

OVERVIEW: WALLS, CAVITIES, REGIONS, AND PLANES
ANTEROLATERAL ABDOMINAL WALL
TABLE 2.1. Abdominal Regions (A), Reference Planes (B), and Quadrants (C)
Fascia of Anterolateral Abdominal Wall
Muscles of Anterolateral Abdominal Wall
TABLE 2.2. Muscles of Anterolateral Abdominal Wall
Neurovasculature of Anterolateral Abdominal Wall
TABLE 2.3. Nerves of Anterolateral Abdominal Wall
TABLE 2.4. Arteries of Anterolateral Abdominal Wall
BLUE BOX: Fascia and Muscles of Anterolateral Abdominal Wall. Clinical Significance of Fascia and Fascial Spaces of Abdominal Wall; Protuberance of Abdomen; Abdominal Hernias; Neurovasculature of Anterolateral Abdominal Wall. Palpation of Anterolateral Abdominal Wall; Superficial Abdominal Reflexes; Injury to Nerves of Anterolateral Abdominal Wall; Abdominal Surgical Incisions; Longitudinal Incisions; Reversal of Venous Flow and Collateral Pathways of Superficial Abdominal Veins
Internal Surface of Anterolateral Abdominal Wall
Inguinal Region
TABLE 2.5. Boundaries of Inguinal Canal
Spermatic Cord, Scrotum, and Testes
TABLE 2.6. Corresponding Layers of Anterior Abdominal Wall, Scrotum, and Spermatic Cord
Surface Anatomy of Anterolateral Abdominal Wall
BLUE BOX: Internal Surface of Anterolateral Abdominal Wall and Inguinal Region. Undescended (Cryptorchid) Testis; External Supravesical Hernia; Postnatal Patency of Umbilical Vein; Metastasis of Uterine Cancer to Labium Majus; Spermatic Cord, Scrotum, and Testes. Inguinal Hernias; Cremasteric Reflex; Cysts and Hernias of Canal of Nuck; Hydrocele of Spermatic Cord and/or Testis; Hematocele of Testis; Torsion of Spermatic Cord; Anesthetizing Scrotum; Spermatocele and Epididymal Cyst; Vestigial Remnants of Embryonic Genital Ducts; Varicocele; Cancer of Testis and Scrotum
PERITONEUM AND PERITONEAL CAVITY
Embryology of Peritoneal Cavity
Peritoneal Formations
Subdivisions of Peritoneal Cavity
BLUE BOX: Peritoneum and Peritoneal Cavity. Patency and Blockage of Uterine Tubes; Peritoneum and Surgical Procedures; Peritonitis and Ascites; Peritoneal Adhesions and Adhesiotomy; Abdominal Paracentesis; Intraperitoneal Injection and Peritoneal Dialysis; Functions of Greater Omentum; Abscess Formation; Spread of Pathological Fluids; Flow of Ascitic Fluid and Pus; Fluid in Omental Bursa; Intestine in Omental Bursa; Severance of Cystic Artery
ABDOMINAL VISCERA
Overview of Abdominal Viscera and Digestive Tract
Esophagus
Stomach
TABLE 2.7. Arterial Supply to Abdominal Foregut Derivatives: Esophagus, Stomach, Liver, Gallbladder, Pancreas, and Spleen
Small Intestine
TABLE 2.8. Relationships of Duodenum
TABLE 2.9. Distinguishing Characteristics of Jejunum and Ileum in Living Body (Fig. 2.48)
Large Intestine
TABLE 2.10. Arterial Supply to Intestines
BLUE BOX: Esophagus and Stomach. Esophageal Varices; Pyrosis; Displacement of Stomach; Hiatal Hernia; Pylorospasm; Congenital Hypertrophic Pyloric Stenosis; Carcinoma of Stomach; Gastrectomy and Lymph Node Resection; Gastric Ulcers, Peptic Ulcers, Helicobacter pylori, and Vagotomy; Visceral Referred Pain; Small and Large Intestine. Duodenal Ulcers; Developmental Changes in Mesoduodenum; Paraduodenal Hernias; Brief Review of Embryological Rotation of Midgut; Navigating Small Intestine; Ischemia of Intestine; Ileal Diverticulum; Position of Appendix; Appendicitis; Appendectomy; Mobile Ascending Colon; Colitis, Colectomy, Ileostomy, and Colostomy; Colonoscopy; Diverticulosis; Volvulus of Sigmoid Colon
Spleen
Pancreas
Liver
TABLE 2.11. Terminology for Subdivisions of Liver
Biliary Ducts and Gallbladder
BLUE BOX: Spleen and Pancreas. Rupture of Spleen; Splenectomy and Splenomegaly; Accessory Spleen(s); Splenic Needle Biopsy and Splenoportography; Blockage of Hepatopancreatic Ampulla and Pancreatitis; Endoscopic Retrograde Cholangiopancreatography; Accessory Pancreatic Tissue; Pancreatectomy; Rupture of Pancreas; Pancreatic Cancer; Liver, Biliary Ducts, and Gallbladder. Palpation of Liver; Subphrenic Abscesses; Hepatic Lobectomies and Segmentectomy; Rupture of Liver; Aberrant Hepatic Arteries; Variations in Relationships of Hepatic Arteries; Hepatomegaly; Cirrhosis of Liver; Liver Biopsy; Mobile Gallbladder; Variations in Cystic and Hepatic Ducts; Accessory Hepatic Ducts; Gallstones; Gallstones in Duodenum; Cholecystectomy; Portal Hypertension; Portosystemic Shunts
Kidneys, Ureters, and Suprarenal Glands
BLUE BOX: Kidneys, Ureters, and Suprarenal Glands. Palpation of Kidneys; Perinephric Abscess; Nephroptosis; Renal Transplantation; Renal Cysts; Pain in Pararenal Region; Accessory Renal Vessels; Renal Vein Entrapment Syndrome; Congenital Anomalies of Kidneys and Ureters; Renal and Ureteric Calculi
Summary of Innervation of Abdominal Viscera
TABLE 2.12. Autonomic Innervation of Abdominal Viscera (Splanchnic Nerves)
DIAPHRAGM
Vessels and Nerves of Diaphragm
TABLE 2.13. Neurovascular Structures of Diaphragm
Diaphragmatic Apertures
Actions of Diaphragm
POSTERIOR ABDOMINAL WALL
Fascia of Posterior Abdominal Wall
Muscles of Posterior Abdominal Wall
TABLE 2.14. Muscles of Posterior Abdominal Wall
Nerves of Posterior Abdominal Wall
Vessels of Posterior Abdominal Wall
TABLE 2.15. Branches of Abdominal Aorta
BLUE BOX: Diaphragm. Hiccups; Section of a Phrenic Nerve; Referred Pain From Diaphragm; Rupture of Diaphragm and Herniation of Viscera; Congenital Diaphragmatic Hernia; Posterior Abdominal Wall. Psoas Abscess; Posterior Abdominal Pain; Partial Lumbar Sympathectomy; Pulsations of Aorta and Abdominal Aortic Aneurysm; Collateral Routes for Abdominopelvic Venous Blood
SECTIONAL MEDICAL IMAGING OF ABDOMEN
The abdomen is the part of the trunk between the thorax and the pelvis (Fig. 2.1). It is a flexible, dynamic container, housing most of the organs of the alimentary system and part of the urogenital system. Containment of the abdominal organs and their contents is provided by musculo-aponeurotic walls anterolaterally, the diaphragm superiorly, and the muscles of the pelvis inferiorly. The anterolateral musculo-aponeurotic walls are suspended between and supported by two bony rings (the inferior margin of the thoracic skeleton superiorly and the pelvic girdle inferiorly) linked by a semirigid lumbar vertebral column in the posterior abdominal wall. Interposed between the more rigid thorax and pelvis, this arrangement enables the abdomen to enclose and protect its contents while providing the flexibility required by respiration, posture, and locomotion.

