aspiration (FNA) of the kidney. Dean (1939) first reported the treatment of a solitary cyst of kidney by aspiration. Söderström (1966) described a large experience with this method, and Von Schreeb et al (1967), Kristensen et al (1972), Thommesen and Nielsen (1975), Edgren et al (1975), and Holm et al (1975) each reported a series of cases.
Cystic lesions (as a diagnostic and therapeutic procedure)
Lesions with equivocal radiologic findings
Confirmation of diagnosis in advanced malignant lesions prior to nonsurgical treatment
Confirmation of local recurrence at the site of a prior tumor or a direct extension from neighboring site (e.g., colon or adrenal)
Confirmation of metastatic cancer
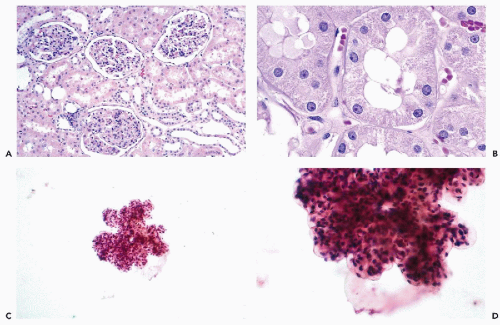 Figure 40-1 Histology and cytology of the normal kidney. A. Glomeruli and proximal convoluted tubules with pink granular cytoplasm are the predominant component of the cortex. Smaller cuboidal cells with pale cytoplasm line the distal tubule). B. Proximal tubules at high magnification. C,D. Renal glomerulus at low and high magnification. In aspiration smears, the glomeruli are seen as thick, three-dimensional, lobulated structures. The anatomic relationship among the endothelial, epithelial, and mesangial cells is lost. |
are often observed. However, unless a large-bore needle is used, intact glomeruli are rarely encountered (Fig. 40-1C,D).
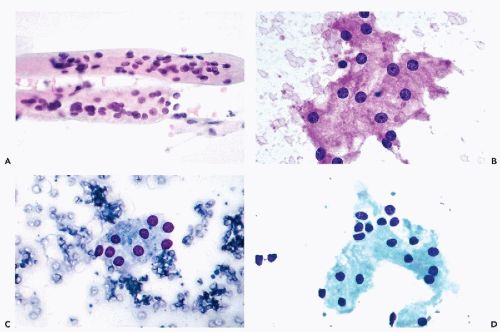 Figure 40-2 A. Whole renal tubules in aspiration smears. B. Proximal tubular cells. Note that the majority of the nuclei are separated from each other by pink granular cytoplasm. C,D. Tubular cells forming sheets in MGG-stained smears. Note the uniformity of the cells and their small nuclei. |
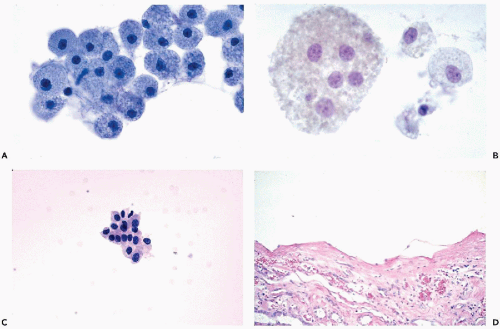 Figure 40-3 Renal cyst aspirates. A. Large mononucleated macrophages with finely vacuolated cytoplasm are the cells typically seen in clear, straw-colored cyst fluid. B. Multinucleated macrophage in cyst fluid. C. A small, tight cluster of benign epithelial cells, corresponding to the excised renal cyst shown in D. |
yields bloody fluid with high fat and protein but low LDH levels.
