The discovery of adrenaline came about through a mistaken impression. A certain Dr. Oliver had developed a gadget which he thought measured the diameter of that artery at the wrist which is used for feeling the pulse. He measured the diameter of this artery in his son under a variety of conditions. One of the conditions involved the injection of an extract of calves’ adrenal glands. He thought he detected that this injection decreased the size of the artery. We now know that the effect of adrenaline on the diameter of a large artery would be undetectable. Dr. Oliver rushed off to let the world know of his discovery. The world, as represented by Professor Schafer, a renowned physiologist, was disbelieving. But Dr. Oliver’s enthusiasm eventually persuaded the professor to inject some of the extract into a dog whose blood pressure was being measured. To his amazement the blood pressure rose in an extraordinary fashion. Adrenaline had been discovered.
It is possible to point out many other instances where an effective discovery came at the end of a line of reasoning which was certainly not correct at every stage. It is like walking over a rocky beach. One way is to move slowly and cautiously; making sure that at each step you are firmly balanced on the rock on which you are standing before you take another step. The other way is to move swiftly over the rocks pausing so briefly on each that a precise balance at every step is no longer required. When you have got somewhere interesting, that is the time to look back and pick out the surest way of getting there again. Sometimes it is very much easier to see the surest route to a place only after you have arrived. You may have to be at the top of a mountain to find the easiest way up.
Edward de Bono, English physician and writer. From The Use of Lateral Thinking.
The best way to have a good idea is to have lots of ideas.
–Linus Pauling, Nobel Prize scientist.
SOURCES OF NEW DRUGS
What Is Meant by “Sources”?
From a company’s perspective, there are several different usages of the term sources of new drugs. They include (a) the source of the intellectual idea that led to the drug’s discovery, (b) the source of the material that is the drug, (c) the business source from which the company obtained the drug, and (d) the type of institution in which the drug was discovered.
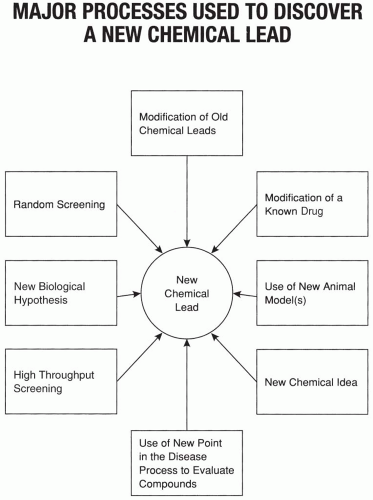
The first usage refers to the discovery of the drug. If the drug was synthesized, what was the source of the idea that led to the compound? Was it a close analogue or metabolite of a known compound, was it a prodrug (i.e., a chemical that is converted inside the body into the active drug), or did the idea come from another direction? Figure 8.1 shows a number of processes or sources used to discover a chemical with an interesting biological activity (i.e., a chemical lead). The second usage refers to whether the molecule’s origins came from a natural source (i.e., plant, mineral, or animal), whether it was artificially synthesized, or whether it was a biological product (e.g., protein).
The third group of sources refers to business sources. These include licensing arrangements, joint ventures, in-house research, purchases, or other types of business arrangements. The fourth type of source refers to the nature of the institution that developed the idea. Marketed drugs may come from pharmaceutical companies, private entrepreneurs, academicians, government laboratories, or other types of businesses. Nonetheless, approximately 90% of new drugs come from the pharmaceutical industry (Schwartzman 1976). This subject is reviewed by Kahn et al. (1982).
Figure 8.1 Major processes used to discover a new chemical lead.
Sources of Ideas for New Drugs
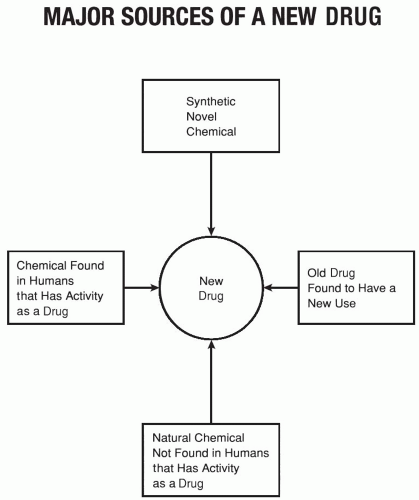
There is no limit to the intellectual sources of ideas for new drugs. Four common sources are shown in Fig. 8.2.
