EMERGENCY INTERVENTIONS
After detecting tachycardia, take the patient’s other vital signs and determine his level of consciousness (LOC). If the patient has increased or decreased blood pressure and is drowsy or confused, administer oxygen and begin cardiac monitoring. Perform electrocardiography (ECG) to examine for reduced cardiac output, which may initiate or result from tachycardia. Insert an I.V. line for fluid, blood product, and drug administration, and gather emergency resuscitation equipment.
History and Physical Examination
If the patient’s condition permits, take a focused history. Find out if he has had palpitations. If so, how were they treated? Explore associated symptoms. Is the patient dizzy or short of breath? Is he weak or fatigued? Is he experiencing episodes of syncope or chest pain? Next, ask about a history of trauma, diabetes, or cardiac, pulmonary, or thyroid disorders. Also, obtain an alcohol and drug history, including prescription, over-the-counter, and illicit drugs.
Inspect the patient’s skin for pallor or cyanosis. Assess pulses, noting peripheral edema. Finally, auscultate the heart and lungs for abnormal sounds or rhythms.
Medical Causes
- Acute respiratory distress syndrome (ARDS). Besides tachycardia, ARDS causes crackles, rhonchi, dyspnea, tachypnea, nasal flaring, and grunting respirations. Other findings include cyanosis, anxiety, decreased LOC, and abnormal chest X-ray findings.
- Adrenocortical insufficiency. With adrenocortical insufficiency, tachycardia commonly occurs with a weak pulse as well as progressive weakness and fatigue, which may become so severe that the patient requires bed rest. Other signs and symptoms include abdominal pain, nausea and vomiting, altered bowel habits, weight loss, orthostatic hypotension, irritability, bronze skin, decreased libido, and syncope. Some patients report an enhanced sense of taste, smell, and hearing.
What Happens in Tachycardia
Tachycardia represents the heart’s effort to deliver more oxygen to body tissues by increasing the rate at which blood passes through the vessels. This sign can reflect overstimulation within the sinoatrial node, the atrium, the atrioventricular node, or the ventricles.
Because heart rate affects cardiac output (cardiac output = heart rate × stroke volume), tachycardia can lower cardiac output by reducing ventricular filling time and stroke volume (the output of each ventricle at every contraction). As cardiac output plummets, arterial pressure and peripheral perfusion decrease. Tachycardia further aggravates myocardial ischemia by increasing the heart’s demand for oxygen while reducing the duration of diastole — the period of greatest coronary flow.
- Anaphylactic shock. With life-threatening anaphylactic shock, tachycardia and hypotension develop within minutes after exposure to an allergen, such as penicillin or an insect sting. Typically, the patient is visibly anxious and has severe pruritus, perhaps with urticaria and a pounding headache. Other findings may include flushed and clammy skin, a cough, dyspnea, nausea, abdominal cramps, seizures, stridor, change or loss of voice associated with laryngeal edema, and urinary urgency and incontinence.
- Anemia. Tachycardia and bounding pulse are characteristic with anemia. Associated signs and symptoms include fatigue, pallor, dyspnea, and, possibly, bleeding tendencies. Auscultation may reveal an atrial gallop, a systolic bruit over the carotid arteries, and crackles.
- Aortic insufficiency. Accompanying tachycardia with aortic insufficiency are a “water-hammer” bounding pulse and a large, diffuse apical heave. With severe insufficiency, widened pulse pressure occurs. Auscultation reveals a hallmark diastolic murmur that starts with the second heart sound; is decrescendo, high-pitched, and blowing; and is heard best at the left sternal border of the second and third intercostal spaces. An atrial or ventricular gallop, an early systolic murmur, an Austin Flint murmur (apical diastolic rumble), or Duroziez’s sign (a murmur over the femoral artery during systole and diastole) may also be heard. Other findings include angina, dyspnea, palpitations, strong and abrupt carotid pulsations, pallor, and signs of heart failure, such as crackles and jugular vein distention.
- Aortic stenosis. Typically, aortic stenosis — a valvular disorder — causes tachycardia, a weak, thready pulse, and an atrial gallop. Its chief features, however, are exertional dyspnea, angina, dizziness, and syncope. Aortic stenosis also causes a harsh, crescendo-decrescendo systolic ejection murmur that’s loudest at the right sternal border of the second intercostal space. Other findings include palpitations, crackles, and fatigue.
