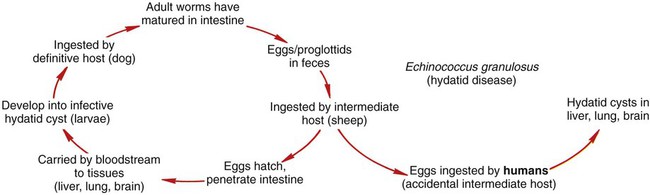
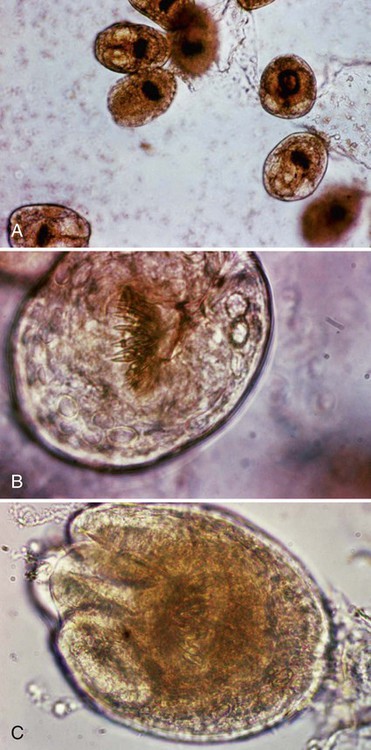
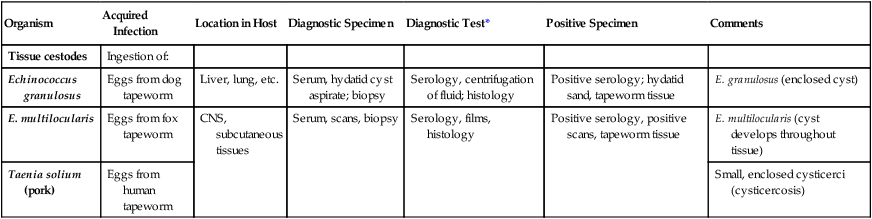
1. Describe and compare the life cycles of the tissue cestodes, including reservoir and intermediate hosts. 2. Describe the clinical manifestations and complications of cysticercus in the human host. 3. List the various methods used to diagnose cystericercus infection. 4. Define and describe the morphologic characteristics of the following: oncosphere, brood capsule, hydatid cyst, and hydatid sand. 5. Describe hydatid disease, including laboratory diagnosis and the best course of treatment. 6. Compare and contrast the pathogenesis and spectrum of disease associated with direct tissue damage versus the immune response to Echinococcus spp. 7. Describe the tapeworm that causes coenurosis, including hosts and symptoms of disease. 8. Describe the preventive measures recommended to avoid infection with tissue cestodes. Tissue cestodes do not reach the adult stage in the human host. The organisms infect the human in their intermediate or cyst stage. The infections are much more serious than those caused by the adult tapeworm. The parasites can cause serious disease, or even death. Larval cestodes cause infection by accidental ingestion of eggs excreted from the intermediate host (Table 55-1), and they lodge in various organs and tissues in the human body. Diagnosis of larval infections can be problematic. TABLE 55-1 Common Human Parasites, Diagnostic Specimens, Tests, and Positive Findings *Although serologic tests are not always mentioned, they are available for a number of parasitic infections. Unfortunately, most are not routinely available. Contact your state public health laboratory or the Centers for Disease Control and Prevention in Atlanta, Ga. Taenia solium, also known as the pork tapeworm, causes an intestinal infection from eating contaminated pork, as discussed in Chapter 54. The adult worm usually causes no clinical disease. Humans may accidentally become the intermediate host and ingest eggs from human feces. This typically occurs when an individual is already infected with adult T. solium. Autoinfection occurs when the individual swallows eggs from improper hand washing. Humans may develop the larval infection, which could result in cysticercosis. Cysticercosis is usually asymptomatic unless larvae invade the central nervous system (CNS), the globe of the eye, or other muscle and tissues. E. granulosus is most common in cool, damp areas where sheep herds are prevalent, such as southern South America, Russia, East Africa, and the western United States. The eggs in the definitive host are passed through the feces and contaminate soil, water, or food. The eggs are able to survive freezing conditions and can remain viable within the environment for several years. Adult worms are found only in the intermediate hosts (Figure 55-1). Hydatid disease in humans is potentially dangerous depending on the size and location of the cyst. Some cysts may remain undetected for many years until they grow large enough to affect other organs. Many humans live day-to-day without ever knowing they are infected. The cyst is very slow growing in humans. It is usually fluid-filled and has a germinal layer from which many thousands of scolices are budded. These are known as daughter cysts (brood capsules), which attach to the germinal layer or free-float in the cyst. The scolices in the hydatid fluid resemble grains of sand and are called hydatid sand (Figures 55-2, A and 55-3). The result is a unilocular cyst containing future adult worms. The cyst may resemble a slow-growing tumor. Infections in the liver or lungs may be asymptomatic for many years, but the pressure eventually causes noticeable symptoms. The majority of the hydatid cysts occur within the liver. Cysts within the liver cause chronic abdominal pain and allergic reactions and may result in cholangitis (infection of the common bile duct) and cholestasis (interference with flow of bile from the liver). Cysts that develop in the lungs may cause infections and abscesses and result in chronic cough, shortness of breath, and chest pain. During the life cycle of the cyst, there may be occasional seepage of fluid into the host tissue and circulation causing sensitization or activation of the immune response from the presence of the parasite. The rupture and release of the fluid of a hydatid cyst may cause anaphylactic shock as a result of the primary sensitization in a previously asymptomatic individual. If a cyst bursts within the human body, many new cysts may be released that are typically eliminated via the host’s cellular immune response. Leaking fluid from a cyst may cause notable eosinophilia.
Tissue Cestodes
Organism
Acquired Infection
Location in Host
Diagnostic Specimen
Diagnostic Test*
Positive Specimen
Comments
Tissue cestodes
Ingestion of:
Echinococcus granulosus
Eggs from dog tapeworm
Liver, lung, etc.
Serum, hydatid cyst aspirate; biopsy
Serology, centrifugation of fluid; histology
Positive serology; hydatid sand, tapeworm tissue
E. granulosus (enclosed cyst)
E. multilocularis
Eggs from fox tapeworm
CNS, subcutaneous tissues
Serum, scans, biopsy
Serology, films, histology
Positive serology, positive scans, tapeworm tissue
E. multilocularis (cyst develops throughout tissue)
Taenia solium (pork)
Eggs from human tapeworm
Small, enclosed cysticerci (cysticercosis)
Taenia Solium
General Characteristics
Echinococcus Granulosus
General Characteristics
Epidemiology
Pathogenesis and Spectrum of Disease
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Tissue Cestodes