Adverse Events
Ideas may also result from problems (i.e., adverse events, which are sometimes referred to as adverse experiences or adverse events) with existing drugs. Adverse events for one use of a drug may serve as a new indication for the same drug. For example, a drug that is found to cause constipation as an adverse event (e.g., morphine) may be used as an active antidiarrheal. A drug that causes sedation (e.g., certain antihistamines) may be used as a sleep-promoting agent. Adverse events also stimulate companies to search for chemically related compounds that have more potent actions of the desired type. A well-known example of this situation relates to the sulfonamide antibacterial drugs. It was noticed that “sulfa” drugs lowered blood sugar and caused diuresis (excessive urination) as adverse events. Many new compounds were synthesized over many years in an attempt to exploit these adverse events. Eventually, the oral antidiabetic drugs (sulfonylureas) were discovered. Thiazide diuretics are also a descendant of many years of molecular modifications searching for a sulfonamide diuretic.
Improving on Activity
Benefits observed with some drugs have provided the impetus to companies to try to improve on this activity and develop a new therapeutic agent. In some cases, the original benefit either is a weak effect or is not observed in all patients. Therefore, there is need to improve the magnitude of the effect. For example, 6-mercaptopurine (6MP) is an antileukemic drug. It was found by Dr. Robert Schwartz at Tufts Medical Center in Boston to influence the immune response. Dr. Schwartz convinced Dr. G. Hitchings and Dr. G. Elion at the Burroughs Wellcome Company that it was important to search for other immunosuppressive compounds that might have less toxicity. They screened numerous compounds in the laboratory and found that azathioprine (Imuran) was highly active and had a much better therapeutic index in mice. During this time, Dr. Roy Calne in London read Dr. Schwartz’s paper on 6MP and tested it in dogs who had received kidney transplants. He found that the drug had some activity in preventing the body’s rejection of the kidney. He came to the United States to do a fellowship and, on his way to Boston, stopped by the laboratories of the Burroughs Wellcome Company, just outside New York City. In discussions about a better drug than 6MP, Drs. Hitchings and Elion gave Dr. Calne azathioprine to test as an immunosuppressive drug. He did. This drug had better activity than 6MP and eventually opened up the whole field of renal transplantation.
Figure 8.2 Major sources of a new drug. Genes are discussed in Chapter 12.
Data Mining
Chapter 100 shows that data mining techniques have become an established method to look for ideas of new drugs, either by searching the literature or large databases of data (e.g., genomic or proteomic data, data from high throughout screening) for novel approaches and ideas or to develop new hypotheses. These methods are expanding the possible ways in which new ideas can be generated for discovering drugs.
Computer Modeling and Simulations
Chapter 114 shows that simulations of pharmacokinetics and mechanisms of action can be used to develop ideas for improved products that can be studied both in silico and in vivo. Computer modeling can also be used to help develop and even test hypotheses for new or improved drugs.
Sources of Materials for New Drugs
Drugs Found in Natural Plants
Plants have been a source of drugs for many millennia, and some of the most important drugs still come from plants (Table 8.1). Additional information on this topic is plentiful (Balandrin et al. 1985; Steiner 1986). Nonetheless, proportionally fewer and fewer drugs are derived from plants, and the science of pharmacognosy is less frequently taught in pharmacy schools. There are some strong believers who think that there are many effective drugs in the folk drugs of China, Africa, and other societies that are unknown or underutilized in Western countries. On the other hand, a substantial number of pharmaceutical companies have screened many thousands of folk remedies (seeking active drugs) with very limited success.
Drugs Found in Animals and Humans
Drugs have been obtained from human and animal glands for several decades (e.g., insulin, vitamin B12, adrenaline, thyroid hormone, growth hormone). The advent of biotechnology brought a virtual explosion in the type and number of biologicals that are being developed as drugs (e.g., tissue plasminogen activator, interferons, various growth factors, factor 8, and numerous others). Chapter 12 has a more detailed discussion on biotechnology.