FIGURE 2.1. Overview of viscera of thorax and abdomen in situ.
Through voluntary or reflexive contraction, its muscular roof, anterolateral walls, and floor can raise internal (intra-abdominal) pressure to aid expulsion of air from the thoracic cavity (lungs and bronchi) or of fluid (e.g., urine or vomitus), flatus, feces, or fetuses from the abdominopelvic cavity.
OVERVIEW: WALLS, CAVITIES, REGIONS, AND PLANES
The dynamic, multi-layered, musculo-aponeurotic abdominal walls not only contract to increase intra-abdominal pressure, but also distend considerably, accommodating expansions caused by ingestion, pregnancy, fat deposition, or pathology.
The anterolateral abdominal wall and several organs lying against the posterior wall are covered on their internal aspects with a serous membrane or peritoneum (serosa) that reflects (turns sharply and continues) onto the abdominal viscera (L., soft parts, internal organs), such as the stomach, intestine, liver, and spleen. Thus, a bursal sac or lined potential space (peritoneal cavity) is formed between the walls and the viscera that normally contains only enough extracellular (parietal) fluid to lubricate the membrane covering most of the surfaces of the structures forming or occupying the abdominal cavity. Visceral movement associated with digestion occurs freely, and the double-layered reflections of peritoneum passing between the walls and the viscera provide passage for the blood vessels, lymphatics, and nerves. Variable amounts of fat may also occur between the walls and viscera and the peritoneum lining them.
The abdominal cavity:
• forms the superior and major part of the abdominopelvic cavity (Fig. 2.2), the continuous cavity that extends between the thoracic diaphragm and pelvic diaphragm.
• has no floor of its own because it is continuous with the pelvic cavity. The plane of the pelvic inlet (superior pelvic aperture) arbitrarily, but not physically, separates the abdominal and the pelvic cavities.
• extends superiorly into the osseocartilaginous thoracic cage to the 4th intercostal space (Fig. 2.1). Consequently, the more superiorly placed abdominal organs (spleen, liver, part of the kidneys, and stomach) are protected by the thoracic cage. The greater pelvis (expanded part of the pelvis superior to the pelvic inlet) supports and partly protects the lower abdominal viscera (part of the ileum, cecum, appendix, and sigmoid colon).
• is the location of most digestive organs, parts of the urogenital system (kidneys and most of the ureters), and the spleen.

FIGURE 2.2. Abdominopelvic cavity. The body has been sectioned in the median plane to show the abdominal and pelvic cavities as subdivisions of the continuous abdominopelvic cavity.
Nine regions of the abdominal cavity are used to describe the location of abdominal organs, pains, or pathologies (Table 2.1A & B). The regions are delineated by four planes: two sagittal (vertical) and two transverse (horizontal) planes. The two sagittal planes are usually the midclavicular planes that pass from the midpoint of the clavicles (approximately 9 cm from the midline) to the midinguinal points, midpoints of the lines joining the anterior superior iliac spine (ASIS) and the pubic tubercles on each side.
TABLE 2.1. ABDOMINAL REGIONS (A), REFERENCE PLANES (B), AND QUADRANTS (C)
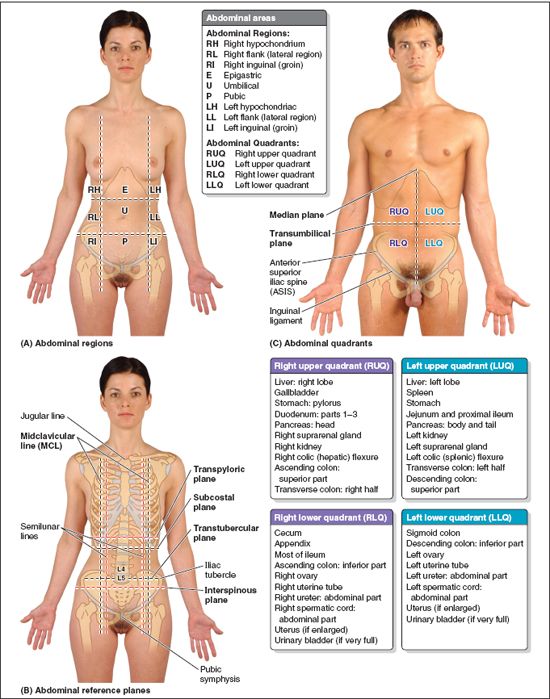
Most commonly, the transverse planes are the subcostal plane, passing through the inferior border of the 10th costal cartilage on each side, and the transtubercular plane, passing through the iliac tubercles (approximately 5 cm posterior to the ASIS on each side) and the body of the L5 vertebra. Both of these planes have the advantage of intersecting palpable structures.
Some clinicians use the transpyloric and interspinous planes to establish the nine regions. The transpyloric plane, extrapolated midway between the superior borders of the manubrium of the sternum and the pubic symphysis (typically the L1 vertebral level), commonly transects the pylorus (the distal, more tubular part of the stomach) when the patient is recumbent (supine or prone) (Fig. 2.1). Because the viscera sag with the pull of gravity, the pylorus usually lies at a lower level when the individual is standing erect. The transpyloric plane is a useful landmark because it also transects many other important structures: the fundus of the gallbladder, neck of the pancreas, origins of the superior mesenteric artery (SMA) and hepatic portal vein, root of the transverse mesocolon, duodenojejunal junction, and hila of the kidneys. The interspinous plane passes through the easily palpated ASIS on each side (Table 2.1B).
For more general clinical descriptions, four quadrants of the abdominal cavity (right and left upper and lower quadrants) are defined by two readily defined planes: (1) the transverse transumbilical plane, passing through the umbilicus (and the intervertebral [IV] disc between the L3 and L4 vertebrae), dividing it into upper and lower halves, and (2) the vertical median plane, passing longitudinally through the body, dividing it into right and left halves (Table 2.1C).
It is important to know what organs are located in each abdominal region or quadrant so that one knows where to auscultate, percuss, and palpate them (Table 2.1), and to record the locations of findings during a physical examination.
ANTEROLATERAL ABDOMINAL WALL
Although the abdominal wall is continuous, it is subdivided into the anterior wall, right and left lateral walls, and posterior wall for descriptive purposes (Fig. 2.3). The wall is musculo-aponeurotic, except for the posterior wall, which includes the lumbar region of the vertebral column. The boundary between the anterior and lateral walls is indefinite, therefore the term anterolateral abdominal wall is often used. Some structures, such as muscles and cutaneous nerves, are in both the anterior and lateral walls. The anterolateral abdominal wall extends from the thoracic cage to the pelvis.