- Cardiac arrhythmias. Tachycardia may occur with an irregular heart rhythm. The patient may be hypotensive and report dizziness, palpitations, weakness, and fatigue. Depending on his heart rate, he may also exhibit tachypnea, decreased LOC, and pale, cool, clammy skin.
- Cardiac contusion. The result of blunt chest trauma, cardiac contusion may cause tachycardia, substernal pain, dyspnea, and palpitations. Assessment may detect sternal ecchymoses and a pericardial friction rub.
- Cardiac tamponade. With life-threatening cardiac tamponade, tachycardia is commonly accompanied by paradoxical pulse, dyspnea, and tachypnea. The patient is visibly anxious and restless and has cyanotic, clammy skin and distended jugular veins. He may develop muffled heart sounds, pericardial friction rub, chest pain, hypotension, narrowed pulse pressure, and hepatomegaly.
- Cardiogenic shock. Although many features of cardiogenic shock appear in other types of shock, they’re usually more profound in this type. Accompanying tachycardia are weak, thready pulse; narrowing pulse pressure; hypotension; tachypnea; cold, pale, clammy, and cyanotic skin; oliguria; restlessness; and altered LOC.
- Cholera. Signs of cholera include abrupt watery diarrhea and vomiting. Severe fluid and electrolyte loss leads to tachycardia, thirst, weakness, muscle cramps, decreased skin turgor, oliguria, and hypotension. Without treatment, death can occur within hours.
- Chronic obstructive pulmonary disease (COPD). Although the clinical picture varies widely with COPD, tachycardia is a common sign. Other characteristic findings include cough, tachypnea, dyspnea, pursed-lip breathing, accessory muscle use, cyanosis, diminished breath sounds, rhonchi, crackles, and wheezing. Clubbing and barrel chest are usually late findings.
- Diabetic ketoacidosis. Life-threatening diabetic ketoacidosis commonly produces tachycardia and a thready pulse. Its cardinal sign, however, is Kussmaul’s respirations — abnormally rapid, deep breathing. Other signs and symptoms of acidosis include fruity breath odor, orthostatic hypotension, generalized weakness, anorexia, nausea, vomiting, and abdominal pain. The patient’s LOC may vary from lethargy to coma.
- Heart failure. Especially common with left-sided heart failure, tachycardia may be accompanied by a ventricular gallop, fatigue, dyspnea (exertional and paroxysmal nocturnal), orthopnea, and leg edema. Eventually, the patient develops widespread signs and symptoms, such as palpitations, narrowed pulse pressure, hypotension, tachypnea, crackles, dependent edema, weight gain, slowed mental response, diaphoresis, pallor, and, possibly, oliguria. Late signs include hemoptysis, cyanosis, and marked hepatomegaly and pitting edema.
- Hyperosmolar hyperglycemic nonketotic syndrome. A rapidly deteriorating LOC is commonly accompanied by tachycardia, hypotension, tachypnea, seizures, oliguria, and severe dehydration with poor skin turgor and dry mucous membranes.
- Hypertensive crisis. Life-threatening hypertensive crisis is characterized by tachycardia, tachypnea, diastolic blood pressure that exceeds 120 mm Hg, and systolic blood pressure that may exceed 200 mm Hg. Typically, the patient develops pulmonary edema with jugular vein distention, dyspnea, and pink, frothy sputum. Related findings include chest pain, severe headache, drowsiness, confusion, anxiety, tinnitus, epistaxis, muscle twitching, seizures, nausea, and vomiting. Focal neurologic signs, such as paresthesia, may also occur.
- Hypoglycemia. A common sign of hypoglycemia, tachycardia accompanies hypothermia, nervousness, trembling, fatigue, malaise, weakness, headache, hunger, nausea, diaphoresis, and moist, clammy skin. Central nervous system effects include blurred or double vision, motor weakness, hemiplegia, seizures, and decreased LOC.
- Hypovolemia. Tachycardia may occur with hypovolemia. Associated findings include hypotension, decreased skin turgor, sunken eyeballs, thirst, syncope, and dry skin and tongue.
- Hypovolemic shock. Mild tachycardia, an early sign of life-threatening hypovolemic shock, may be accompanied by tachypnea, restlessness, thirst, and pale, cool skin. As shock progresses, the patient’s skin becomes clammy and his pulse becomes increasingly rapid and thready. He may also develop hypotension, narrowed pulse pressure, oliguria, subnormal body temperature, and decreased LOC.
