49
Systemic Mycoses
CHAPTER CONTENTS
INTRODUCTION
These infections result from inhalation of the spores of dimorphic fungi that have their mold forms in the soil. Within the lungs, the spores differentiate into yeasts or other specialized forms, such as spherules.
Most lung infections are asymptomatic and self-limited. However, in some persons, disseminated disease develops in which the organisms grow in other organs, cause destructive lesions, and may result in death. Infected persons do not communicate these diseases to others.
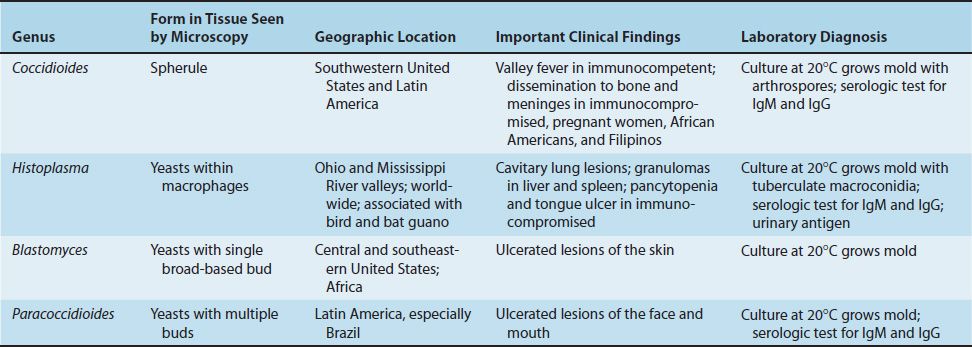
Important features of the systemic fungal diseases are described in Table 49–1. Systemic fungi are also called endemic fungi because they are endemic (localized) to certain geographic areas.
COCCIDIOIDES
Disease
Coccidioides immitis causes coccidioidomycosis.
Properties
C. immitis is a dimorphic fungus that exists as a mold in soil and as a spherule in tissue (Figure 49–1).
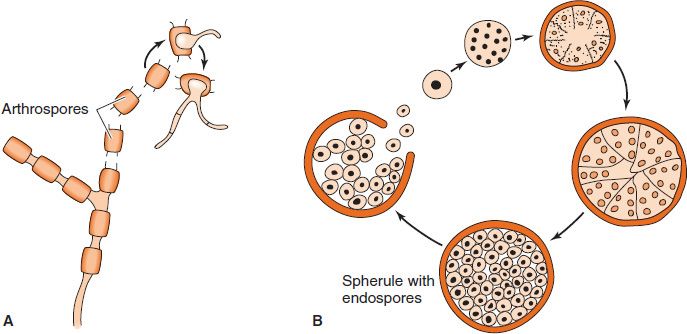
FIGURE 49–1 Stages of Coccidioides immitis. A: Arthrospores form at the ends of hyphae in the soil. They germinate in the soil to form new hyphae. If inhaled, the arthrospores differentiate into spherules. B: Endospores form within spherules in tissue. When spherules rupture, endospores disseminate and form new spherules. (Modified and reproduced with permission from Brooks GF et al. Medical Microbiology. 20th ed. Originally published by Appleton & Lange. Copyright 1995 McGraw-Hill.)
Transmission & Epidemiology
The fungus is endemic in arid regions of the southwestern United States and Latin America. People who live in Central and Southern California, Arizona, New Mexico, Western Texas, and Northern Mexico, a geographic region called the Lower Sonoran Life Zone, are often infected. In soil, it forms hyphae with alternating arthrospores and empty cells (Figure 49–2). Arthrospores are very light and are carried by the wind. They can be inhaled and infect the lungs.
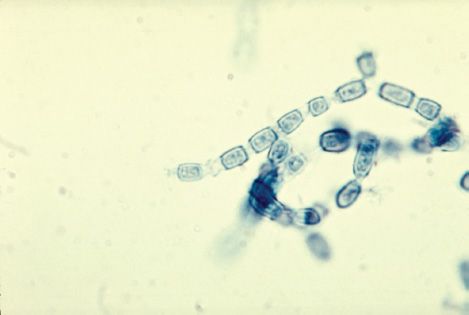
FIGURE 49–2 Coccidioides immitis—arthrospores. Barrel-shaped, rectangular arthrospores appear blue with lactophenol cotton blue stain. Arthrospores are also called arthroconidia. (Figure courtesy of Dr. Hardin, Public Health Image Library, Centers for Disease Control and Prevention.)
Pathogenesis
In the lungs, arthrospores form spherules that are large (30 μm in diameter), have a thick, doubly refractive wall, and are filled with endospores (Figure 49–3). Upon rupture of the wall, endospores are released and differentiate to form new spherules. The organism can spread within a person by direct extension or via the bloodstream. Granulomatous lesions can occur in virtually any organ but are found primarily in bones and the central nervous system (meningitis).
