Chapter 20 The Bedside Diagnosis of Coma
-René Theophyle Yacinthe Laennec, 1810; letter to his cousin Cristophe
“His was a great sin who first invented consciousness. Let us lose it for a few hours.”
-John, in The Diamond as Big as the Ritz, by F. Scott Fitzgerald—uttered before falling asleep
Generalities
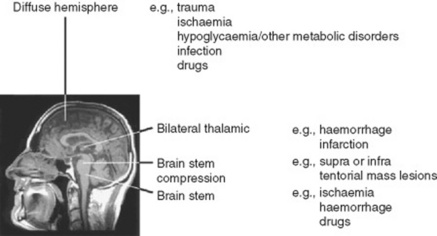
15 So what are the causes of coma?
 Diffuse or extensive processes affecting the whole brain (but primarily the cortex)
Diffuse or extensive processes affecting the whole brain (but primarily the cortex)

 Supratentorial mass lesions causing transtentorial herniation with brain stem compression (these are often associated with other neurologic signs, such as third nerve palsy and crossed hemiparesis) (see Fig. 20-1)
Supratentorial mass lesions causing transtentorial herniation with brain stem compression (these are often associated with other neurologic signs, such as third nerve palsy and crossed hemiparesis) (see Fig. 20-1)

16 What is the function of the neurologic exam in comatose patients?



17 What is the neurologic exam of a comatose patient?
A simple one. Since the cortex of coma is, by definition, dysfunctional, exam is only aimed at assessing brain stem function. This is carried out in a rostral-caudal and level-by-level fashion. If all four layers of the brain stem are working properly, then the coma is cortical (i.e., one in which the cortex is primarily dysfunctional). If one or more brain stem layer is damaged, then the coma is a brain stem coma (i.e., one in which the cortex is secondarily dysfunctional as a result of direct brain stem damage) (see Table 20-1).
Table 20-1 Clinical Assessment of Coma
| General Examination |
 Skin (e.g., rash, anemia, cyanosis, jaundice) Skin (e.g., rash, anemia, cyanosis, jaundice) |
 Temperature (fever-infection, hypothermia-drugs, circulatory failure) Temperature (fever-infection, hypothermia-drugs, circulatory failure) |
 Blood pressure (e.g., septicemia, Addison’s disease) Blood pressure (e.g., septicemia, Addison’s disease) |
 Breath (e.g., fetor hepaticus) Breath (e.g., fetor hepaticus) |
 Cardiovascular (e.g., arrhythmias) Cardiovascular (e.g., arrhythmias) |
 Abdomen (e.g., organomegaly) Abdomen (e.g., organomegaly) |
| Neurologic Examination |
 Head, neck, and eardrum (trauma) Head, neck, and eardrum (trauma) |
 Meningism (subarachnoid hemorrhage, meningitis) Meningism (subarachnoid hemorrhage, meningitis) |
 Funduscopy Funduscopy |
| Level of Consciousness |
 Glasgow Coma Scale (verbal response, eye opening, motor response) Glasgow Coma Scale (verbal response, eye opening, motor response) |
| Brain Stem Function |
 Pupillary responses Pupillary responses |
 Spontaneous eye movements Spontaneous eye movements |
 Oculocephalic responses Oculocephalic responses |
 Caloric responses Caloric responses |
 Corneal responses Corneal responses |
| Motor Function |
 Motor response Motor response |
 Deep tendon reflexes Deep tendon reflexes |
 Muscle tone Muscle tone |
 Plantars Plantars |
| Respiratory Pattern |
 Cheyne-Stokes: hemisphere Cheyne-Stokes: hemisphere |
 Central neurogenic hyperventilation: rapid/midbrain Central neurogenic hyperventilation: rapid/midbrain |
 Apneustic: rapid with pauses/lower pontine Apneustic: rapid with pauses/lower pontine |
(Adapted from Bateman DE. Neurological assessment of coma. J Neurol Neurosurg Psychiatry 71[Suppl 1]: i13–i17, 2001.)
19 What is the first step in evaluating coma?
To assess whether there is any response to verbal stimuli. This can be done by asking patients to open their eyes and look up, down, and from side to side. “Locked-in” patients (see question 54) will open their eyes on command, and even look up and down, but will be unable to make any other purposeful response. Once this is done, the next step in the evaluation of coma is to test the first and uppermost brain stem level: the thalamus.
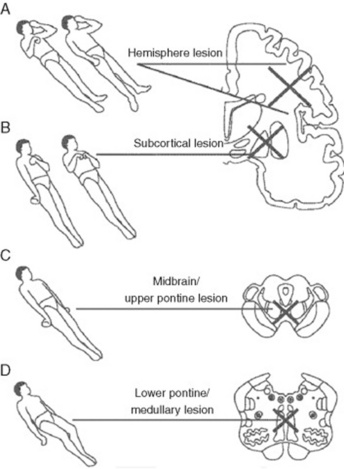
22 What are these postures?
Valuable findings for localization. A decorticate posture is a sign of subcortical/thalamic dysfunction. It consists of upper extremities’ flexion, with extension and internal rotation of lower extremities. A decerebrate posture consists instead of extension and internal rotation of both upper and lower extremities. This is a sign of upper brain stem dysfunction, usually the consequence of midbrain or upper pontine lesions. Finally, lower brain stem damage (low pontine and medullary) will cause no response to painful stimuli, or just extension of the upper extremities with simple bending of the knees (a spinal reflex). Unilateral decerebrate or decorticate responses also may occur, usually indicating unilateral lesions. Overall, it is easy to separate decortication from decerebration by remembering that in de-cor-tication the hand points toward the heart (cor), whereas in decerebration the hand points away from the heart (see Fig. 20-2).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


