normal in tumors. Therefore, our approach in evaluating a palpable thyroid mass is to begin with fine-needle aspiration biopsy, which we found to be a safe procedure as have many others (Castro and Gharib, 2000; Werga et al, 2000; Mazzaferri, 1993; Gagneten et al, 1987; Rojeski and Gharib, 1985; Löwhagen and Willems, 1981; Wang et al, 1976; Löwhagen and Sprenger, 1974). Using this approach, we have performed approximately 10,000 fine-needle aspiration biopsies of the thyroid, most guided by palpation and the others under ultrasound guidance.
pure colloid may be consistent with the diagnosis of benign colloid goiter and a pure population of macrophages may be diagnostic of a thyroid cyst or pseudocyst in a patient with past history of hemorrhage. In neither instance is the presence of epithelial cells required for diagnosis. Clearly, the issue depends on the type of lesion (cystic or solid) and the skill of the performer. It has been our experience that the latter is paramount.
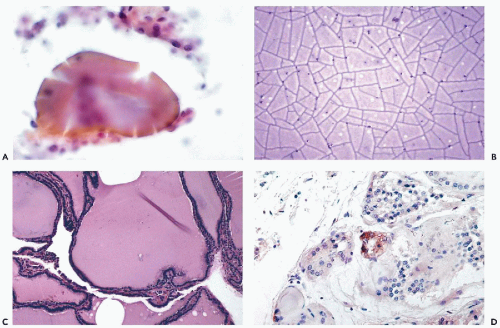 Figure 30-1 Benign thyroid. A. Large deposit of colloid surrounded by a few follicular cells. B. Pure colloid from a colloid nodule. Note the deep purple color and the “cracking artifact” in Diff-Quik stain. C. Histologic section of thyroid removed for colloid goiter corresponding to B. D. “C cells” immunostained for calcitonin by immunoperoxidase stain. |
Cysts
Goiters
Colloid goiter
Thyroiditis
Acute
Subacute (deQuervain’s)
Lymphocytic (Hashimoto’s disease)
Riedel’s Struma (fibrosing thyroiditis)
Tumors
Follicular tumors
Follicular adenomas
Follicular carcinoma
Hürthle cell tumors
Hürthle cell adenoma
Hürthle cell carcinoma
Other carcinomas
Papillary and its variants
Medullary
Anaplastic (large- and small-cell types)
Malignant lymphomas
Rare malignant tumors
Metastatic tumors
Acute thyroiditis
Cyst with acute hemorrhage
Subacute or De Quervain’s thyroiditis
Infarcted Hürthle cell tumor (rare)
Hashimoto’s thyroiditis
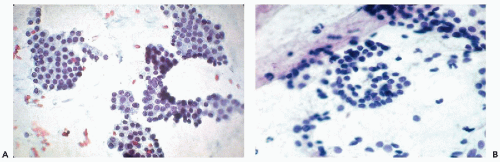 Figure 30-2 Benign follicular cells. A. Follicular cells forming flat sheets with “honeycomb” pattern. B. Clusters of normal follicular cells with many dispersed cells in the background. |
duct are located in the midline, usually above the thyroid, and are lined by either cylindrical or squamous epithelium (see below). A case of an intrathyroid lymphoepithelial cyst of probable branchial origin was described by Apel et al (1994). It must be stressed that some malignant tumors, particularly papillary carcinomas, are often partly cystic.
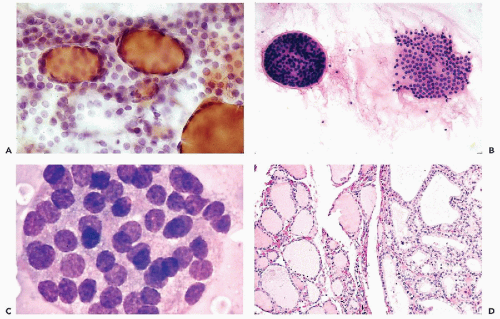 Figure 30-3 Thyroid follicles in benign goiters. A. Several colloid-filled follicles with dispersed follicular cells in the background. B. Left, An entire three-dimensional thyroid follicle. Right, Broken up follicle with a small deposit of colloid in the center. C. Tightly packed, compact thyroid follicle, commonly observed in benign colloid goiters. Note the abundant cytoplasm seen under high magnification with Diff-Quik stain. The term “syncytial balls” has been attached to this formation. D. Histologic section of colloid goiter. Note the variability in the size of the acini. (C: Courtesy of Dr. Sixtén Franzén, Stockholm, Sweden.) |
thyroiditis to chronic inflammatory processes. The term also includes a number of transient disorders such as postpartum thyroiditis and drug-induced thyroiditis (recent review in Pearce et al, 2003). Only the common forms of thyroiditis should be sampled by FNA and they are discussed below.
