The Skin
HISTORICAL OVERVIEW
The skin and its adnexa are easily sampled by “shave” or excisional biopsies, which are usually interpreted by tissue pathologists. Therefore, cytologic techniques, which require special skills of sampling and interpretation, are not widely used. It is of historical interest, though, that the term biopsy was coined by a French dermatologist, Ernest Besnier in 1879 (Besnier, 1879; Nezelof et al, 2001). Also, the German dermatologist, Hirschfeld (1912) first reported the use of a small caliber (thin or fine) needle for cell sampling in a case of malignant lymphoma of the skin.
Direct scrape smears are a much neglected field of cytologic diagnosis of skin lesions, although there is ample evidence that this approach is rapid, accurate and cost-effective (Zoon and Mali, 1950; Hitch et al, 1951; Wilson, 1954; Urbach et al, 1957; Goldman et al, 1960; Graham et al, 1961; Selbach and Heisel, 1962; Brown et al, 1979; Canti, 1984). To be sure, “scrape” cutaneous cytology requires skilled and dedicated practitioners with considerable expertise in the clinical and cytologic aspects of various cutaneous disorders, ranging from infectious disorders, bullous disease (such as pemphigus vulgaris), to benign tumors and other benign conditions of adnexal glands to cancer. Fine (thin) needle aspiration biopsy (FNA) is used by a small number of clinicians and cytopathologists to the diagnosis of palpable nodular lesions (Daskalopoulou et al, 1998; David et al, 1998). As in other organs, a limitation of this approach is the loss of the tissue patterns that some observers consider essential for diagnosis of many skin lesions (Ackerman, 1997).
In this chapter, the cytologic presentation of common disorders of the skin that may be diagnosed either by direct scrape cytology or by FNA, will be discussed.
BRIEF RECALL OF HISTOLOGY
The skin consists of keratinized squamous epithelium or epidermis and the underlying connective tissue or the dermis (see Fig. 5-2). The epidermis, which is similar to other squamous epithelia, contains antigen-presenting cells or the Langerhans’ cells and the endocrine Merkel cells. The dermis contains the sweat- and sebaceous glands and the piliary apparatus, i.e., hairs and hair follicles. All the components of the skin may be affected either by inflammatory disorders or by neoplastic disorders that may be either benign or malignant.
Methods of Sampling
Scrape Smears
Canti (1984) advocated the use of a double edge dissector, a lightweight instrument that can be used for removal of scrape samples and their spread on glass slides (Fig. 34-1). A variety of curettes, or even simple scalpel blades, may also be used for this purpose. In some cases, the layer of keratinized superficial cells must be removed from the surface of the lesion. Canti (1984) advocated the preparation of two smears, one fixed in alcohol for processing with Papanicolaou stain, and one unfixed, stained immediately with methylene blue or Diff-Quik stain (Dade Behring Inc., Deerfield, IL) for immediate microscopic diagnosis. In many instances, the rapidly stained smear is adequate for diagnosis and saves much time to the patient and the dermatologist who can initiate treatment without delay. Several examples of the latter techniques can be found in
this chapter, courtesy of Dr. G. Canti. The stain preparation techniques are discussed in Chapter 44.
this chapter, courtesy of Dr. G. Canti. The stain preparation techniques are discussed in Chapter 44.
 Figure 34-1 Curette used by Canti for sampling of skin lesions (Canti, 1984). |
Aspiration Biopsies (FNA)
For aspiration biopsies (FNA) of skin or subcutaneous nodules, a very small caliber needle (gauge 22 to 25), with or without syringe, can be used. For description of aspiration techniques of superficial skin nodules, see Chapter 28. Smear preparation may be the same, as outlined above for scrape smears. Nearly all of the recent reports are based on aspiration biopsies of palpable, nodular lesions of the skin and subcutaneous tissues (summaries in Koss et al, 1992; Layfield and Glasgow, 1993; Dey et al, 1996).
INFLAMMATORY DISORDERS
The skin is the site of numerous inflammatory disorders that require clinical recognition and sometimes skin biopsies for diagnosis. Cytologic approaches to this large group of diseases have not been explored, except for infectious disorders.