FIGURE 2.3. Subdivisions of abdominal wall. A transverse section of the abdomen demonstrates various aspects of the wall and its components. [*The relatively superficial latissimus dorsi and deeper psoas major muscles are axioappendicular muscles that attach distally in the upper and lower limbs, respectively.]
The anterolateral abdominal wall is bounded superiorly by the cartilages of the 7th–10th ribs and the xiphoid process of the sternum, and inferiorly by the inguinal ligament and the superior margins of the anterolateral aspects of the pelvic girdle (iliac crests, pubic crests, and pubic symphysis) (Fig. 2.4A).

FIGURE 2.4. Abdominal contents, undisturbed, and layers of anterolateral abdominal wall. A. The anterior abdominal wall and soft tissues of the anterior thoracic wall have been removed. Most of the intestine is covered by the apron-like greater omentum, a peritoneal fold hanging from the stomach. B. Layers of the anterolateral abdominal wall, including the trilaminar flat muscles, are shown.
The anterolateral abdominal wall consists of skin and subcutaneous tissue (superficial fascia) composed mainly of fat, muscles and their aponeuroses and deep fascia, extraperitoneal fat, and parietal peritoneum (Fig. 2.4B). The skin attaches loosely to the subcutaneous tissue, except at the umbilicus, where it adheres firmly. Most of the anterolateral wall includes three musculotendinous layers; the fiber bundles of each layer run in different directions. This three-ply structure is similar to that of the intercostal spaces in the thorax.
Fascia of the Anterolateral Abdominal Wall
The subcutaneous tissue over most of the wall includes a variable amount of fat. It is a major site of fat storage. Males are especially susceptible to subcutaneous accumulation of fat in the lower anterior abdominal wall. In morbid obesity, the fat is many inches thick, often forming one or more sagging folds (L. panniculi; singular = panniculus, apron).
Superior to the umbilicus, the subcutaneous tissue is consistent with that found in most regions. Inferior to the umbilicus, the deepest part of the subcutaneous tissue is reinforced by many elastic and collagen fibers, so it has two layers: the superficial fatty layer (Camper fascia) and the deep membranous layer (Scarpa fascia) of subcutaneous tissue. The membranous layer continues inferiorly into the perineal region as the superficial perineal fascia (Colles fascia), but not into the thighs.
Superficial, intermediate, and deep layers of investing fascia cover the external aspects of the three muscle layers of the anterolateral abdominal wall and their aponeuroses (flat expanded tendons) and cannot be easily separated from them. The investing fascias here are extremely thin, being represented mostly by the epimysium (outer fibrous connective tissue layer surrounding all muscles—see Introduction) superficial to or between muscles. The internal aspect of the abdominal wall is lined with membranous and areolar sheets of varying thickness constituting endoabdominal fascia. Although continuous, different parts of this fascia are named according to the muscle or aponeurosis it is lining. The portion lining the deep surface of the transversus abdominis muscle and its aponeurosis is the transversalis fascia. The glistening lining of the abdominal cavity, the parietal peritoneum, is formed by a single layer of epithelial cells and supporting connective tissue. The parietal peritoneum is internal to the transversalis fascia and is separated from it by a variable amount of extraperitoneal fat.
Muscles of Anterolateral Abdominal Wall
There are five (bilaterally paired) muscles in the anterolateral abdominal wall (Fig. 2.3): three flat muscles and two vertical muscles. Their attachments are demonstrated in Figure 2.5 and listed, along with their nerve supply and main actions, in Table 2.2.

FIGURE 2.5. Muscles of anterolateral abdominal wall.
TABLE 2.2. MUSCLES OF ANTEROLATERAL ABDOMINAL WALL

aApproximately 80% of people have an insignificant muscle, the pyramidalis, which is located in the rectus sheath anterior to the most inferior part of the rectus abdominis. It extends from the pubic crest of the hip bone to the linea alba. This small muscle draws down on the linea alba.
bIn so doing, these muscles act as antagonists of the diaphragm to produce expiration.
The three flat muscles are the external oblique, internal oblique, and transversus abdominis. The muscle fibers of these three concentric muscle layers have varying orientations, with the fibers of the outer two layers running diagonally and perpendicular to each other for the main part, and the fibers of the deep layer running transversely. All three flat muscles are continued anteriorly and medially as strong, sheet-like aponeuroses (Fig. 2.6A). Between the midclavicular line (MCL) and the midline, the aponeuroses form the tough, aponeurotic, tendinous rectus sheath enclosing the rectus abdominis muscle (Fig. 2.6B). The aponeuroses then interweave with their fellows of the opposite side, forming a midline raphe (G. rhaphe, suture, seam), the linea alba (L. white line), which extends from the xiphoid process to the pubic symphysis. The decussation and interweaving of the aponeurotic fibers here is not only between right and left sides but also between superficial and intermediate and intermediate and deep layers.