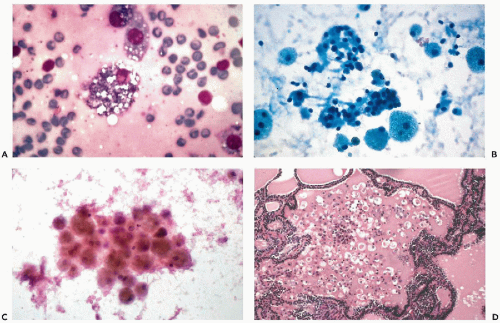 Figure 30-4 Macrophages in colloid goiter. A. A macrophage containing in its cytoplasm, numerous fragments of clear material, most likely fat. B. Numerous large macrophages with faintly vacuolated cytoplasm next to sheets of follicular cells. C. Hemosiderin containing macrophages from a hemorrhagic cyst of the thyroid. D. Follicle filled with colloid containing numerous macrophages. (A,C: High magnification; B: Diff-Quik stain.) |
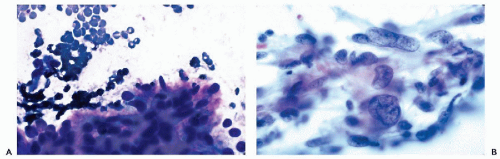 Figure 30-5 Fibrous reaction in colloid goiter. A. Cluster of elongated cells, corresponding to fibroblasts. B. Numerous elongated cells, some with giant nuclei, in reactive fibrosis in a thyroid scar. (A: Diff-Quik stain; B: high magnification.) |
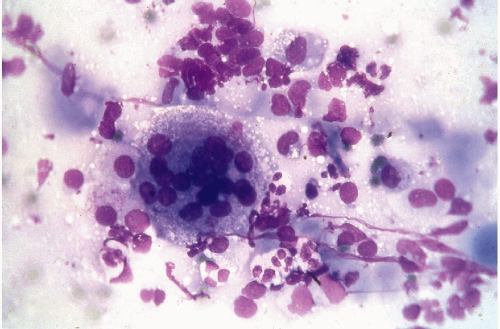 Figure 30-6 Subacute thyroiditis. The smear contains a large multinucleated giant cell surrounded by debris. (Diff-Quik stain.) |
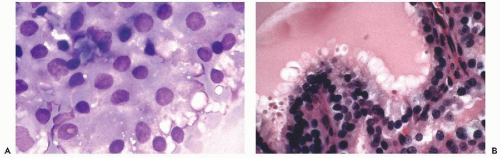 Figure 30-7 Hyperthyroidism (Graves’ disease). A. Follicular cells with eosinophilic cytoplasmic vacuoles in Diff-Quik stain, characteristic of hyperthyroidism. The term “flare cells” has been often attached to this phenomenon. B. Section of thyroid in hyperthyroidism, showing scalloped colloid and tall, vacuolated follicular cells. |
may occur in Hashimoto’s thyroiditis. There is a misperception that malignant lymphoma is the most common tumor seen in Hashimoto’s thyroiditis. In fact, from 5% to 10% of patients with this disease will develop papillary carcinoma, and less than 1% develop malignant lymphoma (Carson et al, 1996).