Drugs Originally Used in Animals
There are many examples where drugs used in humans were subsequently tested and eventually marketed for use in animals. There are few examples, however, of the opposite situation, where drugs used in animals were eventually used in humans. One example of this situation occurred with permethrin. Permethrin is applied as an ear tag to cattle and helps keep flies away. This is important because certain types of flies interfere with normal grazing of these animals. This drug has been found to kill lice and to treat scabies in humans.
Old Drugs Developed for New Uses
The discovery that an already marketed drug could be useful for treating a new disease is usually made in the clinic. This discovery may have been logically conceived prior to evaluation, or it may result from serendipity. A number of examples of serendipity are given in Table 8.2.
Who Discovers Drugs?
A drug’s discovery is rarely the sudden achievement of one person’s sole idea. Many people’s ideas and brainpower invariably contribute to the discovery. Sometimes there are several people who have made a major contribution. Because of human nature and many people’s desire to simplify the truth, one person usually receives credit for the discovery of a newly synthesized compound with important biological activity. This individual is often a chemist, although other people may provide intellectual input into the compound’s design. With some well-known drugs, however, other individuals (e.g., pharmacologists, research managers) have been given credit for a drug’s discovery. In some situations, this is clearly an example of power and glory going to the powerful. On the other hand, these people are often critically important as promoters of a drug. Many drugs would never reach the market if they were not pushed and promoted within a company because of the strong competition that usually exists for attention and resources.
Table 8.1Selected drugs that are prepared from natural plants
a While most of these drugs’ uses were found purely by serendipity, a few also involved hypothesis testing (e.g., allopurinol for gout, propranolol for prevention of myocardial reinfarction).
b Allopurinol was originally used in conjunction with 6MP to prevent its oxidation and, therefore, potentiate 6MP‘s anticancer effect.
When Is a Drug Discovered?
The discovery of a drug may be defined as occurring at the time when a new biological or clinical use of a compound or drug is identified. Using this broad definition, a number of important discoveries may occur for a single drug after the original discovery of its biological activity is made. Numerous processes are used to discover a drug during its life—from the initial synthesis or extraction to the end of its marketing. These processes include the following.
An idea for a new drug stimulates a chemist to synthesize a compound that is found to have the hypothesized activity and is designated as a lead compound. Alternatively, a biologically active substance may be distilled or extracted from naturally occurring products or may be produced by cells and isolated. This is an important discovery, even if it is not the discovery of the specific compound or material that eventually becomes the drug.
A biologist (e.g., pharmacologist) provides feedback of information to a chemist that leads to synthesis of a new compound that eventually becomes a drug.
Biological activity of an unanticipated type is discovered during preclinical testing. This use is eventually developed as an indication (or as the indication) for the drug.
A novel clinical activity of a drug is discovered serendipitously during investigational studies in humans. This use becomes a major, or possibly the only, use of the drug (e.g., the antihypertensive effect of propranolol was discovered during antianginal studies in humans).
A theory is tested in humans for a new use of an investigational drug and found to be correct.
Processes described in items 4 or 5 above may occur for a drug that is already marketed.
Table 8.2 lists some examples where marketed drugs were found to have new activities that became their major use.
CHOOSING THERAPEUTIC AREAS TO RESEARCH
Where Does One Look to Find a New Drug?
There is a well-known story that captures the essence of the answer to this question. An adult man was down on all fours late at night, obviously looking for something under a street lamp. Another man walked up and told the first man that he would be happy to help, but where did the man lose the object? The first man answered, “Oh, about 20 yards away.” “Then why look here?” the other asked. “Because, this is where the light is,” the first man replied.
In pharmaceutical research, companies are focusing most of their efforts in areas where the light is, not in many of the dark areas, where they believe many important drugs are. This is unfortunate, but researchers are generally limited to looking for new drugs where biological tests exist to evaluate compounds. Also, the data from those tests must be sufficiently predictive of human activity to justify spending the large sums of money necessary to develop a drug to the point where activity in humans can be assessed. In many situations, such as looking for new drugs for schizophrenia or Alzheimer’s disease, we know that we would like to look in different areas using better glasses. Another way of expressing this concept is that we would like to have better tests to aid our search for new drugs, but those improved glasses (validated animal test models) do not yet exist in many disease areas.