FIGURE 2.6. Structure of anterolateral abdominal wall. A. Intramuscular and intermuscular fiber exchanges within the bilaminar aponeuroses of the external and internal oblique muscles are shown. B. Transverse sections of the wall superior and inferior to the umbilicus show the makeup of the rectus sheath.
The two vertical muscles of the anterolateral abdominal wall, contained within the rectus sheath, are the large rectus abdominis and the small pyramidalis.
EXTERNAL OBLIQUE MUSCLE
The external oblique muscle is the largest and most superficial of the three flat anterolateral abdominal muscles (Fig. 2.7). The attachments of the external oblique are demonstrated in Figure 2.5A, and listed, along with the nerve supply, and main actions, in Table 2.2. In contrast to the two deeper layers, the external oblique does not originate posteriorly from the thoracolumbar fascia; its posteriormost fibers (the thickest part of the muscle) have a free edge where they span between its costal origin and the iliac crest (Fig 2.5D & E). The fleshy part of the muscle contributes primarily to the lateral part of the abdominal wall. Its aponeurosis contributes to the anterior part of the wall.

FIGURE 2.7. Anterolateral abdominal wall. A. In this superficial dissection, the anterior layer of the rectus sheath is reflected on the left side. Observe the anterior cutaneous nerves (T7–T12) piercing the rectus abdominis and the anterior layer of the rectus sheath. B. The three flat abdominal muscles and the formation of the inguinal ligament are demonstrated.
Although the posteriormost fibers from rib 12 are nearly vertical as they run to the iliac crest, more anterior fibers fan out, taking an increasingly medial direction so that most of the fleshy fibers run inferomedially—in the same direction as the fingers do when the hands are in one’s side pockets—with the most anterior and superior fibers approaching a horizontal course. The muscle fibers become aponeurotic approximately at the MCL medially and at the spino-umbilical line (line running from the umbilicus to the ASIS) inferiorly, forming a sheet of tendinous fibers that decussate at the linea alba, most becoming continuous with tendinous fibers of the contralateral internal oblique (see Fig. 2.6A). Thus, the contralateral external and internal oblique muscles together form a “digastric muscle,” a two-bellied muscle sharing a common central tendon that works as a unit (see Introduction chapter). For example, the right external oblique and left internal oblique work together when flexing and rotating to bring the right shoulder toward the left hip (torsional movement of trunk).
Inferiorly, the external oblique aponeurosis attaches to the pubic crest medial to the pubic tubercle. The inferior margin of the external oblique aponeurosis is thickened as an undercurving fibrous band with a free posterior edge that spans between the ASIS and the pubic tubercle as the inguinal ligament (Poupart ligament) (Figs. 2.7B and 2.8).

FIGURE 2.8. Inferior abdominal wall and inguinal region of a male. The aponeurosis of the external oblique is partly cut away, and the spermatic cord has been cut and removed from the inguinal canal.
Palpate your inguinal ligament by pressing deeply into the center of the crease between the thigh and trunk and moving the fingertips up and down. Inferiorly the inguinal ligament is continuous with the deep fascia of the thigh. The inguinal ligament is therefore not a freestanding structure, although—as a useful landmark—it is frequently depicted as such. It serves as a retinaculum (retaining band) for the muscular and neurovascular structures passing deep to it to enter the thigh. The inferior parts of the two deeper anterolateral abdominal muscles arise in relationship to the lateral portion of the inguinal ligament. The complex modifications and attachments of the inguinal ligament, and of the inferomedial portions of the aponeuroses of the anterolateral abdominal wall muscles, are discussed in detail with the inguinal region (later in this chapter).
INTERNAL OBLIQUE MUSCLE
The intermediate of the three flat abdominal muscles, the internal oblique is a thin muscular sheet that fans out anteromedially (Figs. 2.5B, 2.8, and 2.9A). Except for its lowermost fibers, which arise from the lateral half of inguinal ligament, its fleshy fibers run perpendicular to those of the external oblique, running superomedially (like your the fingers when the hand is placed over your chest). Its fibers also become aponeurotic at the MCL and participate in the formation of the rectus sheath. The attachments of the internal oblique are demonstrated in Figure 2.5B, and listed, along with the nerve supply and main actions, in Table 2.2.