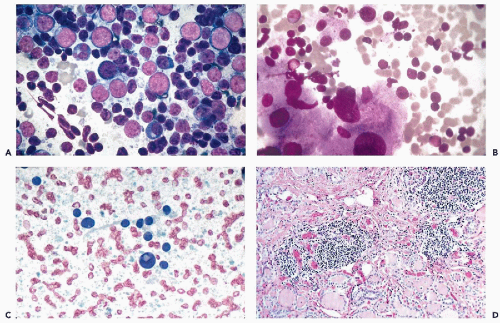 Figure 30-8 Hashimoto’s thyroiditis. A. Smear pattern with lymphocytic predominance. The lymphocytes are in various stages of maturation. This pattern may be misinterpreted as a malignant lymphoma. B. Scattered lymphocytes and large Hürthle cells. C. A Hürthle cell showing an intranuclear cytoplasmic inclusion. D. Histologic pattern of Hashimoto’s thyroiditis showing lymphocytic deposit and follicles lined by eosinophilic Hürthle cells. (A,B: Diff-Quik stain.) |
Further, the presence of abundant lymphocytes is very uncommon in Hürthle cell tumors.
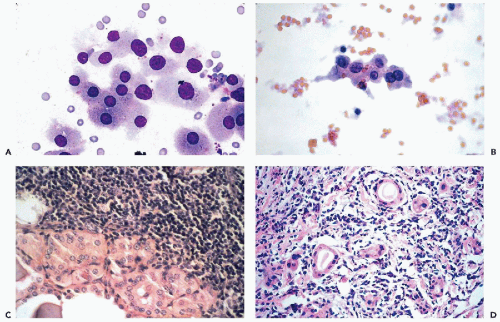 Figure 30-9 Hashimoto’s thyroiditis. A,B. Hürthle cells stained with Diff-Quik (A) and, after fixation, with Papanicolaou stain (B). The difference in size of the cells in the two modes of smear preparation is well shown. Note the variability in the sizes of the nuclei in the benign Hürthle cells. C. Section of the thyroid gland in Hashimoto’s disease showing lymphocytic infiltrate and Hürthle cells lining the adjacent acini. D. Section of the thyroid with follicular atrophy in Hashimoto’s thyroiditis. |
TABLE 30-1 KEY MORPHOLOGIC FEATURES OF DIFFERENTIAL DIAGNOSIS AMONG COMMON THYROID TUMORS | ||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
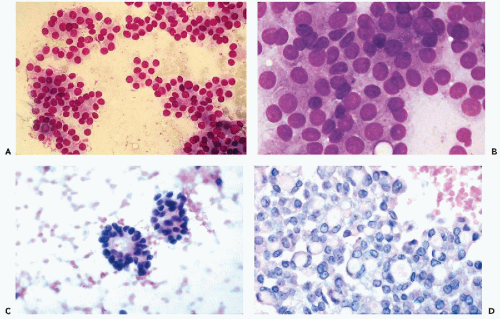 Figure 30-10 Follicular neoplasms. A,B. Flat spherical clusters of follicular cells stained with MGG. Note the absence of colloid and the somewhat enlarged nuclei, when compared with normal acini shown in Figure 30-2. C. One acinar and one solid cluster of follicular cells (Diff-Quik). D. Histologic section of a follicular adenoma, corresponding to C. Note small follicles containing scanty, pale colloid. |
visible. Small, indistinct intranuclear clear inclusions may occur and do not necessarily indicate a malignant tumor (see Fig. 30-10B). The papillary configuration of some of the colloid-free clusters may be reminiscent of papillary carcinoma. However, the clusters in papillary cancer are often multilayered and complex and show specific nuclear abnormalities that are not evident in follicular tumors (see below). Aspiration smears from follicular carcinomas are also highly cellular with little or no colloid. The cells occur primarily in clusters and are often arranged in follicle-like structures. Thus, they may closely resemble the cytologic presentation of follicular adenoma. In well-differentiated follicular carcinoma, cellular atypia may be minimal, and the general impression from the smear may suggest a benign lesion, rather than a carcinoma (Fig. 30-11). Therefore, in such cases, the cytologic diagnosis should be “follicular neoplasm or tumor,” clearly indicating that surgical excision and histologic examination is mandatory for a reliable differential diagnosis between follicular adenoma and a well-differentiated carcinoma.