Description and Definitions of Therapeutic Areas
One of the most sensitive and important issues in research-based pharmaceutical companies concerns the decision of which therapeutic areas to explore in a search for new drugs. Although this issue may superficially appear to have a simple answer (e.g., those areas of greatest medical and commercial need), it is actually a complex issue at many companies, with many tensions and pressures from both within and outside the research groups. Identifying new therapeutic areas to explore is an infrequent but important decision at most companies.
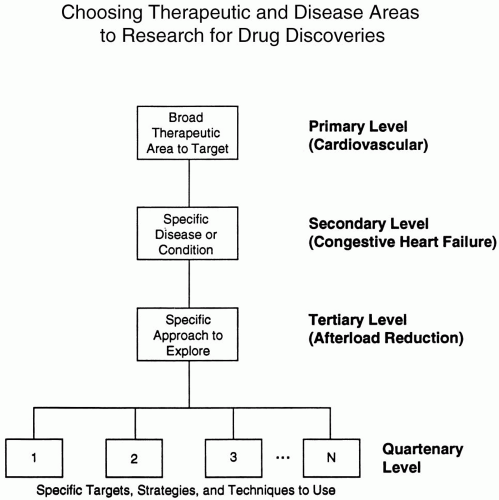
A therapeutic area is defined as a major area of disease in which drugs are presently or could potentially be used. These areas include basic specialties of internal drugs (e.g., cardiology, gastroenterology, rheumatology, nephrology) plus psychiatry, neurology, anesthesiology, and numerous other fields of drug. These categories may be viewed as a primary level. Specific diseases, syndromes, or conditions within each of those medical areas represent a secondary level of the therapeutic areas.
A tertiary level relating to therapeutic areas may be defined as the approaches and methods followed to discover new drugs within each of the secondary areas (i.e., diseases) being researched. More specifically, this tertiary level refers to the number of different places in biochemical pathways, pharmacological systems, physiological processes, and/or pathological stages of a disease that are being explored (often simultaneously) in looking for a new drug. Decisions about therapeutic areas to explore are made on at least the three different levels described. These may be summarized as (a) broad therapeutic areas, (b) specific diseases, and (c) approaches to be used. More decisions relate to the latter two levels than to the first level.
Who Has Input and Who Decides about Therapeutic Areas to Explore?
Within the research and development group, the major individuals who have input into decisions about therapeutic areas to explore (primary level) are the (a) director of research and development, (b) head of research, (c) department heads of relevant preclinical departments (e.g., organic chemistry, pharmacology, biochemistry, virology, molecular biology), and (d) senior scientists within the relevant preclinical departments. The actual decision may be made at one or more of these administrative levels and usually depends primarily on whether the proposal contains good ideas scientifically. In addition, the decision makers will usually consider company objectives, marketing goals, and the company’s comfort zone. If the decision is not made by the director of research and development, then each of the relevant individuals must usually review decisions made with those people above them in the research and development hierarchy. Depending on the training and personality of the company’s president and chief executive officer, he or she may also desire to review and approve these decisions.
Decisions on secondary areas to explore and the tertiary level of approaches are usually made at lower levels in the organization. Research scientists often propose the tertiary level approaches that they believe offer the best opportunities for discovering a new drug.
The previous discussion assumes that a company has a single site at which research to discover drugs is conducted. This is often untrue, because multinational companies usually have two or more research centers. In those instances, each site may explore and also develop different therapeutic areas, or another means of dividing their research activities may be used.
Marketing Input into Choosing Therapeutic Areas to Explore
Outside the research and development environment, there are a number of groups (primarily in marketing) that often seek to influence the areas in which research is conducted. Marketing personnel are usually primarily interested in the second level of therapeutic areas (i.e., specific diseases). Research scientists are generally aware of which medical areas have unmet therapeutic needs and usually understand whether or not there is commercial value for such potential drugs. It is often important for a company to identify therapeutic areas that it does not wish to explore.
