Patient Story
A 6-year-old girl is brought to the office for a round, itchy rash on her body (Figure 138-1). It was first noted 2 weeks ago. The family cat does have some patches of hair loss. Note the concentric rings with scaling, erythema, and central sparing. UV light showed green fluorescence (Microsporum species) and the KOH is positive for branching and septate hyphae. The child was treated with a topical antifungal cream bid and the tinea resolves in 3 to 4 weeks. The family cat was taken to the veterinarian for treatment, too.
Figure 138-1
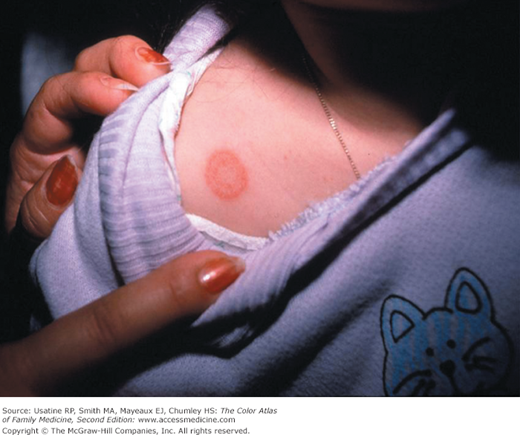
Tinea corporis on the shoulder of this young girl. This is a very typical annular pattern and the cat on a sweatshirt might be a clue to an infected pet at home spreading a Microsporum dermatophyte to its owner. Note the concentric rings with scaling, erythema, and central sparing. (Courtesy of Richard P. Usatine, MD.)
Introduction
Epidemiology
Etiology and Pathophysiology
Risk Factors
Diagnosis
The diagnosis can be made from history, clinical presentation, culture, and direct microscopic observation of hyphae in infected tissue and hairs after KOH preparation.
- Pruritus of affected area.
- Well-demarcated, annular lesions with central clearing, erythema, and scaling of the periphery. Concentric rings are highly specific (80%) for tinea infections (Figure 138-1).
- Central clearing is not always present (Figure 138-2).
- Although scale is the most prominent morphologic characteristic, some tinea infections will actually cause pustules from the inflammatory response (Figure 138-3).


Any part of the body including the face and axilla (Figures 138-1, 138-2, 138-3, 138-4).

Tinea incognito is a type of tinea infection that was previously not recognized by the physician or patient and topical steroids were used on the site. While applying the steroid, the dermatophyte continues to grow and form concentric rings (Figures 138-5 and 138-6).
Figure 138-5


Tinea incognito on the chest and arm of this black woman. This tinea infection continued to grow as the patient applied the topical steroids given to her by her physician. There is an extensive amount of postinflammatory hyperpigmentation. A. Tinea incognito on the arm with concentric rings as this dermatophyte infection continued to grow under the influence of the topical steroids. B. Tinea incognito on the chest. (Courtesy of Richard P. Usatine, MD.)
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