FIGURE 2.9. Formation of rectus sheath and neurovascular structures of anterolateral abdominal wall. A. In this deep dissection, the fleshy portion of the external oblique is excised on the right side, but its aponeurosis and the anterior wall of the rectus sheath are intact. The anterior wall of the sheath and the rectus abdominis are removed on the left side so that the posterior wall of the sheath may be seen. Lateral to the left rectus sheath, the fleshy part of the internal oblique has been cut longitudinally; the edges of the cut are retracted to reveal the thoraco-abdominal nerves coursing in the neurovascular plane between the internal oblique and the transversus abdominis. B. Sagittal section through the rectus sheath of the anterior abdominal wall.
TRANSVERSUS ABDOMINIS MUSCLE
The fibers of the transversus abdominis, the innermost of the three flat abdominal muscles (see Figs. 2.5C and 2.7B), run more or less transversally, except for the inferior ones, which run parallel to those of the internal oblique. This transverse, circumferential orientation is ideal for compressing the abdominal contents, increasing intra-abdominal pressure. The fibers of the transversus abdominis muscle also end in an aponeurosis, which contributes to the formation of the rectus sheath (Fig. 2.9). The attachments of the transversus abdominis are demonstrated in Figure 2.5C, and listed, along with the nerve supply and main actions, in Table 2.2.
Between the internal oblique and the transversus abdominis muscles is a neurovascular plane, which corresponds with a similar plane in the intercostal spaces. In both regions, the plane lies between the middle and deepest layers of muscle (Fig. 2.9A). The neurovascular plane of the anterolateral abdominal wall contains the nerves and arteries supplying the anterolateral abdominal wall. In the anterior part of the abdominal wall, the nerves and vessels leave the neurovascular plane and lie mostly in the subcutaneous tissue.
RECTUS ABDOMINIS MUSCLE
A long, broad, strap-like muscle, the rectus abdominis (L. rectus, straight) is the principal vertical muscle of the anterior abdominal wall (Figs. 2.5D, 2.6A, and 2.8B). The attachments of the rectus abdominis are demonstrated in Figure 2.5D, and listed, along with the nerve supply and main actions, in Table 2.2. The paired rectus muscles, separated by the linea alba, lie close together inferiorly. The rectus abdominis is three times as wide superiorly as inferiorly; it is broad and thin superiorly and narrow and thick inferiorly. Most of the rectus abdominis is enclosed in the rectus sheath. The rectus muscle is anchored transversely by attachment to the anterior layer of the rectus sheath at three or more tendinous intersections (see Figs. 2.5D and 2.7A). When tensed in muscular people, the areas of muscle between the tendinous intersections bulge outward. The intersections, indicated by grooves in the skin between the muscular bulges, usually occur at the level of the xiphoid process, umbilicus, and halfway between these structures.
PYRAMIDALIS
The pyramidalis is a small, insignificant triangular muscle that is absent in approximately 20% of people. It lies anterior to the inferior part of the rectus abdominis and attaches to the anterior surface of the pubis and the anterior pubic ligament. It ends in the linea alba, which is especially thickened for a variable distance superior to the pubic symphysis. The pyramidalis tenses the linea alba. When present, surgeons use the attachment of the pyramidalis to the linea alba as a landmark for median abdominal incision (Skandalakis et al., 2009).
RECTUS SHEATH, LINEA ALBA, AND UMBILICAL RING
The rectus sheath is the strong, incomplete fibrous compartment of the rectus abdominis and pyramidalis muscles (Figs. 2.7–2.9). Also found in the rectus sheath are the superior and inferior epigastric arteries and veins, lymphatic vessels, and distal portions of the thoraco-abdominal nerves (abdominal portions of the anterior rami of spinal nerves T7–T12).
The rectus sheath is formed by the decussation and interweaving of the aponeuroses of the flat abdominal muscles (Fig. 2.6B). The external oblique aponeurosis contributes to the anterior wall of the sheath throughout its length. The superior two thirds of the internal oblique aponeurosis splits into two layers (laminae) at the lateral border of the rectus abdominis; one lamina passing anterior to the muscle and the other passing posterior to it. The anterior lamina joins the aponeurosis of the external oblique to form the anterior layer of the rectus sheath. The posterior lamina joins the aponeurosis of the transversus abdominis to form the posterior layer of the rectus sheath.
Beginning approximately one third of the distance from the umbilicus to the pubic crest, the aponeuroses of the three flat muscles pass anterior to the rectus abdominis to form the anterior layer of the rectus sheath, leaving only the relatively thin transversalis fascia to cover the rectus abdominis posteriorly. A crescentic arcuate line (Fig. 2.9) demarcates the transition between the aponeurotic posterior wall of the sheath covering the superior three quarters of the rectus and the transversalis fascia covering the inferior quarter. Throughout the length of the sheath, the fibers of the anterior and posterior layers of the sheath interlace in the anterior median line to form the complex linea alba.
The posterior layer of the rectus sheath is also deficient superior to the costal margin because the transversus abdominis is continued superiorly as the transversus thoracis, which lies internal to the costal cartilages (see Fig. 1.14, p. 89), and the internal oblique attaches to the costal margin. Hence, superior to the costal margin, the rectus abdominis lies directly on the thoracic wall (Fig. 2.9B).
The linea alba, running vertically the length of the anterior abdominal wall and separating the bilateral rectus sheaths (Fig. 2.7A), narrows inferior to the umbilicus to the width of the pubic symphysis and widens superiorly to the width of the xiphoid process. The linea alba transmits small vessels and nerves to the skin. In thin muscular people, a groove is visible in the skin overlying the linea alba. At its middle, underlying the umbilicus, the linea alba contains the umbilical ring, a defect in the linea alba through which the fetal umbilical vessels passed to and from the umbilical cord and placenta. All layers of the anterolateral abdominal wall fuse at the umbilicus. As fat accumulates in the subcutaneous tissue postnatally, the skin becomes raised around the umbilical ring and the umbilicus becomes depressed. This occurs 7–14 days after birth, when the atrophic umbilical cord “falls off.”
FUNCTIONS AND ACTIONS OF ANTEROLATERAL ABDOMINAL MUSCLES
The muscles of the anterolateral abdominal wall:
• Form a strong expandable support for the anterolateral abdominal wall.
• Support the abdominal viscera and protect them from most injuries.
• Compress the abdominal contents to maintain or increase the intra-abdominal pressure and, in so doing, oppose the diaphragm (increased intra-abdominal pressure facilitates expulsion).
• Move the trunk and help to maintain posture.
The oblique and transverse muscles, acting together bilaterally, form a muscular girdle that exerts firm pressure on the abdominal viscera. The rectus abdominis participates little, if at all, in this action. Compressing the abdominal viscera and increasing intra-abdominal pressure elevates the relaxed diaphragm to expel air during respiration, and more forcibly for coughing, sneezing, nose blowing, voluntary eructation (burping), and yelling or screaming. When the diaphragm contracts during inspiration, the anterolateral abdominal wall expands as its muscles relax to make room for the organs, such as the liver, that are pushed inferiorly. The combined actions of the anterolateral muscles also produce the force required for defecation (discharge of feces), micturition (urination), vomiting, and parturition (childbirth). Increased intra-abdominal (and intrathoracic) pressure is also involved in heavy lifting, the resulting force sometimes producing a hernia.
The anterolateral abdominal muscles are also involved in movements of the trunk at the lumbar vertebrae and in controlling the tilt of the pelvis when standing for maintenance of posture (resisting lumbar lordosis). Consequently, strengthening the anterolateral abdominal wall musculature improves standing and sitting posture. The rectus abdominis is a powerful flexor of the thoracic and especially lumbar regions of the vertebral column, pulling the anterior costal margin and pubic crest toward each other. The oblique abdominal muscles also assist in movements of the trunk, especially lateral flexion and rotation of the lumbar and lower thoracic vertebral column. The transversus abdominis probably has no appreciable effect on the vertebral column (Standring, 2008).
Neurovasculature of Anterolateral Abdominal Wall
DERMATOMES OF ANTEROLATERAL ABDOMINAL WALL
The map of dermatomes of the anterolateral abdominal wall is almost identical to the map of peripheral nerve distribution (Fig. 2.10). This is because the anterior rami of spinal nerves T7–T12, which supply most of the abdominal wall, do not participate in plexus formation. The exception occurs at the L1 level, where the L1 anterior ramus bifurcates into two named peripheral nerves. Each dermatome begins posteriorly overlying the intervertebral foramen by which the spinal nerve exits the vertebral column and follows the slope of the ribs around the trunk. Dermatome T10 includes the umbilicus, whereas dermatome L1 includes the inguinal fold.