- Neurogenic shock. Tachycardia or bradycardia may accompany tachypnea, apprehension, oliguria, variable body temperature, decreased LOC, and warm, dry skin.
- Orthostatic hypotension. Tachycardia accompanies the characteristic signs and symptoms of orthostatic hypotension, which include dizziness, syncope, pallor, blurred vision, diaphoresis, and nausea.
- Pneumothorax. Life-threatening pneumothorax causes tachycardia and other signs and symptoms of distress, such as severe dyspnea and chest pain, tachypnea, and cyanosis. Related findings include dry cough, subcutaneous crepitation, absent or decreased breath sounds, cessation of normal chest movement on the affected side, and decreased vocal fremitus.
- Pulmonary embolism. With pulmonary embolism, tachycardia is usually preceded by sudden dyspnea, angina, or pleuritic chest pain. Common associated signs and symptoms include weak peripheral pulses, cyanosis, tachypnea, low-grade fever, restlessness, diaphoresis, and a dry cough or a cough with blood-tinged sputum.
- Thyrotoxicosis. Tachycardia is a classic feature of thyrotoxicosis — a thyroid disorder. Others include an enlarged thyroid, nervousness, heat intolerance, weight loss despite increased appetite, diaphoresis, diarrhea, tremors, and palpitations. Although also considered characteristic, exophthalmos is sometimes absent.
Because thyrotoxicosis affects virtually every body system, its associated features are diverse and numerous. Some examples include full and bounding pulse, widened pulse pressure, dyspnea, anorexia, nausea, vomiting, altered bowel habits, hepatomegaly, and muscle weakness, fatigue, and atrophy. The patient’s skin is smooth, warm, and flushed; his hair is fine and soft and may gray prematurely or fall out. The female patient may have a reduced libido and oligomenorrhea or amenorrhea; the male patient may exhibit a reduced libido and gynecomastia.
Other Causes
- Diagnostic tests. Cardiac catheterization and electrophysiologic studies may induce transient tachycardia.
- Drugs and alcohol. Various drugs affect the nervous system, circulatory system, or heart muscle, resulting in tachycardia. Examples of these include sympathomimetics; phenothiazines; anticholinergics, such as atropine; thyroid drugs; vasodilators, such as hydralazine; acetylcholinesterase inhibitors, such as captopril; nitrates, such as nitroglycerin; alpha-adrenergic blockers, such as phentolamine; and beta-adrenergic bronchodilators, such as albuterol. Excessive caffeine intake and alcohol intoxication may also cause tachycardia.
- Surgery and pacemakers. Cardiac surgery and pacemaker malfunction or wire irritation may cause tachycardia.
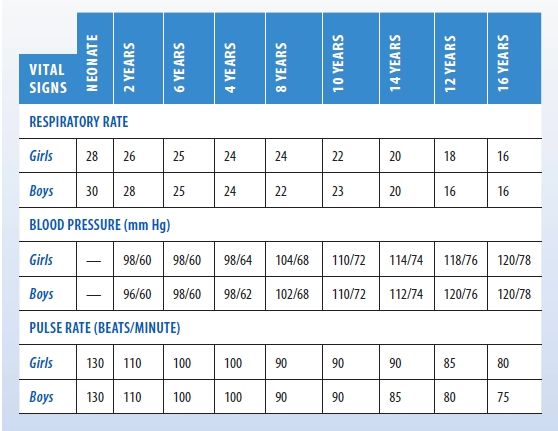
Normal Pediatric Vital Signs
This chart lists the normal resting respiratory rate, blood pressure, and pulse rate for girls and boys to age 16.
Special Considerations
Continue to monitor the patient closely. Explain ordered diagnostic tests, such as a thyroid panel, electrolyte and hemoglobin levels, hematocrit, pulmonary function studies, and 12-lead ECG. If appropriate, prepare him for an ambulatory ECG.
Educate the patient about the possibility of the tachyarrhythmia recurring. Explain that an antiarrhythmic and an internal defibrillator or ablation therapy may be indicated for symptomatic tachycardia.
Patient Counseling
Explain the possibility of tachyarrhythmia recurring. Instruct the patient about the use of antiarrhythmics, an internal defibrillator, or ablation therapy, as appropriate.
