The skin is the largest organ of the body and the first line of defense. Hair, nails, glands, and the skin make up the integumentary system. The skin functions to protect and insulate underlying structures, activate vitamin D, and assist with immune regulation, and it serves as a calorie reserve. The skin mirrors our emotions and stresses and impacts how others relate to and treat us. In a lifetime, the skin may be cut, bitten, irritated, burned, or infected. The skin has enormous resilience and capacity for recovery.
● Physiologic Concepts
STRUCTURE AND FUNCTION OF THE SKIN
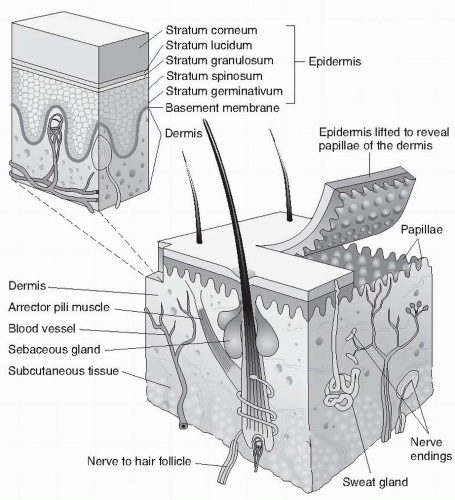
The skin is composed of three layers, each consisting of different cell types and serving different functions. The three layers are the epidermis, dermis, and subcutaneous layer. A diagram of the skin is shown in Figure 5-1.
Epidermis
The outermost layer of the skin, the epidermis, is fairly thin all over the body except for the palms of the hands and soles of the feet. The cells of the epidermis continually undergo mitosis and are replaced approximately every 30 days. The epidermis contains sensory receptors for touch, temperature, vibration, and pain.
The main component of the epidermis is the protein keratin, produced by cells called keratinocytes. Keratin is an extremely durable, tough substance that is insoluble in water. Keratin prevents the loss of body water and protects the epidermis from irritants and infection-causing microorganisms. Keratin is the main component of the skin appendages: the nails and the hair.
FIGURE 5-1 Three-dimensional view of the skin. (From Porth, C. & Matfin, G [2009]. Pathophysiology, concepts of altered health states [8th edition]. Philadelphia: Lippincott Williams & Wilkins.)
Melanocyte cells are present at the base of the epidermis. Melanocytes synthesize and secrete melanin in response to stimulation by melanocytestimulating hormone, which is produced by the anterior pituitary. Melanin is a black pigment which disperses throughout the epidermis to give color pigmentation to the skin and protect cells from ultraviolet (UV) radiation.
Immune cells, called Langerhans’ cells, or dendritic cells, are present throughout the epidermis. The cells originate in the bone marrow but are deposited in the deep layer of the epidermis early in life. Langerhans’ cells recognize foreign particles or microorganisms that enter the skin and present them to T lymphocytes as the first step in initiating an immune attack. Langerhans’ cells may be responsible for recognizing and eliminating dysplastic or neoplastic skin cells. Langerhans’ cells are physically associated with sympathetic nerves, suggesting a relation between the nervous system and the ability of the skin to fight off infection or prevent skin cancer. Stress may affect the functioning of Langerhans’ cells by increasing sympathetic stimulation. UV radiation may damage Langerhans’ cells, reducing their ability to prevent cancer.
Merkel cells or tactile epithelial cells provide sensory information. They connect to sensory nerve endings and serve as light touch receptors.
Dermis
Lying immediately under the epidermis, the dermis is considered loose connective tissue and is composed of fibroblast cells that secrete the proteins collagen and elastin. The collagen and elastin fibers are arranged haphazardly, giving the dermis distensibility and resilience. A gel-like substance, hyaluronic acid, is secreted by the connective tissue cells. Hyaluronic acid surrounds the proteins and gives the skin elasticity and turgor (tension). In addition to the protective function, the dermis also serves as a reservoir for water and electrolytes. Throughout the dermis are blood vessels, sensory and sympathetic nerves, lymphatic vessels, hair follicles, and sweat and sebaceous glands. The somatic sensory receptors in the dermis process sensory information such as touch, pressure, pain, and temperature. Mast cells, which release histamine during injury or inflammation, and macrophages, which phagocytize dead cells and microorganisms, are also present.