Commercial information from marketing personnel provides valuable input to research scientists in assisting them to make decisions about the first two levels. One of the difficulties with accepting a marketing assessment of which therapeutic or disease areas to research is that a group attempting to find a drug for Disease X may uncover a drug for Disease Y or Z. Drugs for Diseases Y or Z may be much less attractive to marketing than a drug for Disease X, but the drug may have clear activity that indicates it could be marketed without undue effort. Also, the commercial value of a drug depends to a large degree on how closely its activity profile compares with that of an ideal or the best available drug for the specific disease. The answer to that question cannot be known until the drug has been in clinical trials for a number of years. A “slight” change in efficacy or safety often determines whether a drug is a large moneymaker or an “also ran” that never repays its cost of development. Finally, drugs developed for one disease are sometimes found to be useful for others. In addition to this happening for a number of common drugs, many drugs used to treat rare diseases (i.e., orphan drugs) are found in this manner.
How Many Different Therapeutic Areas Should Be Explored Simultaneously?
This question stimulates endless debate between those who wish to explore a small area intensively and those who believe that spreading research resources more thinly over a broad area increases the chances of discovering a drug. There are no simple answers to this debate.
The decision of how broadly to explore each therapeutic area being researched is usually made by the director of research and development in conjunction with the head of research. Other individuals may also be involved in this decision. The personalities, philosophies, and interests of the individuals involved will determine the decisions reached. One aspect of their philosophy would involve their general concept of research. If they have an image analogous to looking for a few diamonds lying on the surface of a large endless landscape, they might tend to deploy their staff over a broad area. If their image is analogous to looking for a diamond amidst tons of coal and rubble in a deep mine, they may choose to focus activities on a smaller number of areas to search more intensively. One of these basic approaches is usually followed at a pharmaceutical company, although it probably makes sense for most companies to use both approaches but in different therapeutic areas.
To illustrate possible approaches to the three levels of therapeutic areas, basic combinations are listed in the following text. The therapeutic areas and diseases being researched may represent any of the combinations found in Table 8.3 and in Fig. 8.3.
Table 8.3Basic approaches a company can follow in seeking to discover new drugs
Number of general therapeutic areas (primary level)
Number of diseases within each therapeutic area (secondary level)
Number of approaches used to study each disease (tertiary level)
1.
Few
Few
Few
2.
Few
Many
Few
3.
Few
Many
Many
4.
Few
Few
Many
5.
Many
Few
Few
6.
Many
Many
Few
7.
Many
Many
Many
8.
Many
Few
Many
Figure 8.3 Four levels considered in conducting research seeking to discover a new drug. Specific examples of the first three are given. Multiple or a single target, strategy, and technique may be used to explore the tertiary level. A company may explore many (or few) approaches at each level.
It is unlikely that any company’s research group approaches this issue as systematically as described here, but their philosophy will tend to lead them toward using a few of these eight general directions. The actual situation followed at many research-based pharmaceutical companies is that, within some therapeutic areas, many diseases are pursued and, within other therapeutic areas, few diseases are pursued.
What Are the Criteria to Use in Determining Which Therapeutic Areas to Explore?
There are numerous general as well as specific criteria that should be considered in determining which therapeutic areas to explore. Once these criteria are considered, the decision about each of the potential therapeutic areas to explore should be more straightforward. Broad criteria include:
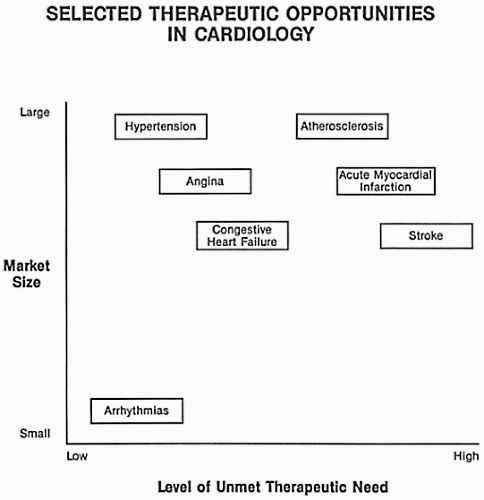
Medical value in terms of the need for new therapies in each of the areas being considered (e.g., Fig. 8.4)
Commercial value of each market area in terms of both present and anticipated future size
Skills of the scientific staff presently employed and those available to be hired or consulted
Interests of the scientific staff and managers
Other drugs (both marketed and investigational) in the area from the same company
Availability of suitable animal models to predict efficacy in humans
Company traditions in emphasizing certain therapeutic areas
A more specific criterion (which may trump several of the more general criteria) is the presence of worthwhile chemical leads or novel scientific ideas for developing drugs.