FIGURE 2.10. Dermatomes and nerves of anterolateral abdominal wall.
NERVES OF ANTEROLATERAL ABDOMINAL WALL
The skin and muscles of the anterolateral abdominal wall are supplied mainly by the following nerves (Fig. 2.9A and 2.10; Table 2.3):
• Thoraco-abdominal nerves: these are the distal, abdominal parts of the anterior rami of the inferior six thoracic spinal nerves (T7–T11); they are the former inferior intercostal nerves distal to the costal margin.
• Lateral (thoracic) cutaneous branches: of the thoracic spinal nerves T7–T9 or T10.
• Subcostal nerve: the large anterior ramus of spinal nerve T12.
• Iliohypogastric and ilio-inguinal nerves: terminal branches of the anterior ramus of spinal nerve L1.
TABLE 2.3. NERVES OF ANTEROLATERAL ABDOMINAL WALL

The thoraco-abdominal nerves pass inferoanteriorly from the intercostal spaces and run in the neurovascular plane between the internal oblique and the transversus abdominis muscles to supply the abdominal skin and muscles. The lateral cutaneous branches emerge from the musculature of the anterolateral wall to enter the subcutaneous tissue along the anterior axillary line (as anterior and posterior divisions), whereas the anterior abdominal cutaneous branches pierce the rectus sheath to enter the subcutaneous tissue a short distance from the median plane. Anterior abdominal cutaneous branches of thoraco-abdominal nerves (Fig. 2.10; Table 2.3):
• T7–T9 supply the skin superior to the umbilicus.
• T10 supplies the skin around the umbilicus.
• T11, plus the cutaneous branches of the subcostal (T12), iliohypogastric, and ilio-inguinal (L1), supply the skin inferior to the umbilicus.
During their course through the anterolateral abdominal wall, the thoraco-abdominal, subcostal, and iliohypogastric nerves communicate with each other.
VESSELS OF ANTEROLATERAL ABDOMINAL WALL
The skin and subcutaneous tissue of the abdominal wall are served by an intricate subcutaneous venous plexus, draining superiorly to the internal thoracic vein medially and the lateral thoracic vein laterally and inferiorly to the superficial and inferior epigastric veins, tributaries of the femoral and external iliac veins, respectively (Fig. 2.11). Cutaneous veins surrounding the umbilicus anastomose with para-umbilical veins, small tributaries of the hepatic portal vein that parallel the obliterated umbilical vein (round ligament of the liver). A relatively direct lateral superficial anastomotic channel, the thoraco-epigastric vein, may exist or develop (as a result of altered venous flow) between the superficial epigastric vein (a femoral vein tributary) and the lateral thoracic vein (an axillary vein tributary). The deeper veins of the anterolateral abdominal wall accompany the arteries, bearing the same name. A deeper, medial venous anastomosis may exist or develop between the inferior epigastric vein (an external iliac vein tributary) and the superior epigastric/internal thoracic veins (subclavian vein tributaries). The superficial and deep anastomoses may afford collateral circulation during blockage of either vena cava.

FIGURE 2.11. Lymphatics and superficial veins of anterolateral abdominal wall.
The primary blood vessels (arteries and veins) of the anterolateral abdominal wall are the
• Superior epigastric vessels and branches of the musculophrenic vessels from the internal thoracic vessels.
• Inferior epigastric and deep circumflex iliac vessels from the external iliac vessels.
• Superficial circumflex iliac and superficial epigastric vessels from the femoral artery and greater saphenous vein, respectively.
• Posterior intercostal vessels of the 11th intercostal space and the anterior branches of subcostal vessels.
The arterial supply to the anterolateral abdominal wall is demonstrated in Figure 2.12 and summarized in Table 2.4. The distribution of the deep abdominal blood vessels reflects the arrangement of the muscles: The vessels of the anterolateral abdominal wall have an oblique, circumferential pattern (similar to the intercostal vessels; Fig. 2.11), whereas the vessels of the central anterior abdominal wall are oriented more vertically.

FIGURE 2.12. Arteries of anterolateral abdominal wall.
TABLE 2.4. ARTERIES OF ANTEROLATERAL ABDOMINAL WALL