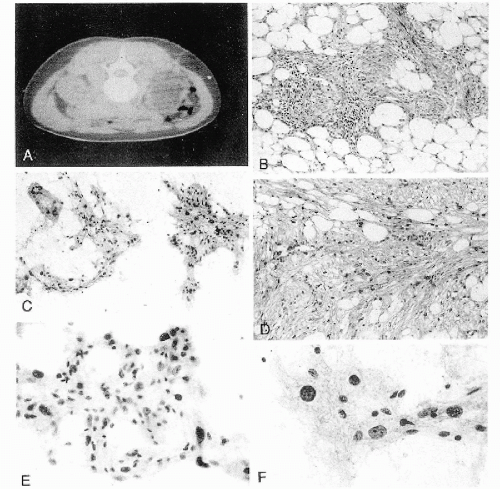 Figure 40-4 Angiomyolipoma. Angiomyolipoma of the left kidney in a 34-year-old woman with no evidence of tuberous sclerosis. A. Computed tomography (CT) revealed the tumor in the lower pole of the right kidney. The patient was in a prone position. The CT features were characteristic of angiomyolipoma, notably because of the presence of clear areas representing fat within the tumor. B,D. Tissue sections. B. Numerous thick-walled vessels, smooth muscle cells, and fat are present. D. Bundles of smooth muscle cells. Note the presence of pleomorphic, atypical nuclei. C,E,F. Aspirate. C. Irregular tissue fragments containing smooth muscle cells, fat, and vessels. E. Tissue fragment. Note the irregular arrangement of the nuclei and their variable sizes. F. Group of cells with abundant cytoplasm. Note the significant differences in nuclear sizes. Most of the nuclei are hyperchromatic, but their contour is smooth. These cytologic features may lead to an erroneous diagnosis of a carcinoma or a sarcoma. (From Koss et al. Aspiration Biopsy. Cytologic Interpretation and Histologic Bases, 2nd ed. New York: Igaku-Shoin, 1992.) |
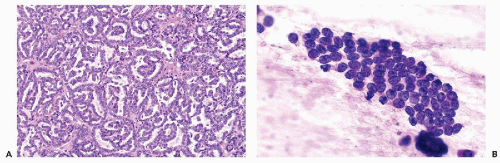 Figure 40-5 Metanephric adenoma. A. Histology. Closely packed tubular structures with papillary infolding (glomeruloid bodies). The tumor cells are monotonous and small with scanty cytoplasm. B. Touch-preparation of a nephrogenic adenofibroma (see text). |
TABLE 40-1 CLASSIFICATION OF RENAL CELL NEOPLASMS | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
related to papillary RCC, which shows similar findings (Brown et al, 1997). We recently encountered a case of papillary carcinoma that arose in a metanephric adenoma, confirming the relationship between the two lesions.
tumors invade beyond Gerota’s fascia, or are metastatic to distant organs. Metastases to regional lymph nodes upstages stage 1 and 2 tumors to stage 3 tumors.
TABLE 40-2 RENAL CELL NEOPLASMS: PRESUMED CELL OF ORIGIN AND CYTOGENETIC ABNORMALITIES* | |||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||
TABLE 40-3 FUHRMAN’S GRADING OF CONVENTIONAL RENAL CELL CARCINOMA | ||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
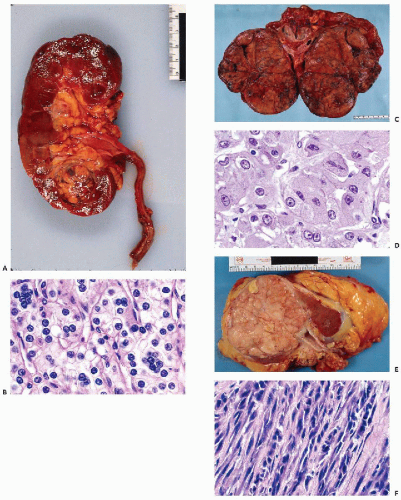 Figure 40-6 Conventional renal cell carcinoma (RCC). A. Gross picture of a 2-cm conventional RCC in the inferior pole of left kidney. The tumor was asymptomatic, an incidental finding on imaging. Note the golden-yellow cut surface. B. Histology: conventional RCC, clear cell type. Note the microtubule or acinar pattern and multiple nuclei in many cells. This is a grade 1 tumor. C. RCC with predominantly granular cells. The gross appearance is dark yellow to brick red. This large tumor (16 cm in diameter) presented as a left abdominal mass and flank pain. D. Histology of conventional RCC with predominantly granular cells. Note the presence of cytoplasmic vacuoles containing fat and glycogen. The nuclei are larger and some irregularly shaped, with visible nucleoli; therefore, this is a grade 2 tumor. E. Conventional RCC with predominantly sarcomatoid growth. The gross appearance is fleshy white. F. Histology of spindly (sarcomatoid) RCC. |
TABLE 40-4 MORPHOLOGIC VARIANTS OF CONVENTIONAL RCC | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
|
that is often filled with numerous small vacuoles containing lipid and glycogen but not mucin (Fig. 40-7B). The vacuoles are better seen in air-dried smears processed with hematologic stains. Phagocytosed hemosiderin may be seen. The nuclei are relatively small, but still much larger than those of benign tubular cells. They are only slightly pleomorphic, haphazardly placed, usually hyperchromatic, and contain readily visible nucleoli.
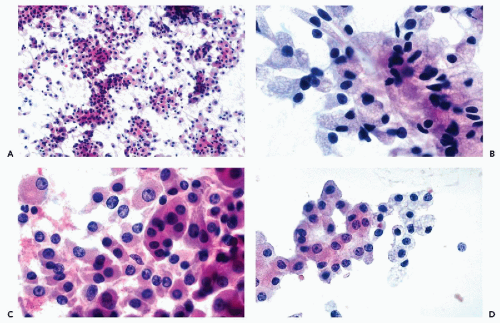 Figure 40-7 FNA appearance of conventional RCC with a mixture of clear and granular cells. A. Loosely cohesive flat groups of large cancer cells. Many single cells are present. B. High magnification reveals abundant, finely vacuolated cytoplasm and relatively small, hyperchromatic nuclei in large cancer cells of various configurations. C. Adjacent field shows predominantly granular cancer cells with eosinophilic cytoplasm. D. Another example of a renal smear showing side-by-side cancer cells with clear and granular cytoplasm. |
well-differentiated hepatomas was absent in RCC (see Chap. 38).