Choosing the Number of New Compounds of One Type to Develop
There may be sound medical reasons (e.g., greater convenience and compliance, improved tolerance, efficacy for patients not helped by others) to develop several drugs of one therapeutic or chemical class such as beta-blockers or nonsteroidal anti-inflammatory drugs. But, after ten or so drugs of the same type are marketed, it is difficult to justify the development of additional ones. Some research and marketing directors believe that most markets can only support two to four drugs of any one type. Incentives to develop additional drugs of the same type generally decrease as regulatory agencies become more resistant to approving newer versions where many similar drugs exist. This trend is already occurring in North America where many nonsteroidal anti-inflammatory drugs, beta-receptor antagonists, and other examples exist. Another factor that will diminish the development of an excessive number of “me-too” drugs is the fact that hospitals, Health Maintenance Organizations (HMOs), provinces with national health, and other medical provider organizations that have formularies are becoming resistant to including new drugs that have no demonstrated benefits over existing therapy. Such benefits may, however, be defined in terms of quality of life, cost effectiveness, compliance, and other categories in addition to efficacy and safety.
Figure 8.4 Selected therapeutic opportunities in cardiology for new drug development.
Competition of Drug Discovery Ideas for Resources
Within most drug discovery groups of research-based pharmaceutical companies, hundreds if not thousands of novel ideas surface each year. Many of these require resources in terms of staff effort and time to evaluate their feasibility or quality. Because of commitments to ongoing projects, only a small number of these ideas can be adequately evaluated. One critical question is: Which ideas are evaluated and to what degree? In an ideal situation, ideas with the greatest scientific merit would be the ones evaluated. But, in this imperfect world, there are two other major factors that influence the decision.
First, it is often impossible to determine the true scientific value of an idea until after the idea is actually tested. Some of the most outlandish ideas are found to be correct after the experiments have been done, and other ideas that seem both true and valuable are shown to be false. Therefore, there is a degree of guesswork at an early stage in ranking ideas according to their ultimate value. In fact, it is shortly prior to submitting a New Drug Application that the clinical profiles of most new products are known for the first time.
Second, there is the issue of company politics. Everyone knows (or should know) that the value of an idea equals its intrinsic value times the position of the idea’s proponent to the third power. Therefore, if someone wants to have an idea receive a more sympathetic hearing from management, that person might wish to seek a superior in the company to sponsor the idea. Alternatively, the innovator might turn the idea over to a superior in the hope that that would enhance its chance of being approved for evaluation. If a committee is to evaluate the idea, it might be advisable for the idea’s proponent to meet each of the members in advance to review and lobby for the idea before it is actually proposed. Many ideas are turned down because they were never properly understood by the group that discussed them. This situation could often be avoided by having the idea’s sponsor conduct preliminary discussions with committee members. This is especially important when the idea’s sponsor is not present at the major meeting where the idea’s ultimate fate is determined.
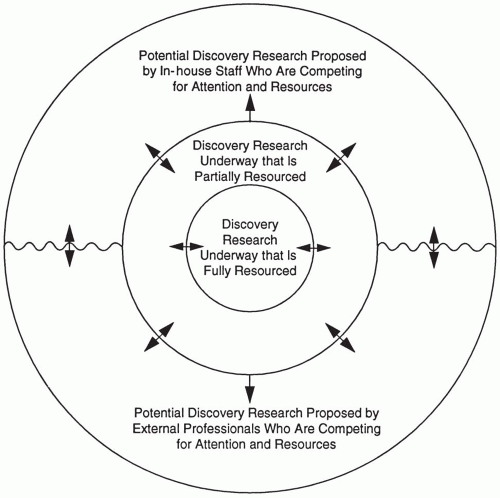
Pertinent questions for a company to assess are whether the best ideas are being proposed or being suppressed. Do scientists believe their ideas are being given a fair hearing? Also, is there a formal system to air new ideas of drug discovery? For example, a written document could be presented every month or half year in which new ideas could be presented. In addition, a scientific forum could be held periodically where ideas would be presented and critiqued. Ultimately, ideas that require major resources must be evaluated by senior research managers, and those that require little time or resources may be reviewed by scientists who would perform the experiments. Figure 8.5 illustrates some of these issues.