Blood vessels in the dermis supply the dermis and epidermis with nutrients and oxygen and remove waste products. Dermal blood flow offers a means for the body to control its temperature. With a decrease in body temperature, sympathetic nerves to the blood vessels are activated and increase the release of norepinephrine, causing constriction of the vessels and a conservation of body heat. If body temperature is too high, sympathetic stimulation of the dermal blood vessels is reduced, dilating the vessels and allowing for the transfer of body heat to the environment. Arteriovenous (AV) connections, called anastomoses, are present on some blood vessels. AV anastomoses facilitate skin temperature regulation by allowing blood to bypass the upper layers of the dermis in times of severe cold. Sympathetic nerves to the dermis also innervate sweat glands, sebaceous (oil) glands, and hair follicles.
Subcutaneous Layer
Although not always considered a part of the skin, the subcutaneous layer or hypodermis lies beneath the dermis and connects skin with underlying body structures. The subcutaneous layer of the skin is composed of fat and connective tissue and acts both as a shock absorber and a heat insulator. The subcutaneous layer is a calorie reserve station as well: fat can be stored in this layer and, if needed, broken down to serve as an energy source.
HAIR AND NAILS
The nails are keratinized plates that extend from the fingers and the toes. The nails protect the fingertips and are most likely evolved with an original purpose of defense. A layer of epithelium underneath the nail is the nail bed. The nail bed is highly vascular and monitoring the color of the nail beds can offer valuable information about oxygenation of the blood.
The hair is hardened keratin that grows at variable rates on different parts of the body. The lanugo which covers the fetus in utero is replaced by vellus hair before or shortly after birth. This hair is strong, fine, and less pigmented. Terminal hair that appears around puberty in the pubic and axillary area is coarse. Hair grows as a follicle shaft in a canal, beginning deep in the dermis. In addition to a hair follicle, each canal contains a sebaceous gland and a smooth muscle fiber, called an arrector pili muscle. When this muscle cell is stimulated by the sympathetic nervous system, it causes the hair to stand on end. Hair on the head may protect against sunburn. Hair color is largely determined by the amount, type, and distribution of melanin. With aging, hair turns white because of the inability to continue melanin production.
SEBACEOUS GLANDS
The sebaceous glands accompany the hair follicles. They secrete an oily substance called sebum into the surrounding canal to prevent damage to the surrounding hair and skin. Sebaceous glands are present all over the body, especially on the face, chest, and back. Testosterone increases the size of the sebaceous glands and the production of sebum. Testosterone levels increase in males and females during puberty.
SWEAT GLANDS
There are two types of sweat glands: eccrine and apocrine. Eccrine sweat glands open directly onto the surface of the skin and are distributed over the entire body. Eccrine glands function mainly in cooling the body by means of evaporative heat loss. They are especially concentrated on the hands, feet, and forehead. Apocrine glands are mainly located in the axillae (armpits) and in the pubic and anal areas. These glands secrete sweat into the canals of the hair follicles. When acted upon by surface bacteria, the secretions of the apocrine glands cause the characteristic odor of perspiration.
VITAMIN D
The skin plays a vital role in the body’s use of vitamin D. Vitamin D is a hormone obtained in the diet in an inactive form. It is required both for the absorption of calcium from the gut and in order to reduce the renal excretion of calcium. For vitamin D to function, however, it first must be activated by the body. The initial step in vitamin D activation occurs in the skin as a result of UV radiation, after which it is further acted upon by the kidney and the liver. Vitamin D activation is increased in response to a decrease in serum calcium. Because vitamin D acts as a hormone, the skin may be considered an endocrine gland.
● Pathophysiologic Concepts
Many different lesions occur on the skin. They are described on the basis of size, depth, color, and consistency. See pages C3, C4, C5, and C6 for illustrations of common skin lesions.
BULLA
Measuring more than 1.0 cm in diameter and filled with watery fluid, a bulla is a large, raised area on the skin. Bullae are large blisters that can occur after a burn.
CRUST
A crust is the accumulation of dried serous (serum-like) or seropurulent (pus) exudate on the skin (e.g., the crust seen on an impetigo or herpes lesion). It is usually golden in color.
CYST
An elevated, circumscribed encapsulated lesion in the dermis or subcutaneous layer is called a cyst. It may be filled with liquid or a semisolid substance.
EROSION
An erosion is an area on the body characterized by the loss of superficial epidermis. Typically the area is depressed, moist, and glistening but does not bleed (e.g., the skin after bursting of a blister or vesicle).