Pediatric Pointers
When examining a child for tachycardia, recognize that normal heart rates for children are higher than those for adults. (See Normal Pediatric Vital Signs.) In children, tachycardia may result from many of the adult causes described above.
REFERENCES
Berkowitz, C. D. (2012). Berkowitz’s pediatrics: A primary care approach (4th ed.). USA: American Academy of Pediatrics.
Buttaro, T. M., Tybulski, J., Bailey, P. P., & Sandberg-Cook, J. (2008). Primary care: A collaborative practice (pp. 444–447). St. Louis, MO: Mosby Elsevier.
Colyar, M. R. (2003). Well-child assessment for primary care providers. Philadelphia, PA: F.A. Davis.
Lehne, R. A. (2010). Pharmacology for nursing care (7th ed.). St. Louis, MO: Saunders Elsevier.
McCance, K. L., Huether, S. E., Brashers, V. L., & Rote, N. S. (2010). Pathophysiology: The biologic basis for disease in adults and children. Maryland Heights, MO: Mosby Elsevier.
Sommers, M. S., & Brunner, L. S. (2012). Pocket diseases. Philadelphia, PA: F.A. Davis.
Tachypnea
A common sign of cardiopulmonary disorders, tachypnea is an abnormally fast respiratory rate — 20 or more breaths/minute. Tachypnea may reflect the need to increase minute volume — the amount of air breathed each minute. Under these circumstances, it may be accompanied by an increase in tidal volume — the volume of air inhaled or exhaled per breath — resulting in hyperventilation. Tachypnea, however, may also reflect stiff lungs or overloaded ventilatory muscles, in which case tidal volume may actually be reduced.
Tachypnea may result from reduced arterial oxygen tension or arterial oxygen content, decreased perfusion, or increased oxygen demand. Heightened oxygen demand, for example, may result from fever, exertion, anxiety, and pain. It may also occur as a compensatory response to metabolic acidosis or may result from pulmonary irritation, stretch receptor stimulation, or a neurologic disorder that upsets medullary respiratory control. Generally, respirations increase by 4 breaths/minute for every 1°F (17.2°C) increase in body temperature.
Emergency Interventions
After detecting tachypnea, quickly evaluate cardiopulmonary status; obtain a set of vital signs with oxygen saturation; and check for cyanosis, chest pain, dyspnea, tachycardia, and hypotension. If the patient has paradoxical chest movement, suspect flail chest and immediately splint his chest with your hands or with sandbags. Then administer supplemental oxygen by nasal cannula or face mask and, if possible, place the patient in semi-Fowler’s position to help ease his breathing. Intubation and mechanical ventilation may be necessary if respiratory failure occurs. Also, insert an I.V. line for fluid and drug administration and begin cardiac monitoring.
History and Physical Examination
If the patient’s condition permits, obtain a medical history. Find out when the tachypnea began. Did it follow activity? Has he had it before? Does the patient have a history of asthma, chronic obstructive pulmonary disease (COPD), or any other pulmonary or cardiac conditions? Then have him describe associated signs and symptoms, such as diaphoresis, chest pain, and recent weight loss. Is he anxious about anything, or does he have a history of anxiety attacks? Note whether he takes any drugs for pain relief. If so, how effective are they?
Begin the physical examination by taking the patient’s vital signs, including oxygen saturation, if you haven’t already done so, and observing his overall behavior. Does he seem restless, confused, or fatigued? Then auscultate the chest for abnormal heart and breath sounds. If the patient has a productive cough, record the color, amount, and consistency of sputum. Finally, check for jugular vein distention, and examine the skin for pallor, cyanosis, edema, and warmth or coolness.
Medical Causes
- Acute respiratory distress syndrome (ARDS). With life-threatening ARDS, tachypnea and apprehension may be the earliest features. Tachypnea gradually worsens as fluid accumulates in the patient’s lungs, causing them to stiffen. It’s accompanied by accessory muscle use, grunting expirations, suprasternal and intercostal retractions, crackles, and rhonchi. Eventually, ARDS produces hypoxemia, resulting in tachycardia, dyspnea, cyanosis, respiratory failure, and shock.
