which are similar to squamous pearls and are dispersed throughout the thymus, are formed by epithelial cells (Fig. 37-2D). During the maturation in the thymus, T-lymphocytes (so named because of their thymic origin) are located within spaces formed by the epithelial cells. The lymphocytes, enveloped by the epithelial cells, form so-called lymphoepithelial complexes. T-lymphocytes, unlike the B-lymphocytes, express both CD-4 and CD-8 antigens. In an interesting observation by Nerurkar and Krishnamurthy (2000), which has not yet been confirmed by others, penetration of lymphocytes into the epithelial cells (or emperipolesis) was demonstrated in imprint cytology of the normal thymus.
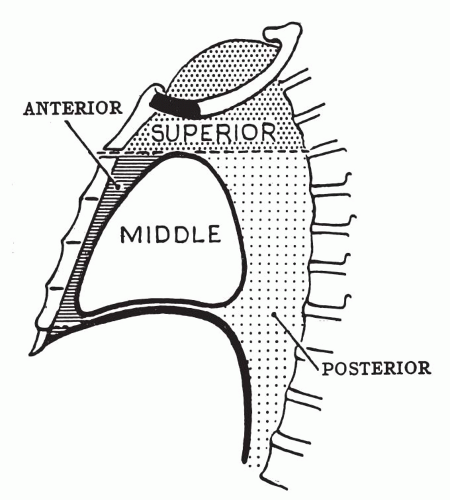 Figure 37-1 Diagrammatic representation of mediastinal compartments. |
TABLE 37-1 MOST COMMON PRIMARY TUMORS AND SPACE-OCCUPYING LESIONS ACCORDING TO COMPARTMENTS OF THE MEDIASTINUM | ||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
rare immune disorders. Like myasthenia gravis, these disorders may be the first manifestation of thymoma.
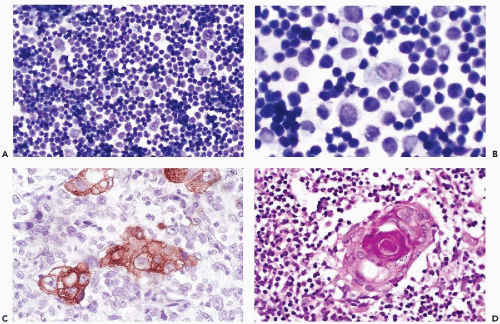 Figure 37-2 Normal thymus. A. Histology showing a network of large epithelial cells among many small lymphocytes (thymocytes). B. Imprint of a normal thymus under oil immersion. The epithelial cells have large, smoothly contoured nuclei with a delicate chromatin structure and occasional chromocenters or nucleoli. Cytoplasm is abundant and lightly stained, with indistinct cytoplasmic borders. C. Cytokeratin stain brings out the cytoplasm of the epithelial cells; lymphocytes are negative. D. Hassall’s corpuscle, a benign squamous pearl. (A,B: Diff-Quik stain.) |
and invasive. In our experience, the best evidence of malignant potential is invasion through the capsule and into the lung or other tissues. The cytology of frankly malignant thymomas (carcinomas) is considered separately below.
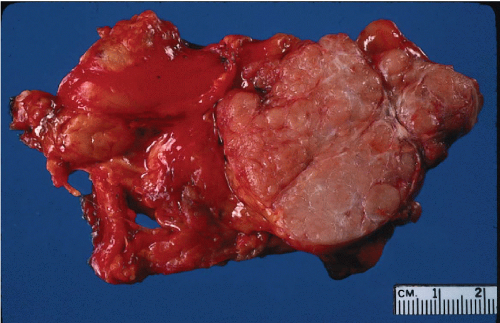 Figure 37-3 Gross appearance of a thymoma. The tumor is sharply circumscribed and soft, pale brown or tan on the cut surface. It is adherent to the adjacent lung (left) but noninvasive. |
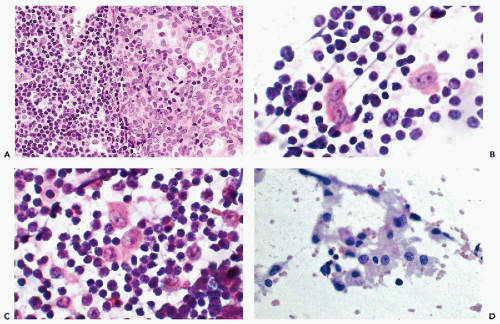 Figure 37-4 Thymoma. A. Histologic section showing sheets of epithelial cells with large round or ovoid vesicular nuclei and pale staining cytoplasm with indistinct nuclear borders. Compare with the many small lymphocytes present. B,C. At higher magnification, a tumor imprint showing several single thymic epithelial cells with abundant cytoplasm and large round or ovoid nuclei with delicate nuclear chromatin and prominent chromocenters or small nucleoli. D. FNA of another thymoma showing epithelial cells in coherent clusters, in strands of cells and single cells. |
intermixed with lymphocytes, should suggest the possibility of thymoma, Slagel et al (1997) reviewed 22 cases of mediastinal tumors in which the needle aspirate contained a predominant spindle cell component, and found only two thymomas and two thymic cysts. The remaining cases included nerve sheath tumors, granulomatous inflammation, Hodgkin’s disease, and a heterogenous group of other tumors.
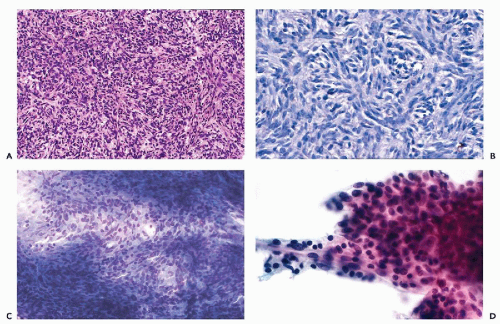 Figure 37-5 Spindle cell thymoma. A. The thymic epithelial cells form interlacing bands of elongated cells with thin, spindle-shaped nuclei. B. High magnification to demonstrate the spindle cell configuration and pattern of thymic tumor cells. C. Diff-Quik stain of the cytologic specimen. D. FNA of another case. Note that the tumor cells, which are oval or spindly and uniform, are in clusters or tissue fragments. A spindle cell tumor in the needle aspirate of an anterior mediastinal mass should be considered thymoma until proved otherwise. |
Positive chromogranin staining of tumor cells can be used to confirm the diagnosis when in doubt.
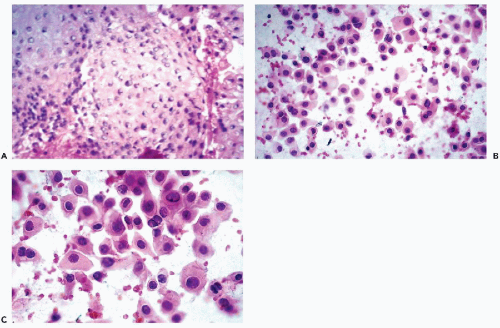 Figure 37-6 Thymic carcinoma. A. Histologic section showing an epidermoid pattern of carcinoma arising in thymus. B,C. Needle aspirate showing abundant malignant cells similar to those of a squamous carcinoma. |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