EXCORIATION
An excoriation is a scratch on the skin with loss of the epidermis (e.g., a skinned knee). It may be a hollowed-out, crusted area with slight bleeding.
FISSURE
A fissure is a linear crack in the skin from the epidermis to the dermis, for example, as seen with athlete’s foot. The fissure may be pink or red, dry or moist, and usually there is no bleeding.
KELOID
A keloid is a scar formation on the skin, occurring after a trauma, injury, or piercing, that is out of proportion to the injury. Keloids are caused by excessive collagen formation during the healing process. They appear raised, red, and firm. There is a genetic tendency to develop keloids, and this type of scarring is especially common in African Americans. An individual prone to keloid formation should alert a health care provider when a skin injury occurs. Prevention of keloid formation is supported by careful surgical techniques, pressure dressings, good wound care, and adequate nutrition. There is no single best treatment for an existing keloid, although topical dressings, steroid injections, and laser therapy all have been used with some success. Immunotherapy is under investigation. Removal of a keloid may worsen scarring in some cases.
LICHENIFICATION
Thickened, roughened skin that may occur with constant irritation is known as lichenification. This condition is seen, for example, in skin with atopic dermatitis.
MACULE
A macule is a flattened area of the skin, characterized by a change in color. A macule (e.g., a freckle or a flat mole, also called a nevus) is typically smaller than 1.0 cm in diameter.
NODULE
A nodule is a solid, elevated mass measuring between 1.0 cm and 2.0 cm in diameter. It is firmer in consistency than a papule and occurs deeper in the dermis (e.g., a cyst).
PAPULE
A papule is a solid, elevated mass, smaller than 1.0 cm in diameter. Examples of papules include elevated moles and warts.
PATCH
A patch is a flat, nonpalpable irregularly shaped macule measuring greater than 1.0 cm in diameter. Examples include vitiligo, Mongolian spots, and port-wine stains.
PETECHIA
A deep red spot of pinpoint hemorrhage under the skin is called petechia. Petechiae may signify a bleeding disorder or fragility of the capillaries and may accompany a serious infection.
PLAQUE
A plaque is a raised surface with a flat top and measures larger than 1.0 cm. Examples of plaques are several papules grouped together or the lesions seen with psoriasis.
PRURITUS
Pruritus refers to itching of the skin. Pruritus may occur as a primary response to a surface irritant or inflammation, for example, after a mosquito bite, or with dry skin. Primary pruritus results from release of histamine during inflammation. Pruritus may occur secondarily to a systemic disease, such as liver or kidney failure. With systemic disease, metabolic toxins may accumulate in the interstitial fluid under the skin.
PURPURA
A purpuric lesion is a large patch of purple discoloration under the skin associated with hemorrhage. It may result from a variety of causes, including thrombocytopenia (decreased platelets), trauma (a “black and blue mark”), or an allergic response. A purpuric lesion occurring without trauma may be a red flag for bleeding elsewhere in the body, including the brain.
PUSTULE
A pustule is an elevated vesicle filled with pus. Examples of pustules are the lesions of impetigo or acne.
SCALE
An irregular collection of keratinized cells or a flake of epidermis is referred to as a scale. It may be thick or thin, dry or oily, and can vary in size. Examples of scaling are seen in dandruff or dried skin.
SCAR
A scar is an area of the body where the skin has been replaced by fibrous tissue (e.g., a burn scar). A scar may be thin or thick.
TELANGIECTASIA
Capillary dilation will manifest as fine, irregular lines such as seen with rosacea.
TUMOR
A tumor is a large, solid mass that is elevated and larger than 2.0 cm. Tumors may be neoplastic or benign, as, for example, a breast cancer versus a lipoma (a benign tumor made up mostly of adipose tissue).
ULCER
An ulcer is an area with loss of epidermal and deeper layers of the skin that may bleed and scar. Ulcers have a concave appearance and may vary in size. An example of an ulcer is a decubitus ulcer (pressure sore).
URTICARIA
Urticaria, also known as hives, consists of raised edematous plaques (wheals) associated with intense itching (pruritus). Urticaria results from the release of histamine during an inflammatory response to an allergen to which the individual has become sensitized. Chronic urticaria may accompany systemic disorders such as hepatitis, some cancers, or thyroid abnormality.
VESICLE
A vesicle is a small, raised circumscribed area on the skin with a measurement of less than 1.0 cm. It is formed by the presence of serous fluid within the skin layers (e.g., a chickenpox blister).