Infectious Disorders
Fungal and Parasitic Infections
Direct smear preparations for infectious disorders of the skin, especially in scaly skin lesions, have been in use for many years. The diagnosis of fungus infections of the skin (dermatophytosis) is readily accomplished in direct smears using a few drops of potassium hydroxide (KOH) to clear the cornified cells (squames) scraped from the surface of a lesion. The smears may be inspected unstained or stained with methylene blue or another rapid stain. Fungal hyphae and yeast forms (such as cryptococcus or blastomyces) may be demonstrated.
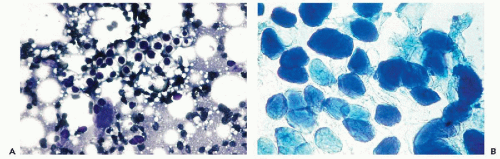 Figure 34-2 A. Cryptococcosis of skin. The spherical organisms with a thick capsule form single, tear-shaped buds (not shown). B. Molluscum contagiosum. High magnification to show molluscum bodies cells filled with masses of viral particles, pushing the nucleus to the periphery. (A: May-Grünwald-Giemsa [MGG] stain; B: Methylene blue stain.) (B: Courtesy of Dr. G. Canti, London, UK.) |
Aspiration biopsies of nodular lesions of the skin caused by fungal organisms have been reported. Thus, blastomycosis was reported by Desai et al (1997) and histoplasmosis by Stong et al (1994). We observed a case of cryptococcosis of the skin in the form of a palpable nodule in a patient with AIDS (Fig. 34-2A). The morphologic features of these organsims are discussed in Chapter 19.
Some parasitic diseases of the skin, such as the mite Sarcoptes scabiei causing a severe skin itch known as scabies and Leishmania donovanii, may also be identified in scrape smears (Baez-Giangreco et al, 1989; Koss et al, 1992). Kapila and Verma (1989) and Koss et al (1992) described filariasis of the skin. African trypanosomiasis (sleeping sickness) can also be diagnosed by aspiration of lymph nodes as first reported by Graig and Gray in 1904. The disease produces ulcerated skin lesions (chancre). The diagnosis can be established on fluid from the chancre (Case Records of the Massachusetts General Hospital, Case 20-2002). The harmless small parasite, Demodex folliculorum, a common inhabitant of follicular infundibula of face, can also be recognized in scrape smears because of eight protrusions known as “sucker feet” and a striated abdomen (Canti, 1984). Kamal and Grover (1995) reported on several cases of cysticercosis diagnosed by aspiration of subcutaneous nodules. For a detailed discussion of leishmaniasis and cysticercosis, see Chapter 19.
Bacterial Infections
Tuberculosis of the skin (known as lupus vulgaris) is now-a-days uncommon. Canti (1984) reported the presence of carrot-shaped epithelioid cells and occasional giant cells, accompanied by inflammatory exudate, in scrape smears. The same observer reported finding epithelioid cells in the uncommon skin manifestations of sarcoidosis. See Chapter 19 for a detailed discussion of these disorders.
The acid fast rods bacillus leprae (leprosy), which may
be very numerous in skin lesions of the lepromatous form, can also be recognized in aspiration smears (Singh et al, 1996). Other applications of this technique are to subcutaneous abscesses or infected cutaneous cysts that may also yield a diagnosis by this simple, rapid and inexpensive procedure. A case of intramuscular bacillary angiomatosis was diagnosed on thin needle aspiration of a subcutaneous mass in a patient with AIDS (Sanchez and Rorat, 1996). Besides inflammatory cells, the aspiration smears in this case contained clumps of amphophylic granular material containing small bacterial rods demonstrated by silver stain. The organisms belonging to the genus Rochalimacea (now Bartonella) are also involved in cat scratch disease (see Chap. 31).
be very numerous in skin lesions of the lepromatous form, can also be recognized in aspiration smears (Singh et al, 1996). Other applications of this technique are to subcutaneous abscesses or infected cutaneous cysts that may also yield a diagnosis by this simple, rapid and inexpensive procedure. A case of intramuscular bacillary angiomatosis was diagnosed on thin needle aspiration of a subcutaneous mass in a patient with AIDS (Sanchez and Rorat, 1996). Besides inflammatory cells, the aspiration smears in this case contained clumps of amphophylic granular material containing small bacterial rods demonstrated by silver stain. The organisms belonging to the genus Rochalimacea (now Bartonella) are also involved in cat scratch disease (see Chap. 31).