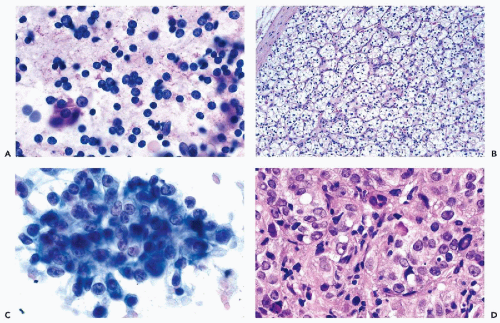 Figure 40-8 FNA of low- and high-grade renal carcinomas. A. FNA of a small RCC (shown in Fig. 40-6A) shows numerous well preserved “naked” nuclei, with some cells still retaining their eosinophilic granular cytoplasm. B. Histology of the same case shows a low-grade (grade 1) conventional RCC, clear cell type. C,D. Cells of a high-grade RCC with clear, scanty cytoplasm forming a cluster. B. Corresponding histology is from metastasis to the liver (core biopsy). |
TABLE 40-5 RENAL CELL TUMORS WITH GRANULAR CYTOPLASM | ||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||
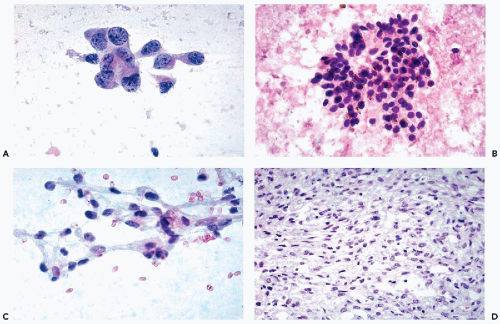 Figure 40-9 A. Renal carcinoma with pleomorphic cells. Pleomorphic cancer cells with abundant cytoplasm and large irregular nuclei. Such cells are usually observed in very high-grade tumors, but may also represent metastatic cancer. B. Conventional RCC with small cells. Undifferentiated small cells with scanty clear cytoplasm. The presence of phagocytosed hemosiderin is in favor of an RCC. C,D. Spindle cell carcinoma of the kidney. C. Elongated cancer cells with clear cytoplasm. Although the nuclei are hyperchromatic and of variable sizes, they are not conspicuous. D. Corresponding histology. Such findings are not uncommon in metastatic sites, where they may be mistaken for a sarcoma. |
nucleoli of moderate sizes are often present. The neoplastic cells often contain large amounts of ingested hemosiderin (Fig. 40-10). Psammoma bodies are not uncommon, particularly in tumors with large cells. Solid variants of PRCC have been described based on cytogenetic findings (Renshaw et al, 1997).
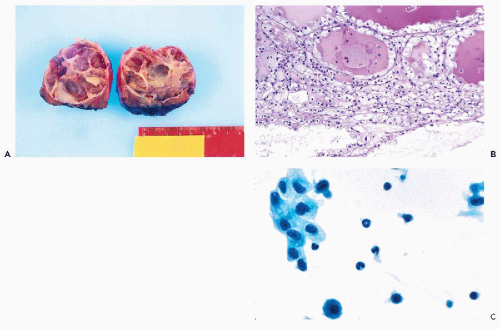 Figure 40-10 Multilocular cystic RCC. A. Gross appearance of a multilocular cystic RCC. B. Histologic sections of light-yellow areas show a grade 1 conventional RCC with cystic changes. FNA of multilocular RCC may be unrewarding (see text). C. Sparse tumor cells with clear and vacuolated cytoplasm in a background of macrophages and leukocytes. |
in most cases is very pale and transparent (typical chromophobe tumors) or, in some cases, eosinophilic and granular (Fig. 40-12D).