WHEAL
A wheal is a raised area of skin edema that exists only temporarily and itches (e.g., the area surrounding a mosquito bite or an area of the skin during an occurrence of urticaria [hives]). The center of a wheal is pink or red, with a surrounding circle of paler skin.
● Conditions of Disease or Injury
BENIGN SKIN DISORDERS
Cysts
A cyst is dome shaped, freely movable, pale, and ranges in size from 0.5 to 5 cm. It is filled with keratin and has a central opening which drains a pasty, malodorous substance. If it becomes infected, treatment may include antibiotics and surgical removal.
Keratoses
A horny overgrowth or abnormal growth of keratinocytes is referred to as keratosis. The most common premalignant skin lesions on sun-exposed areas are actinic keratosis. Beginning as hyperemic, poorly defined lesions, they develop into dry, brown, scaly macules with a reddish tinge and a rough surface. The lesions are typically less than 1 cm in diameter and the surrounding skin may have a weathered appearance. The lesions are more easily felt than visualized. Approximately 20% of actinic keratoses eventually convert to squamous cell carcinoma. Treatment may include cryosurgery, liquid nitrogen, or topical chemotherapeutic agents such as 5-fluorouracil or imiquimod creams. Aldara may be used to stimulate the immune system to remove the lesions.
Seborrheic keratosis is characterized by a sharply circumscribed round or oval wartlike lesion. It may be black, tan, brown, yellow, or pink in color and ranges in size up to several centimeters. Although benign, lesions need to be monitored for changes in color, size, or texture which may be indicative of malignant transformation.
Lipoma
A nodular collection of fat tissue under the skin is a lipoma. It is slow growing, freely movable, soft and may be up to several centimeters in diameter. Surgical removal is possible if desired for cosmetic reasons.
Nevi or Moles
Moles can be flat or raised, hairy or nonhairy and vary in color and size. Although harmless, moles should be monitored for changes in size, color, or texture which may be indicative of malignant transformation.
Skin Tags
Soft, brown, or flesh-colored papules seen in aging adults are skin tags. Ranging in size from pinpoint to pea sized, they most commonly develop on the neck, axilla, and intertriginous areas.
PIGMENTATION ALTERATIONS
Pigmentation alterations are the result of changes in normal skin color. Café-au-Lait spots and liver spots (solar lentigo) are two examples of hyperpigmentation. Café-au-Lait spots are flat cutaneous pigmentations ranging from 0.5 to 20 cm in diameter. They are considered benign, but six spots or more may be indicative of neurofibromatosis. Liver spots or age spots are sharply demarcated dark areas on sun-exposed skin. They generally occur in Caucasians over 60 years of age with a familial tendency. Prevention through limited sun exposure and the use of sunscreen is recommended. Bleaching creams may lighten the areas and for cosmetic purposes, skin resurfacing with laser and liquid nitrogen is an option.
An acquired or hereditary decrease in melanin causes a hypopigmentation of the skin. Vitiligo (leukoderma) is a localized loss of melanocytes in the skin and hair. White patches of skin with definite borders may appear on the face, neck, axillae, or extremities. Possible causes include pernicious anemia, hyperthyroidism, autoimmune disease, or inhibition of melanogenesis.
ALLERGIC AND HYPERSENSITIVITY DISORDERS
An inappropriate or exaggerated response of the immune system is referred to as hypersensitivity. Allergic responses are one type of immune hypersensitivity and may cause an immediate or a delayed response. Examples include atopic dermatitis, contact dermatitis, drug-induced skin eruptions, and urticaria.
Atopic Dermatitis
Atopic dermatitis (atopic eczema) is an inflammation of the skin involving overstimulation of T lymphocytes and mast cells. Histamine from the mast cells causes itching and erythema. Water loss from the epidermis and decreased skin lipid levels cause the skin to be dry. Scratching can cause skin breakdown. Atopic dermatitis is frequently seen in infants and children, but it may persist into adulthood. There appears to be a genetic tendency toward the disease and 75% to 85% have a personal or family history of allergic rhinitis or asthma.
Clinical Manifestations
Severe pruritus.
Periods of remissions and flare-ups.
Irregular, red papular patches, weepy, shiny, thickened.
Infantile characteristics include vesicle formation, oozing, crusting, excoriation, pale cheeks, extra creases under the eyes (Dennie-Mrogan folds), erythema.
Adult characteristics include dry red patches, leathery skin, lichenification, scaling, excoriation.