- Anaphylactic shock. With anaphylactic shock — a life-threatening type of shock — tachypnea develops within minutes after exposure to an allergen, such as penicillin or insect venom. Accompanying signs and symptoms include anxiety, pounding headache, skin flushing, intense pruritus, and, possibly, diffuse urticaria. The patient may exhibit widespread edema, affecting the eyelids, lips, tongue, hands, feet, and genitalia. Other findings include cool, clammy skin; rapid, thready pulse; cough; dyspnea; stridor; and change or loss of voice associated with laryngeal edema.
- Aspiration of a foreign body. Life-threatening upper airway obstruction may result from aspiration of a foreign body. With a partial obstruction, the patient abruptly develops a dry, paroxysmal cough with rapid, shallow respirations. Other signs and symptoms include dyspnea, gagging or choking, intercostal retractions, nasal flaring, cyanosis, decreased or absent breath sounds, hoarseness, and stridor or coarse wheezing. Typically, the patient appears frightened and distressed. A complete obstruction may rapidly cause asphyxia and death.
- Asthma. Tachypnea is common with life-threatening asthma attacks, which commonly occur at night. These attacks usually begin with mild wheezing and a dry cough that progresses to mucus expectoration. Eventually, the patient becomes apprehensive and develops prolonged expirations, intercostal and supraclavicular retractions on inspiration, accessory muscle use, severe audible wheezing, rhonchi, flaring nostrils, tachycardia, diaphoresis, and flushing or cyanosis.
- Bronchitis (chronic). Mild tachypnea may occur in chronic bronchitis (a form of COPD), but it isn’t typically a predominant sign. Usually, chronic bronchitis begins with a dry, hacking cough, which later produces copious amounts of sputum. Other characteristics include dyspnea, prolonged expirations, wheezing, scattered rhonchi, accessory muscle use, and cyanosis. Clubbing and barrel chest are late signs.
- Cardiac arrhythmias. Depending on the patient’s heart rate, tachypnea may occur along with hypotension, dizziness, palpitations, weakness, and fatigue. The patient’s level of consciousness (LOC) may be decreased.
- Cardiac tamponade. With life-threatening cardiac tamponade, tachypnea may accompany tachycardia, dyspnea, and paradoxical pulse. Related findings include muffled heart sounds, pericardial friction rub, chest pain, hypotension, narrowed pulse pressure, and hepatomegaly. The patient is noticeably anxious and restless. His skin is clammy and cyanotic, and his jugular veins are distended.
- Cardiogenic shock. Although many signs of cardiogenic shock appear in other types of shock, they’re usually more severe in this type. Besides tachypnea, the patient commonly displays cool, pale, clammy, cyanotic skin; hypotension; tachycardia; narrowed pulse pressure; a ventricular gallop; oliguria; decreased LOC; and jugular vein distention.
- Emphysema. Emphysema — a chronic pulmonary disorder — commonly produces tachypnea accompanied by exertional dyspnea. It may also cause anorexia, malaise, peripheral cyanosis, pursed-lip breathing, accessory muscle use, and chronic productive cough. Percussion yields a hyperresonant tone; auscultation reveals wheezing, crackles, and diminished breath sounds. Clubbing and barrel chest are late signs.
- Flail chest. Tachypnea usually appears early in life-threatening flail chest. Other findings include paradoxical chest wall movement, rib bruises and palpable fractures, localized chest pain, hypotension, and diminished breath sounds. The patient may also develop signs of respiratory distress, such as dyspnea and accessory muscle use.
- Hyperosmolar hyperglycemic nonketotic syndrome. Rapidly deteriorating LOC occurs with tachypnea, tachycardia, hypotension, seizures, oliguria, and signs of dehydration.
- Hypovolemic shock. An early sign of life-threatening hypovolemic shock, tachypnea is accompanied by cool, pale skin; restlessness; thirst; and mild tachycardia. As shock progresses, the patient’s skin becomes clammy; his pulse is increasingly rapid and thready. Other findings include hypotension, narrowed pulse pressure, oliguria, subnormal body temperature, and decreased LOC.
- Hypoxia. Lack of oxygen from any cause increases the rate (and commonly the depth) of breathing. Associated symptoms are related to the cause of the hypoxia.
- Interstitial fibrosis. With interstitial fibrosis, tachypnea develops gradually and may become severe. Associated features include exertional dyspnea, pleuritic chest pain, a paroxysmal dry cough, crackles, late inspiratory wheezing, cyanosis, fatigue, and weight loss. Clubbing is a late sign.
