of connective tissue containing blood vessels, nerves, and melanocytes. The uvea is divided into three distinct anatomic segments: the choroid, which surrounds most of the eye and transits anteriorly into the ciliary body, and the iris. The most common malignant tumors of the eye, malignant melanomas, develop in the uvea, particularly in the choroid but also, less commonly, in the ciliary body and the iris. The optic nerve may be the site of formation of orbital gliomas and meningiomas. For a detailed description of the histology of the eye, the reader is referred to a simple, yet detailed and accurate account by Stevens and Lowe (1992).
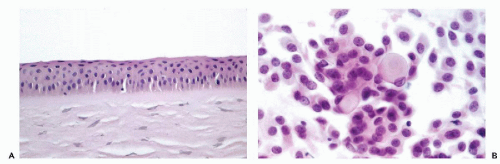 Figure 41-1 A. Normal corneal epithelium. Note orderly epithelium of squamous type without surface keratinization. B. Normal conjunctival scrape smear. Cuboidal and columnar epithelial cells and goblet cells. |
There are now several other diagnostic techniques available, such as polymerase chain reaction (PCR) for viral identification.
TABLE 41-1 CYTOLOGIC CHANGES IN VIRAL INFECTIONS OF THE EYE AND ADNEXA | |||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||
Corneal scrapings may be used for diagnosis (summary in Karayianis et al, 1988; Rivasi et al, 1995). Against a background of acute inflammation, trophozoites and the double-walled cysts of the parasite may be identified by several staining and fluorescent techniques, but also in Papanicolaou stain (Fig. 41-2). An early diagnosis and aggressive therapy are essential to prevent a loss of vision (Moore and McCulley, 1989; Rivasi et al, 1995).
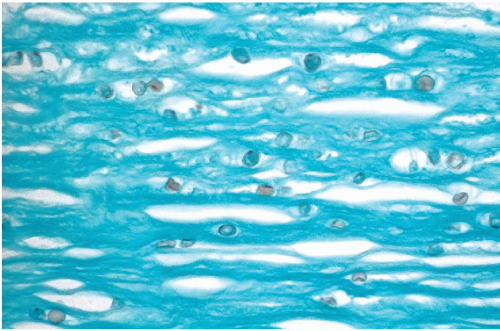 Figure 41-2 Acanthamoeba in corneal epithelium in a young wearer of contact lenses. Small spherical cysts of the parasite are stained with Gomori-methenamine silver. (Courtesy of Dr. Pearl Rosenbaum, Montefiore Medical Center, Bronx, NY.) |
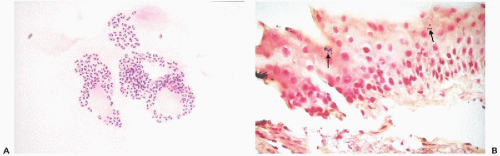 Figure 41-3 Microsporidia. A. Corneal scrapings from a 34-year-old man who was HIV-positive. The tiny organisms are present in the cytoplasm, surrounding a central clear area that is the nucleus. B. Biopsy of the limbal conjunctiva showing the Gram-positive organisms within the cytoplasm of the superficial epithelial cells. (Brown and Brenn stain.) (Courtesy of Dr. Pearl Rosenbaum, Montefiore Medical Center, Bronx, NY.) |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