Viral Disorders
Molluscum Contagiosum
The large size pox virus infects hair follicles and typically produces multiple umbilicated lesions on the surface of the skin which, however, when single, may mimic a basal cell carcinoma. Smears of these lesions are easily obtained by squeezing the lesion and expelling its core on a slide that may be immediately examined after methylene blue staining (Canti, 1984). The smears show a large number of “molluscum bodies,” which are squamous cells filled with masses of viral particles, displacing the nucleus to the periphery (Fig. 34-2B). For comments on herpesvirus infection, see below.
BULLOUS DISEASES OF THE SKIN
Tzanck (1947) was the first to advocate the use of fresh smears for differential diagnosis of vesiculo-bullous diseases, e.g., bullous pemphigoid, herpesvirus infection, or toxic epidermal necrolysis. As discussed at length in Chapters 19 and 21, pemphigus vulgaris and its variants, known as pemphigus foliaceus and pemphigus vegetans, can be recognized because of numerous, dispersed, peculiar intermediate squamous cells with large nuclei and nucleoli (acantholytic cells of Tzank) (Fig. 34-3). The presence of bizarre multinucleated cells was emphasized by Tzanck but we have not observed them in our material, nor did Canti. Other forms of pemphigus, wherein the bullae are formed within the epidermis, such as familial pemphigus, may also show a small number of similar cells (Canti, 1984). For description of cytologic findings in Darier’s disease (that may also occasionally form skin vesicles), see Chapter 21.
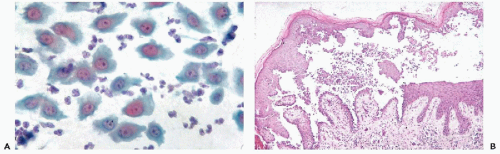 Figure 34-3 Pemphigus vulgaris. A. Tzanck’s cells with large, pale nuclei and prominent, sometimes multiple nucleoli. B. Cross-section of a skin vesicle containing Tzanck’s cells. (Case courtesy of Dr. G. Canti, London, UK.) |
Herpesvirus type I or II and herpes zoster infections form painful vesicles. The cell changes caused by these viruses are discussed at length in Chapter 10. Toxic epidermal necrolysis and other vesicle-forming lesions do not show any of these disease-specific changes but do show necrosis and inflammation (Canti, 1979, 1984).
RARE BENIGN DISORDERS
Amyloidosis
Blumenfeld and Hidebrandt (1993) reported on aspiration of abdominal fat for the diagnosis of amyloidosis in 17 patients in whom amyloidosis was clinically suspected. The presence of amyloid was documented in 8 patients by apple-green birefringence of amyloid stained with congo red.
Subcutaneous Fat Necrosis of Newborns
Subcutaneous fat necrosis occurs in infants subjected to various forms of trauma (Silverman et al, 1986). Gupta et al (1995) established this diagnosis in aspirated material by observing necrotic fat cells and crystals of fatty acids.
Endometriosis
Endometriosis in the form of nodules most often occurs in the abdominal wall in young women in the area of the umbilicus or in laparotomy scars. Subcutaneous endometriosis is an especially important point of differential diagnosis with primary or metastatic tumors (Leiman et al, 1986).