In infants, lesions often appear on the face, scalp, buttocks, extensor surfaces of the extremities. In older children and adults, the lesions appear more commonly on the hands, feet, neck, behind the knees, and in the bends of the elbows.
Diagnosis
Diagnosis is usually accomplished with the help of a good history and physical examination.
Infection of the skin with common surface bacteria, especially Staphylococcus aureus, or with viruses such as herpes simplex may develop. Individuals should avoid inoculation with live, attenuated viruses.
Thinning of the skin with continued steroid use.
Treatment
Avoidance of known irritants or allergens.
Use of emollients for skin hydration (limit number of baths and use tepid water with mild, unscented soap).
Antihistamines to help control itching.
Soft, light cotton clothing made of natural fiber.
Cool compresses to reduce inflammation.
Topical low-dose steroids to reduce inflammation and allow healing.
Minimize stress and temperature extremes to minimize vascular and sweat response.
Antibiotics as needed to prevent or treat secondary infections.
Contact Dermatitis
Contact dermatitis is an acute or chronic inflammation of the skin caused by exposure to an irritant (irritant dermatitis) or allergen (allergic dermatitis). The location of the dermatitis on the skin corresponds to the site of exposure. Allergic contact dermatitis occurs when Langerhans’ cells process and present an allergen to nearby T cells. The T cells respond with a type IV hypersensitivity response against the allergen. The response is delayed in that it takes hours to days to become evident. Several exposures may be incurred before a reaction occurs. The extent of the reaction is dependent on the duration and intensity of the exposure. Irritant dermatitis occurs when the skin is exposed to a substance that dries out or irritates it. Irritant dermatitis is only inflammatory and does not involve a specific immune response.
Common causes of allergic dermatitis include poison ivy or poison oak, latex, and chemicals found in jewelry. Common causes of irritant dermatitis include soaps, detergents, household cleaners, insecticides, and dusts. Some foods and spices may also cause contact dermatitis.
Clinical Manifestations
Both types of dermatitis present acutely with localized papules, erythema (redness), and oozing vesicles in an area of contact. The vesicles burst and crust.
Pruritus may be intense.
Allergic dermatitis typically presents 1 to 2 days after exposure.
Diagnosis
Dermatitis usually follows the pattern of exposure—for example, poison ivy typically travels vertically up the legs or may be present only on areas of the skin that were uncovered when exposed to the plant. A circle of lesions around the wrist may indicate an allergy to a bracelet or watch, whereas lesions below the umbilicus may indicate an allergy to the metal of a zipper. Reddened, irritated hands may indicate an inflammatory response to dishwashing. A good history accompanying the physical pattern is the key to diagnosis.
Allergy skin testing may be indicated.
Complications
Chronic conditions may cause lichenification, fissures, and scales.
An infection of the skin may result from repeated scratching and skin breakdown.
A severe response to poison ivy or another potent allergen may result in significant reddening and swelling of the face. The eyes may be closed because of edema.
Treatment
Identifying the cause of the dermatitis and avoiding exposure prevents recurrence.
Cool compresses reduce inflammation. Oatmeal soaks or baths in other soothing chemicals may provide relief. Antihistamines may be used to reduce itching.
Short-term, topical, anti-inflammatory, steroidal therapy may be used to interrupt the inflammation. For severe attacks involving the eyes and face, a burst of systemic corticosteroids is often used.
Drug-Induced Skin Eruptions
Many drugs can cause a local or generalized skin eruption although it occurs more commonly in females. T cells recognize the medication as a foreign substance and react. Cutaneous reactions typically occur within 7 days of drug exposure. Ampicillin, penicillin, cephalosporins, and barbiturates are the most common drugs causing a reaction. Reactions can range from a mild rash to epidermal skin detachment and bullous skin lesions (erythema multiforme minor, Stevens-Johnson syndrome, and toxic epidermal necrolysis).
Clinical Manifestations
Erythema, pruritus, urticaria
Maculopapular lesions in symmetrical, generalized distribution (face is usually not involved)
Fever and other systemic symptoms may also be present.
Diagnosis
Thorough history with specific questioning about any new medication. Also determine if this type of rash has occurred before and if so, what medications was the patient taking.
Complications
With extensive involvement, dehydration and hypothermia may occur.
Treatment
Discontinue the medication.
Antihistamines for itching.
Systemic corticosteroids for widespread or severe reaction.