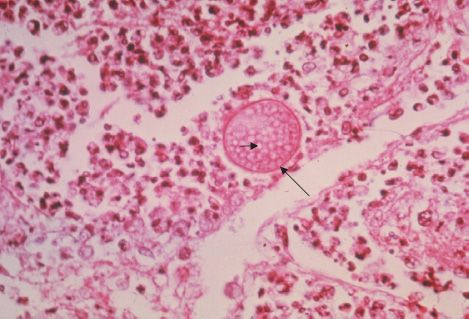
FIGURE 49–3 Coccidioides immitis—spherule. Long arrow points to a spherule in lung tissue. Spherules are large thick-walled structures containing many endospores. Short arrow points to an endospore. (Figure courtesy of Dr. L. Georg, Public Health Image Library, Centers for Disease Control and Prevention.)
Dissemination from the lungs to other organs occurs in people who have a defect in cell-mediated immunity. Most people who are infected by C. immitis develop a cell-mediated (delayed hypersensitivity) immune response that restricts the growth of the organism. One way to determine whether a person has produced adequate cell-mediated immunity to the organism is to do a skin test (see later). In general, a person who has a positive skin test reaction has developed sufficient immunity to prevent disseminated disease from occurring. If, at a later time, a person’s cellular immunity is suppressed by drugs or disease, disseminated disease can occur.
Clinical Findings
Infection of the lungs is often asymptomatic and is evident only by a positive skin test and the presence of antibodies. Some infected persons have an influenzalike illness with fever and cough. About 50% have changes in the lungs (infiltrates, adenopathy, or effusions) as seen on chest X-ray, and 10% develop erythema nodosum (see later) or arthralgias. This syndrome is called “valley fever” (in the San Joaquin Valley of California) or “desert rheumatism” (in Arizona); it tends to subside spontaneously.
Disseminated disease can occur in almost any organ; the meninges (meningitis), bone (osteomyelitis), and skin (nodules) are important sites. The overall incidence of dissemination in persons infected with C. immitis is 1%, although the incidence in Filipinos and African Americans is 10 times higher. Women in the third trimester of pregnancy also have a markedly increased incidence of dissemination. Erythema nodosum (EN) manifests as red, tender nodules (“desert bumps”) on extensor surfaces such as the skin over the tibia and ulna. It is a delayed (cell-mediated) hypersensitivity response to fungal antigens and thus is an indicator of a good prognosis. There are no organisms in these lesions; they are not a sign of disseminated disease. EN is not specific for coccidioidomycosis; it occurs in other granulomatous diseases (e.g., histoplasmosis, tuberculosis, and leprosy).
In infected persons, skin tests with fungal extracts (coccidioidin or spherulin) cause at least a 5-mm induration 48 hours after injection (delayed hypersensitivity reaction). Skin tests become positive within 2 to 4 weeks of infection and remain so for years but are often negative (anergy) in patients with disseminated disease.
Laboratory Diagnosis
In tissue specimens, spherules are seen microscopically. Cultures on Sabouraud’s agar incubated at 25°C show hyphae with arthrospores (Figure 49–2). (Caution: Cultures are highly infectious; precautions against inhaling arthrospores must be taken.) In serologic tests, IgM and IgG precipitins appear within 2 to 4 weeks of infection and then decline in subsequent months. Complement-fixing antibodies occur at low titer initially, but the titer rises greatly if dissemination occurs.
Treatment & Prevention
No treatment is needed in asymptomatic or mild primary infection. Amphotericin B (Fungizone) or itraconazole is used for persisting lung lesions or disseminated disease. Ketoconazole is also effective in lung disease. If meningitis occurs, fluconazole is the drug of choice. Intrathecal amphotericin B may be required and may induce remission, but long-term results are often poor. There are no means of prevention except avoiding travel to endemic areas. Patients who have recovered from coccidioidal meningitis should receive long-term suppressive therapy with fluconazole to prevent a recurrence.
HISTOPLASMA
Disease
Histoplasma capsulatum causes histoplasmosis.
Properties
H. capsulatum is a dimorphic fungus that exists as a mold in soil and as a yeast in tissue. It forms two types of asexual spores (Figure 49–4): (1) tuberculate macroconidia, with typical thick walls and fingerlike projections that are important in laboratory identification; and (2) microconidia, which are smaller, thin, smooth-walled spores that, if inhaled, transmit the infection.
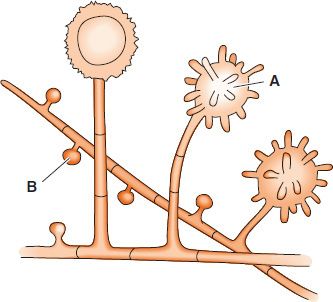
FIGURE 49–4 Asexual spores of Histoplasma capsulatum. A: Tuberculate macroconidia. B: Microconidia. (Reproduced with permission from Brooks GF et al. Medical Microbiology. 19th ed. Originally published by Appleton & Lange. Copyright 1991 McGraw-Hill.)
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