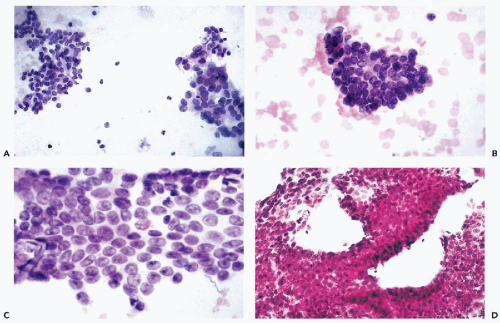 Figure 34-4 Endometriosis occurring in the scar of a Caesarian section. A. Clusters of small, spindly stromal cells (left) and larger glandular cells (right). B. Higher power view of a compact cluster of stromal cells. C. Higher power view of glandular cells forming a “honeycomb” cluster. Small nucleoli occur in some of the nuclei, a common finding in proliferative phase (see Chap. 13). D. Cell block of the lesion showing endometrial glands and stroma. (Case courtesy of Dr. J. Amberson, Dianon Systems, Stratford, CT.) |
The aspirate usually contains two families of cells: larger cells, representing the lining of the endometrial glands, and smaller, spindly cells of endometrial stroma (Fig. 34-4). Unless close attention is paid to the differences between these two cell populations, erroneous diagnoses of metastatic adenocarcinoma have been known to occur, sometimes with disastrous results (Ashfaq et al, 1994). The differential diagnosis becomes even more difficult if the stromal cells are decidualized, i.e., become large, decidual cells with abundant eosinophilic cytoplasm, as described by Berardo et al (1992). The knowledge of clinical history is essential in avoiding such errors.
PRIMARY NEOPLASMS
The application of cytologic techniques to tumors of the skin and skin adnexae is a natural extension of existing diagnostic procedures. In some institutions, scrape preparations have been found to be of value in rapid and inexpensive assessment of suspect neoplastic skin lesions (summary in Canti, 1984). Palpable nodular skin nodules may be sampled by aspiration with the help of very small caliber needles.
Benign Neoplasms
Seborrheic Keratoses
These soft, brown, elevated benign lesions of the sun-exposed skin are usually recognized clinically and rarely need biopsy confirmation. Histologically, the lesions show a proliferation of basal squamous cells with formation of small cystic areas filled with keratin. Basal cell and, very rarely squamous cell carcinomas, may develop in seborrheic keratosis; such lesions may become ulcerated and indurated. The diagnostic procedures of these rare lesions are the same as for carcinomas, described below. Canti (1979) described the smears as composed of nucleated and anucleated squamous cells without specific features.
Benign Tumors of Skin Adnexa
Benign and malignant tumors of the endocrine and apocrine sweat glands, hair or piliary apparatus are uncommon and show a wide spectrum of histologic patterns (Wick et al, 1985). The benign tumors are occasionally aspirated to rule out a primary or metastatic malignant tumor. Layfield and Mooney (1998) reported a case of a benign hydradenoma of the skin. We have seen a misleading case of clear cell hidradenoma in a young woman with a history of treated adenocarcinoma of the uterine cervix that was thought clinically
to be a metastasis. The aspirate contained small epithelial cells with hyperchromatic nuclei occurring singly and in clusters (Fig. 34-5A-C). The clear cytoplasm of some of the cells contributed to the erroneous diagnosis of metastatic adenocarcinoma. Excisional biopsy of the nodule disclosed a clear cell hidradenoma (Fig. 34-5D). Courtesy of Dr. G. Canti, we also examined a smear of an adenoma of a sebaceous gland. The smear contained a cluster of large cells with faintly granular, abundant cytoplasm, resembling fat cells (Fig. 34-6).
to be a metastasis. The aspirate contained small epithelial cells with hyperchromatic nuclei occurring singly and in clusters (Fig. 34-5A-C). The clear cytoplasm of some of the cells contributed to the erroneous diagnosis of metastatic adenocarcinoma. Excisional biopsy of the nodule disclosed a clear cell hidradenoma (Fig. 34-5D). Courtesy of Dr. G. Canti, we also examined a smear of an adenoma of a sebaceous gland. The smear contained a cluster of large cells with faintly granular, abundant cytoplasm, resembling fat cells (Fig. 34-6).