- Lung abscess. With lung abscess, tachypnea is usually paired with dyspnea and accentuated by fever. However, the chief sign is a productive cough with copious amounts of purulent, foul-smelling, usually bloody sputum. Other findings include chest pain, halitosis, diaphoresis, chills, fatigue, weakness, anorexia, weight loss, and clubbing.
- Mesothelioma (malignant). Commonly related to asbestos exposure, this pleural mass initially produces tachypnea and dyspnea on mild exertion. Other classic symptoms are persistent, dull chest pain and aching shoulder pain that progresses to arm weakness and paresthesia. Later signs and symptoms include a cough, insomnia associated with pain, clubbing, and dullness over the malignant mesothelioma.
- Neurogenic shock. Tachypnea is characteristic in neurogenic shock — a life-threatening type of shock. It’s commonly accompanied by apprehension, bradycardia or tachycardia, oliguria, fluctuating body temperature, and decreased LOC that may progress to coma. The patient’s skin is warm, dry, and perhaps flushed. He may experience nausea and vomiting.
- Plague (Yersinia pestis). The onset of the pneumonic form of plague is usually sudden with chills, fever, headache, and myalgias. Pulmonary signs and symptoms include tachypnea, productive cough, chest pain, dyspnea, hemoptysis, and increasing respiratory distress and cardiopulmonary insufficiency. The pneumonic form may be contracted from person-to-person direct contact via the respiratory system. This would also be the form contracted in biological warfare from aerosolization and inhalation of the organism.
- Pneumonia (bacterial). A common sign of pneumonia, tachypnea is usually preceded by a painful, hacking, dry cough that rapidly becomes productive. Other signs and symptoms quickly follow, including high fever, shaking chills, headache, dyspnea, pleuritic chest pain, tachycardia, grunting respirations, nasal flaring, and cyanosis. Auscultation reveals diminished breath sounds and fine crackles; percussion yields a dull tone.
- Pneumothorax. Tachypnea, a common sign of life-threatening pneumothorax, is typically accompanied by severe, sharp, and commonly unilateral chest pain that’s aggravated by chest movement. Associated signs and symptoms include dyspnea, tachycardia, accessory muscle use, asymmetrical chest expansion, dry cough, cyanosis, anxiety, and restlessness. Examination of the affected lung reveals hyperresonance or tympany, subcutaneous crepitation, decreased vocal fremitus, and diminished or absent breath sounds on the affected side. The patient with tension pneumothorax also develops a deviated trachea.
- Pulmonary edema. An early sign of life-threatening pulmonary edema, tachypnea is accompanied by exertional dyspnea, paroxysmal nocturnal dyspnea, and, later, orthopnea. Other features include a dry cough, crackles, tachycardia, and a ventricular gallop. With severe pulmonary edema, respirations become increasingly rapid and labored, tachycardia worsens, and crackles become more diffuse. The patient’s cough also produces frothy, bloody sputum. Signs of shock — such as hypotension, thready pulse, and cool, clammy skin — may also occur.
- Pulmonary embolism (acute). Tachypnea occurs suddenly with pulmonary embolism and is usually accompanied by dyspnea. The patient may complain of angina or pleuritic chest pain. Other common characteristics include tachycardia, a dry or productive cough with blood-tinged sputum, low-grade fever, restlessness, and diaphoresis. Less common signs include massive hemoptysis, chest splinting, leg edema, and — with a large embolus — jugular vein distention and syncope. Other findings include pleural friction rub, crackles, diffuse wheezing, dullness on percussion, diminished breath sounds, and signs of shock, such as hypotension and a weak, rapid pulse.
- Septic shock. Early in septic shock, the patient usually experiences tachypnea; sudden fever; chills; flushed, warm, yet dry skin; and possibly nausea, vomiting, and diarrhea. He may also develop tachycardia and normal or slightly decreased blood pressure. As this life-threatening type of shock progresses, the patient may display anxiety; restlessness; decreased LOC; hypotension; cool, clammy, and cyanotic skin; rapid, thready pulse; thirst; and oliguria that may progress to anuria.
Other Causes
- Salicylates. Tachypnea may result from an overdose of salicylates.