A few other suggestions for scientists or others who wish to have their research (or other) ideas adopted are to (a) attempt to integrate the proposed idea into existing work or into an existing group within the company (as opposed to proposing that a totally new group or department be formed), (b) identify each of the steps that will be necessary to implement the idea, (c) plan and describe each of those steps in a logical sequence, (d) initiate the process described in the proposal but do not rush any of the individual steps, (e) show how others will benefit from the proposal, (f) include a clear rationale in the proposal, (g) conduct a few preliminary tests to demonstrate the likely value of the concept, (h) buttress the concept with published information, and (i) include other scientists in the proposal (possibly from an academic or other institution).
Initiating Activities in a New Therapeutic Area of Research
After a decision is reached to conduct research in a new therapeutic area (primary level), it may be straightforward to reassign scientists to the new therapeutic area within their own discipline (e.g., biochemistry). If the new area of research requires staff with the same general skills and knowledge, then reassigning personnel is usually possible. The ability to reassign people successfully to a new therapeutic area depends on the individuals, their interests, and how well their knowledge and experience enable them to make the transition. If a totally new therapeutic area is to be explored, then many scientists would balk at being reassigned from an area in which they are trained, experienced, and building their careers. This is generally the case for pharmacologists and physiologists who are asked to take on totally new types of methodologies and approaches. On the other hand, many biochemists and chemists would not have to alter their technical skills and approaches in switching their efforts from one therapeutic field to another, and it is much easier to make a major switch to a new therapeutic area in those disciplines.
Because of limitations in moving personnel in many biological sciences, it is often necessary to hire a number of new scientific staff when a decision is made to enter a new therapeutic area. When a relatively large group of five or more professional staff is needed within a single discipline, it is usually desirable to hire initially a single experienced individual to head the group. That person is then given the task of hiring the additional staff needed. This approach helps assure that the group assembled will work well together and have skills that are appropriate to deal with their newly assigned tasks.
Should Pharmaceutical Companies Be Engaged in Basic Research?
Many scientists talk about basic and applied research as if they were easily separated categories. The fact is that many definitions are used for each term, and sometimes there is a great deal of overlap between the two terms. Numerous scientists deny that any meaningful distinction can be made. For example, Bartholini (1983) wrote that “basic and applied research, by my approach, are unified; the same investigator has to screen—which is a fundamental part of pharmacological research—and has to investigate biological mechanisms.” The mechanisms referred to are usually considered as part of basic research, and screening is considered as applied research. Nonetheless, these views depend on to whom one speaks. The author believes there are different types of research conducted within a pharmaceutical company and that they may be visualized as a spectrum that includes both basic and applied research. One such spectrum is shown in Fig. 8.15. Toward the basic research end of the spectrum, the connection to drug discovery or development becomes progressively weaker. Research-based pharmaceutical companies must be engaged in both basic and applied types of research. One major issue is to decide how much of each activity should be conducted, although certain research has both applied and basic characteristics.
Figure 8.5 The competition for resources in discovery activities. Activities closest to the center are best financed and intellectually supported, and those at the perimeter are least supported.
Some people use the term basic research to apply to speculative, fundamental, nondirected, nontargeted, or exploratory research that is curiosity-driven and without any clearly identifiable usefulness. This type of research is most often conducted in academic institutions. Using this definition, many research-based pharmaceutical companies desire to conduct a limited amount of basic research or to avoid it altogether. This is often justified by the belief that this type of work is usually distant from drug discovery. It is accepted that basic research has the potential for leading to a major breakthrough in scientific understanding, which may be able to be converted into (a) a new animal test model, (b) a new chemical series, or (c) a new approach to discovering drugs. One of these three tools may eventually, in turn, lead to discovery of a breakthrough drug. For example, if a little-studied or previously unknown enzyme is found to be important for a specific disease (i.e., a scientific breakthrough), then animal tests can be established to look for compounds that act as inhibitors, stimulators, or mimics of the enzyme. If an active lead compound is found, it would encourage chemists to make many analogues.
Only gold members can continue reading. Log In or Register to continue