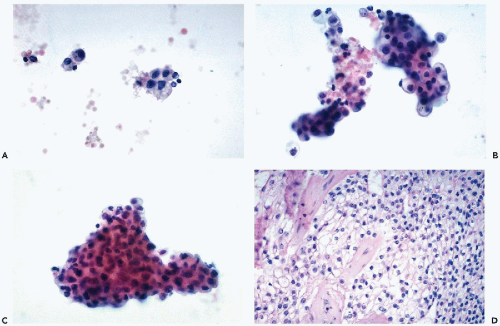 Figure 34-5 Clear cell hidradenoma mimicking metastatic adenocarcinoma. A-C. The aspirate contained spherical or cuboidal cells in small and large clusters. The nuclei, although spherical, were hyperchromatic. The cytoplasm of most cells was clear. D. Histologic section of the encapsulated tumor, documenting the diagnosis of hidradenoma. |
Fat-containing tumors, known as xanthogranulomas, and occurring mainly in infants and children, have been reported (Janney et al, 1991). Besides multiple macrophages, the lesions contained multinucleated giant cells (Grenko et al, 1996).
Pilomatrixoma (Calcifying Epithelioma of Malherbe)
These tumors, which occur mainly but not exclusively in young people, form chalky-white subcutaneous nodules, usually located on the face, neck, or upper extremities, sometimes underneath pigmented skin. The cytology of this tumor was first described in needle aspirates by Woyke et al (1982). The aspirates of these tumors contain small basophilic cells, singly and in clusters, admixed with nucleated and anucleated squames, the latter forming clusters of yellowish “ghost” cells. Calcified material and foreign body giant cells round out the spectrum of features (Fig. 34-7). Numerous errors of diagnosis have been committed in the past mistaking pilomatrixoma for squamous carcinoma (Gomez-Aracil et al, 1990; Koss et al, 1992; Domanski and Domanski, 1997). In recent reports, the features of pilomatrixoma have been better recognized and no errors of identification were made (Viero et al, 1999).
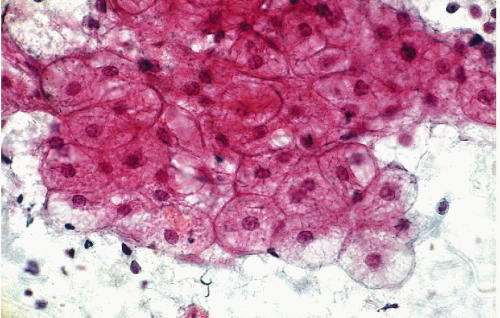 Figure 34-6 Sebaceous adenoma. The cell cluster is composed of large cells with faintly granular cytoplasm, resembling fat cells. (Courtesy of Dr. G. Canti, London, UK.) |
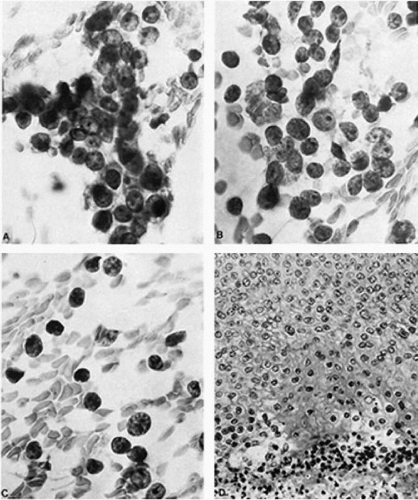 Figure 34-7 Pilomatrixoma of the upper eyelid. A-C. Aspirate, high magnification. A. A cluster of tumor cells with scanty cytoplasm and large vesicular nuclei of fairly even sizes with distinct nucleoli. B,C. Tumor nuclei stripped of cytoplasm. Note the distinct large nucleoli and evenly distributed chromatin. Some variation in nuclear size may be seen. D. Tissue section. The epithelial portion of the tumor consists of cells with vesicular nuclei and distinct nucleoli. There is a transition to an area of shadow cells and amorphous debris (bottom) with pyknotic nuclei (high magnification). (From Woyke S, Olszewski W, Eichelkraut A. Pilomatrixoma. A pitfall in the aspiration cytology of skin tumors. Acta Cytol 26:189-194, 1982
Get Clinical Tree app for offline access
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree


|