Special Considerations
Continue to monitor the patient’s vital signs closely. Be sure to keep suction and emergency equipment nearby. Prepare to intubate the patient and to provide mechanical ventilation if necessary. Prepare the patient for diagnostic studies, such as arterial blood gas analysis, blood cultures, chest X-rays, pulmonary function tests, and an electrocardiogram.
Patient Counseling
Explain that slight increases in respiratory rate may be normal.
Pediatric Pointers
When assessing a child for tachypnea, be aware that the normal respiratory rate varies with the child’s age. (See Normal Pediatric Vital Signs, page 687.) If you detect tachypnea, first rule out the causes listed above. Then consider these pediatric causes: congenital heart defects, meningitis, metabolic acidosis, and cystic fibrosis. Keep in mind, however, that hunger and anxiety may also cause tachypnea.
Geriatric Pointers
Tachypnea may have a variety of causes in elderly patients — such as pneumonia, heart failure, COPD, anxiety, or failure to take cardiac and respiratory medications appropriately — and mild increases in respiratory rate may be unnoticed.
REFERENCES
Berkowitz, C. D. (2012). Berkowitz’s pediatrics: A primary care approach (4th ed.). USA: American Academy of Pediatrics.
Buttaro, T. M., Tybulski, J., Bailey, P. P., & Sandberg-Cook, J. (2008). Primary care: A collaborative practice (pp. 444–447). St. Louis, MO: Mosby Elsevier.
Colyar, M. R. (2003). Well-child assessment for primary care providers. Philadelphia, PA: F.A. Davis.
Lehne, R. A. (2010). Pharmacology for nursing care (7th ed.). St. Louis, MO: Saunders Elsevier.
McCance, K. L., Huether, S. E., Brashers, V. L., & Rote, N. S. (2010). Pathophysiology: The biologic basis for disease in adults and children. Maryland Heights, MO: Mosby Elsevier.
Sommers, M. S., & Brunner, L. S. (2012). Pocket diseases. Philadelphia, PA: F.A. Davis.
Throat Pain
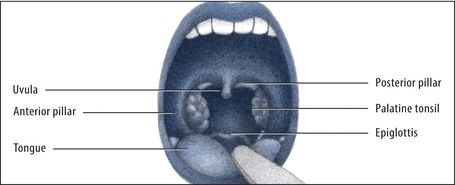
Throat pain — commonly known as a sore throat — refers to discomfort in any part of the pharynx: the nasopharynx, the oropharynx, or the hypopharynx. This common symptom ranges from a sensation of scratchiness to severe pain. It’s commonly accompanied by ear pain because cranial nerves IX and X innervate the pharynx as well as the middle and external ear. (See Anatomy of the Throat.)
Throat pain may result from infection, trauma, allergy, cancer, or a systemic disorder. It may also follow surgery and endotracheal intubation. Nonpathologic causes include dry mucous membranes associated with mouth breathing and laryngeal irritation associated with alcohol consumption, inhaling smoke or chemicals like ammonia, and vocal strain.
History and Physical Examination
Ask the patient when he first noticed the pain, and have him describe it. Has he had throat pain before? Is it accompanied by fever, ear pain, or dysphagia? Review the patient’s medical history for throat problems, allergies, and systemic disorders.
Next, carefully examine the pharynx, noting redness, exudate, or swelling. Examine the oropharynx, using a warmed metal spatula or tongue blade, and the nasopharynx, using a warmed laryngeal mirror or a fiberoptic nasopharyngoscope. Laryngoscopic examination of the hypopharynx may be required. (If necessary, spray the soft palate and pharyngeal wall with a local anesthetic to prevent gagging.) Observe the tonsils for redness, swelling, or exudate. Obtain an exudate specimen for culture. Then examine the nose, using a nasal speculum. Also, check the patient’s ears, especially if he reports ear pain. Finally, palpate the neck and oropharynx for nodules or lymph node enlargement.
Anatomy of the Throat
The throat, or pharynx, is divided into three areas: the nasopharynx (the soft palate and the posterior nasal cavity), the oropharynx (the area between the soft palate and the upper edge of the epiglottis), and the hypopharynx (the area between the epiglottis and the level of the cricoid cartilage). A disorder affecting any of these areas may cause throat pain. Pinpointing the causative disorder begins with accurate assessment of the throat structures as illustrated here.
FRONTAL VIEW
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