Urticaria
Also referred to as hives, urticaria involves fluid leakage from the skin’s blood vessels. Histamine release from mast cells and basophils causes increased permeability of the microvessels in the skin and surrounding tissue. This permits fluid leakage into the tissues which results in edema and wheal formation. Acute urticaria is a result of an IgE-mediated response and chronic urticaria is associated with circulating IgG antibodies to IgE receptors. Common causes include food, medications, insect stings, viral infections, dust mites, and exposure to pollen. Some autoimmune conditions may also trigger urticaria.
Clinical Manifestations
Erythematous wheals. Raised red or pink areas surrounded by a paler halo. Blanch with pressure. Size varies.
Intense itching.
Angioedema may be present.
Diagnosis
History of exposure to a possible causative agent.
Complications
Angioedema of the face can cause airway compromise and temporary disfigurement.
Treatment
Avoid known triggers.
Antihistamines.
Leukotriene inhibitors.
Cold compresses or cool colloid-type baths.
Oral corticosteroids for refractory cases.
Epinephrine for angioedema of larynx and pharynx.
Tricyclic antidepressants with antihistamine actions may be used.
VIRAL INFECTIONS OF THE SKIN
A variety of viral infections may present with a skin rash. Many of these rashes are most common during childhood (Table 5-1) but may occur at any time. Herpes simplex virus (HSV) is the most common viral skin infection seen in adults.
Herpes Simplex 1 and 2
The herpesviruses include herpes simplex 1 and 2. Herpesviruses cause characteristic skin and mucous membrane lesions and are passed by viral shedding from the lesions. The incubation period for both viruses is approximately 2 to 24 days after infection. A prodromal period often precedes the appearance of lesions. During the prodromal period and the time of open lesions (a 2- to 6-week period), the virus is contagious. After an initial infection, the virus may lie dormant in the sensory nerve tract innervating the primary lesion. The dormant virus may become active again at any time, causing the reappearance of lesions. Reactivation of a latent herpes infection may occur with illness, stress, excessive sun exposure, or at certain times of the menstrual cycle. Severity worsens with age and is most severe in the immunocompromised individual.
TABLE 5-1 Common Childhood Rashes
Infection
Causative Agent
Characteristic of the Rash
Complications
Rubeola (10-day measles)
Paramyxovirus
Erythematous macular papular rash, beginning on face, moving to trunk and extremities; Koplik spots (pinpoint white) in mouth 1-3 days before rash
Measles encephalitis; secondary bacterial infection, including otitis and pneumonia
Rubella (3-day measles)
Rubella virus
Diffuse, red-pink macular rash beginning on face and trunk, spreading to extremities
Congenital rubella syndrome, if contracted by mother during pregnancy
Roseola
Herpesvirus 6
High fever followed approximately 3 days later by an erythematous macular rash, especially on the trunk
Unusual
Chickenpox
Herpes varicella-zoster
Macules, vesicles, and scabbings present at the same time. Intense itching
Varicella pneumonia, secondary bacterial infection, joint pain. Mothers infected during first trimester of pregnancy may suffer loss or congenital deformity of the fetus. Newborns infected at birth may have serious morbidity or mortality. Adults infected may become severely ill
Herpes simplex 2 is typically a genital or anal infection, whereas herpes simplex 1 is usually responsible for cold sores on the face. Either virus, however, is capable of infecting any site on the body. Herpes simplex 2 is considered a sexually transmitted disease.
Clinical Manifestations
Symptoms during the prodromal stage may include low-grade fever, malaise, and a burning or itching on the mouth or genitals.
With active infection, clusters of painful vesicles on a red base erupt on the lips, face, skin, nose, oral mucosa, genitalia, or anus. The vesicles may burn and itch. The vesicles rupture within 3 to 4 days and crust over. They usually disappear within the next week.
Diagnosis
Diagnosis is made by history and physical examination, although cell culture may be used to confirm a suspected outbreak.
Complications
Secondary bacterial infection of the vesicles may develop.
Herpes simplex may infect the eye, causing blindness (keratoconjunctivitis). A primary herpes simplex 2 infection during pregnancy may cause damage to the fetal central nervous system, including blindness and mental retardation. Risk to the fetus is especially high if the pregnant woman is exposed to the virus for the first time late in her pregnancy.
Neonatal infection by the virus may occur with an ascending vaginal or cervical infection during the pregnancy or during passage of the newborn through an infected birth canal.