The superior epigastric artery is the direct continuation of the internal thoracic artery. It enters the rectus sheath superiorly through its posterior layer and supplies the superior part of the rectus abdominis and anastomoses with the inferior epigastric artery approximately in the umbilical region (see Fig. 2.9, Table 2.4)
The inferior epigastric artery arises from the external iliac artery just superior to the inguinal ligament. It runs superiorly in the transversalis fascia to enter the rectus sheath below the arcuate line. It enters the lower rectus abdominis and anastomoses with the superior epigastric artery (Fig. 2.9).
Lymphatic drainage of the anterolateral abdominal wall follows the following patterns (Fig. 2.11):
• Superficial lymphatic vessels accompany the subcutaneous veins; those superior to the transumbilical plane drain mainly to the axillary lymph nodes; however, a few drain to the parasternal lymph nodes. Superficial lymphatic vessels inferior to the transumbilical plane drain to the superficial inguinal lymph nodes.
• Deep lymphatic vessels accompany the deep veins of the abdominal wall and drain to the external iliac, common iliac, and right and left lumbar (caval and aortic) lymph nodes.
For an overview of superficial and deep lymphatic drainage, see the Introduction to Clinically Oriented Anatomy.
FASCIA AND MUSCLES OF ANTEROLATERAL ABDOMINAL WALL
Clinical Significance of Fascia and Fascial Spaces of Abdominal Wall
 Liposuction is a surgical method for removing unwanted subcutaneous fat using a percutaneously placed suction tube and high vacuum pressure. The tubes are inserted subdermally through small skin incisions.
Liposuction is a surgical method for removing unwanted subcutaneous fat using a percutaneously placed suction tube and high vacuum pressure. The tubes are inserted subdermally through small skin incisions.
When closing abdominal skin incisions inferior to the umbilicus, surgeons include the membranous layer of subcutaneous tissue when suturing because of its strength. Between this layer and the deep fascia covering the rectus abdominis and external oblique muscles is a potential space where fluid may accumulate (e.g., urine from a ruptured urethra). Although there are no barriers (other than gravity) to prevent fluid from spreading superiorly from this space, it cannot spread inferiorly into the thigh because the deep membranous layer of subcutaneous tissue fuses with the deep fascia of the thigh (fascia lata) along a line approximately 2.5 cm inferior and parallel to the inguinal ligament.
The endoabdominal fascia is of special importance in surgery. It provides a plane that can be opened, enabling the surgeon to approach structures on or in the anterior aspect of the posterior abdominal wall, such as the kidneys or bodies of lumbar vertebrae, without entering the membranous peritoneal sac containing the abdominal viscera. Thus, the risk of contamination is minimized. An anterolateral part of this potential space between the transversalis fascia and the parietal peritoneum (space of Bogros) is used for placing prostheses (Gore-Tex mesh, for example) when repairing inguinal hernias (Skandalakis et al., 1996) (see Fig. 2.15A & B).

