. Tension lines in the skin. The dashed lines indicate the predominant direction of the collagen fibers in the dermis.
The skin also contains many specialized structures (Fig. I.6). The deep layer of the dermis contains hair follicles, with associated smooth arrector muscles and sebaceous glands. Contraction of the arrector muscles of hairs (L. musculi arrector pili) erects the hairs, causing goose bumps. Hair follicles are generally slanted to one side, and several sebaceous glands lie on the side the hair is directed toward (“points to”) as it emerges from the skin. Thus, contraction of the arrector muscles causes the hairs to stand up straighter, thereby compressing the sebaceous glands and helping them secrete their oily product onto the skin surface. The evaporation of the watery secretion (sweat) of the sweat glands from the skin provides a thermoregulatory mechanism for heat loss (cooling). Also involved in the loss or retention of body heat are the small arteries (arterioles) within the dermis. They dilate to fill superficial capillary beds to radiate heat (skin appears red) or constrict to minimize surface heat loss (skin, especially of the lips and fingertips, appears blue). Other skin structures or derivatives include the nails (fingernails, toenails), the mammary glands, and the enamel of teeth.
Located between the overlying skin (dermis) and underlying deep fascia, the subcutaneous tissue (superficial fascia) is composed mostly of loose connective tissue and stored fat and contains sweat glands, superficial blood vessels, lymphatic vessels, and cutaneous nerves (Fig. I.6). The neurovascular structures course in the subcutaneous tissue, distributing only their terminal branches to the skin.
The subcutaneous tissue provides for most of the body’s fat storage, so its thickness varies greatly, depending on the person’s nutritional state. In addition, the distribution of subcutaneous tissue varies considerably in different sites in the same individual. Compare, for example, the relative abundance of subcutaneous tissue evident by the thickness of the fold of skin that can be pinched at the waist or thighs with the anteromedial part of the leg (the shin, the anterior border of the tibia) or the back of the hand, the latter two being nearly devoid of subcutaneous tissue. Also consider the distribution of subcutaneous tissue and fat between the sexes: In mature females, it tends to accumulate in the breasts and thighs, whereas in males, subcutaneous fat accumulates in the lower abdominal wall.
Subcutaneous tissue participates in thermoregulation, functioning as insulation, retaining heat in the body’s core. It also provides padding that protects the skin from compression by bony prominences, such as those in the buttocks.
Skin ligaments (L. retinacula cutis), numerous small fibrous bands, extend through the subcutaneous tissue and attach the deep surface of the dermis to the underlying deep fascia (Fig. I.6). The length and density of these ligaments determines the mobility of the skin over deep structures. Where skin ligaments are longer and sparse, the skin is more mobile, such as on the back of the hand (Fig. I.8A & B). Where ligaments are short and abundant, the skin is firmly attached to the underlying deep fascia, such as in the palms and soles (Fig. I.8C). In dissection, removal of skin where the skin ligaments are short and abundant requires use of a sharp scalpel. The skin ligaments are long but particularly well developed in the breasts, where they form weight-bearing suspensory ligaments (see Chapter 1).

FIGURE I.8. Skin ligaments in subcutaneous tissue. A. The thickness of subcutaneous tissue can be estimated as being approximately half that of a pinched fold of skin (i.e., a fold of skin includes a double thickness of subcutaneous tissue). The dorsum of the hand has relatively little subcutaneous tissue. B. Long, relatively sparse skin ligaments allow the mobility of the skin demonstrated in part A. C. The skin of the palm (like that of the sole) is firmly attached to the underlying deep fascia.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