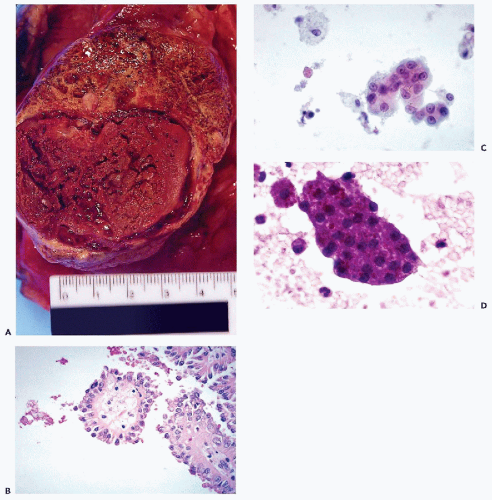 Figure 40-11 Papillary RCC (PRCC). A. Large PRCC with intramural hemorrhage. The upper portion of the tumor with a yellowtan appearance showed abundant foamy macrophages. B. Histology reveals neoplastic papillary fronds with large foamy macrophages in the center. C. Aspiration smear of a papillary renal carcinoma showing a large papillary cluster of epithelial cells with large, bland nuclei and tiny nucleoli. There are numerous large macrophages in the background. D. Numerous hemosiderin crystals are seen in this papillary frond of neoplastic cells from another case. |
Characteristically, the cells stain strongly with Hale’s colloidal iron, express epithelial membrane antigen (EMA), and are vimentin-negative (see Table 40-5).
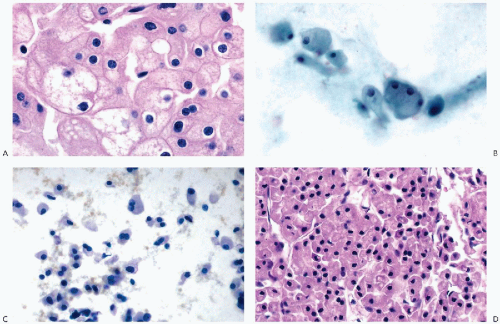 Figure 40-12 Chromophobe RCC (ChRCC). A. Histology of the classic ChRCC. Note that the pink, granular cytoplasm is condensed at the periphery, with many cells showing perinuclear clearing. B. Cytology of ChRCC. The cells show abundant fluffy cytoplasm with central clearing and peripheral nuclei. C. Eosinophilic variant of ChRCC metastatic to the liver. Note the cells with peripheral nuclei. D. Cell block of the same case. (C: Pap stain, × 400.) |
of well-differentiated oncocytes with small nuclei, the prognosis is excellent and the tumor is considered to be benign. However, there have been reports that at least some tumors may invade the parenchyma of the kidney and may recur (Rodriguez et al, 1980; Lieber et al, 1981). For tumors diagnosed as oncocytomas that produce metastases, the possibility of misclassification must be considered. As an example, we recently reviewed a case that was initially classified as oncocytoma and was resected in 1985. Two years later, a mass in the liver was discovered and aspirated. The FNA smears strongly suggested that the cells represented metastatic renal tumor. The “oncocytoma” from 1985 was reclassified as ChRCC (Fig. 40-12A,B). Also, oncocytomas may be associated with conventional RCC (Klein and Valensi, 1976; Fromowitz and Bard, 1990).
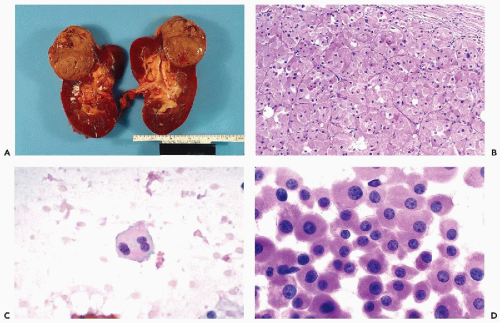 Figure 40-13 Oncocytoma. A. Gross appearance of an oncocytoma. The tumor is often subcapsular, uniformly tan to mahogany brown, and may show blood-filled microcysts but no necrosis or hemorrhage. B. Histology of the oncocytoma: very large uniform cells with dense, pink, granular cytoplasm and disproportionately small, uniform nuclei. The cells are supported by delicate fibroconnective tissue. C,D. Oncocytomas in aspiration biopsies. Note the faintly granular, eosinophilic granular cytoplasm and small nuclei. |
of which have granular cytoplasm (Fig. 40-14A), and of nests of clear cells embedded in fibroblastic stroma that is sometimes very dense. Mucin may be present in some of the glandular structures. Adjacent renal tubules may show dysplastic changes (Kennedy et al, 1990), and psammoma bodies may be present.
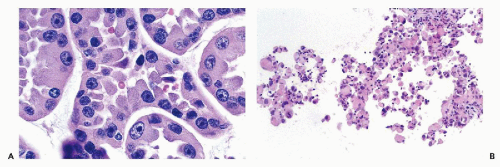 Figure 40-14 Histology of collecting (Bellini) duct carcinoma. A. Neoplastic ducts/tubules are lined by cancer cells with eosinophilic cytoplasm and large, hyperchromatic nuclei with prominent nucleoli. Mucin vacuoles may be seen. B. Cell block of FNA of medullary carcinoma. The microscopic presentation is not specific. |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