Treatment
There is no cure.
Oral or topical treatment with an antiviral drug (acyclovir, famciclovir, valacyclovir), may reduce the frequency, duration, and intensity of the lesions. In some cases, these medications may be used as daily prophylaxis.
Lidocaine, diphenhydramine, and aspirin may decrease pain.
Cesarean section is performed if active genital herpes infection is present or if there is suspicion that the pregnant woman is in the prodromal stage.
Herpes Zoster
More commonly referred to as shingles, herpes zoster is a reactivation of the varicella-zoster virus in people who have previously had chickenpox. With reactivation, the virus that has been dormant in the dorsal root ganglia of the sensory cranial and spinal nerves travels from the ganglia to the skin corresponding to the dermatome. Factors that alter the body’s immunologic functioning (stress, medication, radiation, illness, and aging) may cause a reactivation. The majority of the estimated 1 million Americans affected annually are over 60 years of age. It is highly recommended that individuals over 60 years of age take the vaccine for herpes zoster. It has been shown to decrease the incidence of shingles as well as postherpetic neuralgia.
Clinical Manifestations
Varying levels of pain ranging from mild irritation to excruciating pain prior to eruption of the lesions.
Grouped vesicles on an erythematous base. Occur in a segmental distribution along the infected nerve. Typically occur unilaterally on the face, thorax, and trunk.
Vesicles dry and form crusts.
Diagnosis
Thorough history and classical distribution of lesions.
Polymerase chain reaction (PCR) directly identifies the virus and may be used.
Complications
Postherpetic neuralgia (pain) may occur in a large percentage (10% to 70%) of individuals suffering from shingles. Postherpetic neuralgia refers to pain that persists for longer than 1 month after the acute onset of shingles. It is most common in elderly patients and is difficult to relieve once it becomes established.
Secondary infection with necrosis in immunocompromised individuals.
Eye involvement can result in blindness.
Treatment
Antiviral agents such as acyclovir, famciclovir, or valacyclovir—preferably started within 72 hours of rash development.
Cool compresses, lidocaine patches.
Narcotic analgesics, tricyclic antidepressants, fabapentin, anticonvulsants, and nerve blocks for postherpetic neuralgia.
Use of corticosteroids is controversial.
Chicken pox
Chickenpox is a common childhood communicable disease caused by the varicella zoster virus. It is highly contagious and is transmitted from person to person by way of respiratory droplets. Chickenpox is usually an illness of childhood, but adults exposed to the virus for the first time may develop the disease. The varicella virus has an incubation period of 7 to 21 days and is contagious during a brief prodromal period (approximately 24 hours before lesions appear) and until all lesions are crusted over. The disease is usually self-limiting and resolves within 7 to 14 days.
Clinical Manifestations
Low-grade fever and malaise may be present 24 hours before vesicles appear.
The rash of chickenpox begins as red macules, usually first appearing on the trunk and spreading to the face and extremities. Within a few hours, the macules become fluid-filled vesicles, with more macules developing in the mouth, axilla, labia, and vagina. These latter vesicles progress to become fluid-filled. The vesicles burst after a few days and crust over.
Numerous macules, vesicles, and scabs at different stages may be present at any one time.
Mild to extreme pruritus.
Cough, coryza, and photosensitivity may accompany the lesions.
Diagnosis
Diagnosis is made by history and physical examination.
Complications
Secondary bacterial infection of the vesicles may develop.
Pneumonia, encephalitis, or joint inflammation and pain may follow chickenpox infection.
Reye syndrome may develop in children given aspirin during a chickenpox infection.
Adults who acquire chickenpox may have a particularly severe disease course and are at higher risk of developing pneumonia or other complications.
Chickenpox may spread internally in immunocompromised individuals, leading to increased morbidity and mortality.
Treatment
Prevention of chickenpox is possible with the varicella vaccine. This vaccine can be given to children or adults, and is highly successful in preventing infection. Some individuals (approximately 10%) may develop a few vesicles 10 to 20 days after immunization and may be contagious to others at that time. It is hoped that by preventing varicella, the incidence of shingles will also decline, although this has not as yet been documented.
Treatment of active chickenpox infection is mainly supportive and is geared at preventing the development of secondary skin infections. Oatmeal baths, calamine lotion, and antihistamines may be used to reduce itching. In children, the nails may be cut, or mittens may be worn, to reduce scratching.
Only gold members can continue reading. Log In or Register to continue