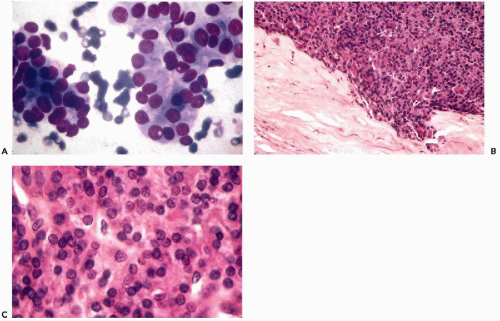 Figure 30-11 Follicular carcinoma. A. Aggregates of follicular cells with nuclear enlargement and small intranuclear cytoplasmic inclusions. The colloid is scanty. B. Periphery of the follicular tumor showing invasion of capsule. C. Histologic section of the same tumor composed of sheets of follicular cells with intranuclear cytoplasmic inclusions. (A: Diff-Quik stain.) |
and do not recur or metastasize after careful surgical removal. A papillary variant of Hürthle cell tumor and a variant of papillary carcinoma composed of Hürthle cells with lymphoid stroma (Warthin’s-like tumor) are discussed below with papillary carcinomas. Fewer than 10% of the Hürthle cell tumors invade the capsule, blood vessels, and adjacent organs and, therefore, must be considered malignant (Fig. 30-15D). Because of their unpredictable behavior, surgical removal of these tumors is the treatment of choice (Nguyen et al, 1999). Infarction of these tumors is an infrequent, but known, complication of FNA (Kini, 1996; Pinto and Mandreker, 1996).
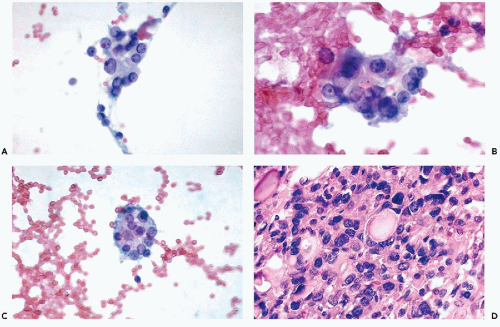 Figure 30-12 Follicular carcinoma with rapid progression in a 38-year-old man. A. Cluster of follicular cells showing variability in the nuclear sizes. B. High-power view of the tumor cells showing prominent nucleoli within the enlarged nuclei. C. Follicular structure of tumor cells. Note the presence of nucleoli. D. Histologic section of the primary tumor showing marked nuclear abnormalities. |
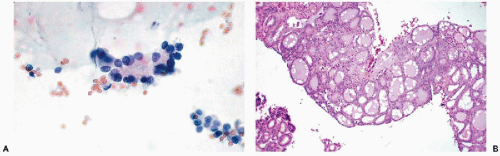 Figure 30-13 Follicular carcinoma. A. Thyroid aspirate. A cluster of acinar cells with central colloid. Nuclear pallor and small intranuclear cytoplasmic inclusions may be observed in some of the cells. This cluster could not be identified as malignant. B. Biopsy of bone, same patient. Bone metastasis of well differentiated thyroid carcinoma. This is an example of the so-called “benign metastasizing struma.” |
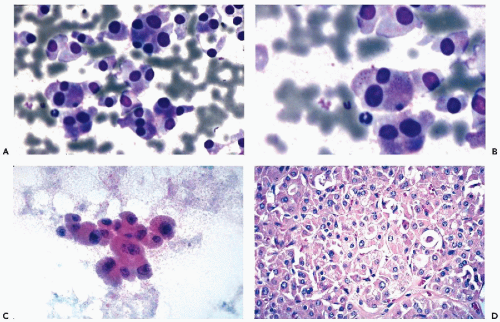 Figure 30-14 Malignant Hürthle cell tumor. A-C. Several examples of Hürthle cells in the tumor shown in D. Note the large Hürthle cells and some variability in cell and nuclear sizes. D. Section of the Hürthle cell tumor corresponding to A, B, and C. (A,B: Diff-Quik stain; B: high magnification.) |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