FIGURE 2.15. Inguinal canal and spermatic cord. A. The layers of the abdominal wall and the coverings of the spermatic cord and testis derived from them are shown. B. Sagittal section of the anterior abdominal wall and inguinal canal at the plane shown in part A.
Protuberance of Abdomen
 A prominent abdomen is normal in infants and young children because their gastrointestinal tracts contain considerable amounts of air. In addition, their anterolateral abdominal cavities are enlarging and their abdominal muscles are gaining strength. An infant’s and young child’s relatively large liver also accounts for some bulging.
A prominent abdomen is normal in infants and young children because their gastrointestinal tracts contain considerable amounts of air. In addition, their anterolateral abdominal cavities are enlarging and their abdominal muscles are gaining strength. An infant’s and young child’s relatively large liver also accounts for some bulging.
Abdominal muscles protect and support the viscera most effectively when they are well toned; thus the well-conditioned adult of normal weight has a flat or scaphoid (lit. boat shaped; i.e., hollowed or concave) abdomen when in the supine position.
The six common causes of abdominal protrusion begin with the letter F: food, fluid, fat, feces, flatus, and fetus. Eversion of the umbilicus may be a sign of increased intra-abdominal pressure, usually resulting from ascites (abnormal accumulation of serous fluid in the peritoneal cavity), or a large mass (e.g., a tumor, a fetus, or an enlarged organ such as the liver).
Excess fat accumulation owing to overnourishment most commonly involves the subcutaneous fatty layer; however, there may also be excessive depositions of extraperitoneal fat in some types of obesity.
Tumors and organomegaly (organ enlargement such as splenomegaly—enlargement of the spleen) also produce abdominal enlargement. When the anterior abdominal muscles are underdeveloped or become atrophic, as a result of old age or insufficient exercise, they provide insufficient tonus to resist the increased weight of a protuberant abdomen on the anterior pelvis. The pelvis tilts anteriorly at the hip joints when standing (the pubis descends and the sacrum ascends) producing excessive lordosis (sway back) of the lumbar region.
Abdominal Hernias
 The anterolateral abdominal wall may be the site of abdominal hernias. Most hernias occur in the inguinal, umbilical, and epigastric regions (see the blue box “Inguinal Hernias,” p. 212). Umbilical hernias are common in neonates because the anterior abdominal wall is relatively weak in the umbilical ring, especially in low-birth-weight infants. Umbilical hernias are usually small and result from increased intra-abdominal pressure in the presence of weakness and incomplete closure of the anterior abdominal wall after ligation of the umbilical cord at birth. Herniation occurs through the umbilical ring. Acquired umbilical hernias occur most commonly in women and obese people. Extraperitoneal fat and/or peritoneum protrude into the hernial sac. The lines along which the fibers of the abdominal aponeuroses interlace are also potential sites of herniation (see Fig. 2.6B). Occasionally, gaps exist where these fiber exchanges occur—for example, in the midline or in the transition from aponeurosis to rectus sheath. These gaps may be congenital, the result of the stresses of obesity and aging, or the consequence of surgical or traumatic wounds.
The anterolateral abdominal wall may be the site of abdominal hernias. Most hernias occur in the inguinal, umbilical, and epigastric regions (see the blue box “Inguinal Hernias,” p. 212). Umbilical hernias are common in neonates because the anterior abdominal wall is relatively weak in the umbilical ring, especially in low-birth-weight infants. Umbilical hernias are usually small and result from increased intra-abdominal pressure in the presence of weakness and incomplete closure of the anterior abdominal wall after ligation of the umbilical cord at birth. Herniation occurs through the umbilical ring. Acquired umbilical hernias occur most commonly in women and obese people. Extraperitoneal fat and/or peritoneum protrude into the hernial sac. The lines along which the fibers of the abdominal aponeuroses interlace are also potential sites of herniation (see Fig. 2.6B). Occasionally, gaps exist where these fiber exchanges occur—for example, in the midline or in the transition from aponeurosis to rectus sheath. These gaps may be congenital, the result of the stresses of obesity and aging, or the consequence of surgical or traumatic wounds.
An epigastric hernia, a hernia in the epigastric region through the linea alba, occurs in the midline between the xiphoid process and the umbilicus. Spigelian hernias are those occurring along the semilunar lines (see Table 2.1B). These types of hernia tend to occur in people older than 40 years and are usually associated with obesity. The hernial sac, composed of peritoneum, is covered with only skin and fatty subcutaneous tissue.
NEUROVASCULATURE OF ANTEROLATERAL ABDOMINAL WALL
Palpation of Anterolateral Abdominal Wall
 Warm hands are important when palpating the abdominal wall because cold hands make the anterolateral abdominal muscles tense, producing involuntary spasms of the muscles, known as guarding. Intense guarding, board-like reflexive muscular rigidity that cannot be willfully suppressed, occurs during palpation when an organ (such as the appendix) is inflamed and in itself constitutes a clinically significant sign of acute abdomen. The involuntary muscular spasms attempt to protect the viscera from pressure, which is painful when an abdominal infection is present. The common nerve supply of the skin and muscles of the wall explains why these spasms occur.
Warm hands are important when palpating the abdominal wall because cold hands make the anterolateral abdominal muscles tense, producing involuntary spasms of the muscles, known as guarding. Intense guarding, board-like reflexive muscular rigidity that cannot be willfully suppressed, occurs during palpation when an organ (such as the appendix) is inflamed and in itself constitutes a clinically significant sign of acute abdomen. The involuntary muscular spasms attempt to protect the viscera from pressure, which is painful when an abdominal infection is present. The common nerve supply of the skin and muscles of the wall explains why these spasms occur.
Palpation of abdominal viscera is performed with the patient in the supine position with thighs and knees semiflexed to enable adequate relaxation of the anterolateral abdominal wall. Otherwise, the deep fascia of the thighs pulls on the membranous layer of abdominal subcutaneous tissue, tensing the abdominal wall. Some people tend to place their hands behind their heads when lying supine, which also tightens the muscles and makes the examination difficult. Placing the upper limbs at the sides and putting a pillow under the person’s knees tends to relax the anterolateral abdominal muscles.
Superficial Abdominal Reflexes
 The abdominal wall is the only protection most of the abdominal organs have. Consequently, the wall will react if an organ is diseased or injured. With the person supine and the muscles relaxed, the superficial abdominal reflex is elicited by quickly stroking horizontally, lateral to medial, toward the umbilicus. Usually, contraction of the abdominal muscles is felt; this reflex may not be observed in obese people. Similarly, any injury to the abdominal skin results in a rapid reflex contraction of the abdominal muscles.
The abdominal wall is the only protection most of the abdominal organs have. Consequently, the wall will react if an organ is diseased or injured. With the person supine and the muscles relaxed, the superficial abdominal reflex is elicited by quickly stroking horizontally, lateral to medial, toward the umbilicus. Usually, contraction of the abdominal muscles is felt; this reflex may not be observed in obese people. Similarly, any injury to the abdominal skin results in a rapid reflex contraction of the abdominal muscles.
Injury to Nerves of Anterolateral Abdominal Wall
 The inferior thoracic spinal nerves (T7–T12) and the iliohypogastric and ilio-inguinal nerves (L1) approach the abdominal musculature separately to provide the multi-segmental innervation of the abdominal muscles. Thus, they are distributed across the anterolateral abdominal wall, where they run oblique but mostly horizontal courses. They are susceptible to injury in surgical incisions or from trauma at any level of the abdominal wall. Injury to nerves of the anterolateral abdominal wall may result in weakening of the muscles. In the inguinal region, such a weakness may predispose an individual to development of an inguinal hernia (see the blue box “Inguinal Hernias” on p. 212).
The inferior thoracic spinal nerves (T7–T12) and the iliohypogastric and ilio-inguinal nerves (L1) approach the abdominal musculature separately to provide the multi-segmental innervation of the abdominal muscles. Thus, they are distributed across the anterolateral abdominal wall, where they run oblique but mostly horizontal courses. They are susceptible to injury in surgical incisions or from trauma at any level of the abdominal wall. Injury to nerves of the anterolateral abdominal wall may result in weakening of the muscles. In the inguinal region, such a weakness may predispose an individual to development of an inguinal hernia (see the blue box “Inguinal Hernias” on p. 212).
Abdominal Surgical Incisions
 Surgeons use various abdominal surgical incisions to gain access to the abdominal cavity. When possible, the incisions follow the cleavage lines (Langer lines) in the skin (see Introduction for discussion of these lines). The incision that allows adequate exposure, and secondarily, the best possible cosmetic effect, is chosen. The location of the incision also depends on the type of operation, the location of the organ(s) the surgeon wants to reach, bony or cartilaginous boundaries, avoidance of (especially motor) nerves, maintenance of blood supply, and minimizing injury to muscles and fascia of the abdominal wall while aiming for favorable healing. Thus, before making an incision, the surgeon considers the direction of the muscle fibers and the location of the aponeuroses and nerves. Consequently, a variety of incisions are routinely used, each having specific advantages and limitations.
Surgeons use various abdominal surgical incisions to gain access to the abdominal cavity. When possible, the incisions follow the cleavage lines (Langer lines) in the skin (see Introduction for discussion of these lines). The incision that allows adequate exposure, and secondarily, the best possible cosmetic effect, is chosen. The location of the incision also depends on the type of operation, the location of the organ(s) the surgeon wants to reach, bony or cartilaginous boundaries, avoidance of (especially motor) nerves, maintenance of blood supply, and minimizing injury to muscles and fascia of the abdominal wall while aiming for favorable healing. Thus, before making an incision, the surgeon considers the direction of the muscle fibers and the location of the aponeuroses and nerves. Consequently, a variety of incisions are routinely used, each having specific advantages and limitations.
Instead of transecting muscles, causing irreversible necrosis (death) of muscle fibers, the surgeon splits them in the direction of (and between) their fibers. The rectus abdominis is an exception; it can be transected because its muscle fibers run short distances between tendinous intersections, and the segmental nerves supplying it enter the lateral part of the rectus sheath where they can be located and preserved. Generally, incisions are made in the part of the anterolateral abdominal wall that gives the freest access to the targeted organ with the least disturbance to the nerve supply to the muscles. Muscles and viscera are retracted toward, not away from, their neurovascular supply.
Cutting a motor nerve paralyzes the muscle fibers supplied by it, thereby weakening the anterolateral abdominal wall. However, because of overlapping areas of innervation between nerves, one or two small branches of nerves may usually be cut without a noticeable loss of motor supply to the muscles or loss of sensation to the skin.
LONGITUDINAL INCISIONS
Longitudinal incisions, such as median and paramedian incisions (Fig. B2.1), are preferred for exploratory operations because they offer good exposure of and access to the viscera, and can be extended as necessary with minimal complication.

FIGURE B2.1.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


