Stress
LANGUAGE OF SCIENCE
 Before reading the chapter, say each of these terms out loud. This will help you avoid stumbling over them as you read.
Before reading the chapter, say each of these terms out loud. This will help you avoid stumbling over them as you read.
[adapt- adjust, -ation process]
[allo- different, -stasis standing still]
[cortic- cortex or bark, -oid like]
[fet- offspring, -al relating to]
hypothalamic-pituitary-adrenal axis (HPA)
(hye-poh-THAL-ah-mik pi-TOO-itair-ee ah-DREE-nal)
[neuro- nerve, -pept- digest, -ide chemical]
[psycho- the mind, –logos- words (study), -al relating to, stress- tighten, -or agent]
[stress- tighten, triad group of three]
LANGUAGE OF MEDICINE
SELYE’S CONCEPT OF STRESS
In 1935, Hans Selye of McGill University in Montreal made an accidental discovery that launched him on a lifelong career and led him to conceive the idea of stress. This chapter tells briefly the story of how Selye developed his stress concept and also describes the mechanism of stress that he postulated. It then presents some current ideas about stress.
Development of the Stress Concept
Selye made his accidental discovery when he was trying to determine whether there was another sex hormone besides those already known. He injected rats with various extracts derived from ovaries and placenta, expecting to find different changes had occurred in animals injected with different hormonal preparations. But to his surprise and puzzlement, he found the same three changes in all the animals. The cortices of their adrenal glands were enlarged, but their lymphatic organs—thymus glands, spleens, and lymph nodes—were atrophied, and bleeding ulcers of the stomach and duodenum had developed in every animal. Next he injected many other substances, for example, extracts from pituitary glands, kidneys, and spleens and even a poison, formaldehyde. Every time he found the same three changes in the animal subjects: enlarged adrenals, shrunken lymphatic organs, and bleeding gastrointestinal ulcers. Selye believed that these symptoms were a specific syndrome.
A syndrome, according to the classical definition, is a set of signs and symptoms that occur together and that characterize one particular disease. The three changes, or “stress triad,” Selye had observed occurred together, but they seemed to characterize not any one particular kind of injury but instead all kinds of harmful stimuli. More experiments using various chemicals and injurious agents confirmed for him that the three changes truly were a syndrome of injury. His first publication on the subject was a short paper entitled “A Syndrome Produced by Diverse Nocuous Agents”; it appeared in the July 1936 issue of the British journal Nature. Years later, in 1956, he published his monumental technical treatise, The Stress of Life.
Although a majority of the current literature credits Hans Selye with the first published reports on stress, Walter B. Cannon used the term “emotional stress” much earlier (1914) when discussing his theory of homeostasis. It seems Cannon was also convinced stress had both a psychological (emotional) and a physiological origin. It was Selye, however, who brought our knowledge of stress and its importance in health and disease into the forefront of modern medicine.
Definitions
Stress, according to Selye’s use of the word, is a state, or condition, of the body produced by “diverse nocuous agents” and manifested by a syndrome of changes. We know as well that stress and its negative effects can also be caused by a wide variety of mental, emotional, and other psychological events that an individual may perceive as threatening or undesirable. Selye named the agents that produce stress stressors and coined a name—general adaptation syndrome (GAS)—for the syndrome or group of changes that make the presence of stress in the body known.
Stressors
A stressor is any agent or stimulus that produces stress. However, just how an individual interacts with or relates to a particular type of physiological or cognitive situation may well determine whether that particular event is stressful or not. Even the same intensity of a particular physiological stressor, such as temperature change, may be perceived as a threat and activate a stress response in one individual and not another.
In addition to variances in ability to handle physiological stress, some people have the ability to cope better than others when faced with difficult events in life, such as divorce or bereavement. As a result, they suffer less from negative stress-related symptoms or illness.
Clearly, a precise classification of stimuli as stressors or nonstressors is not possible. We can, however, make these five generalizations about the character of stressors.
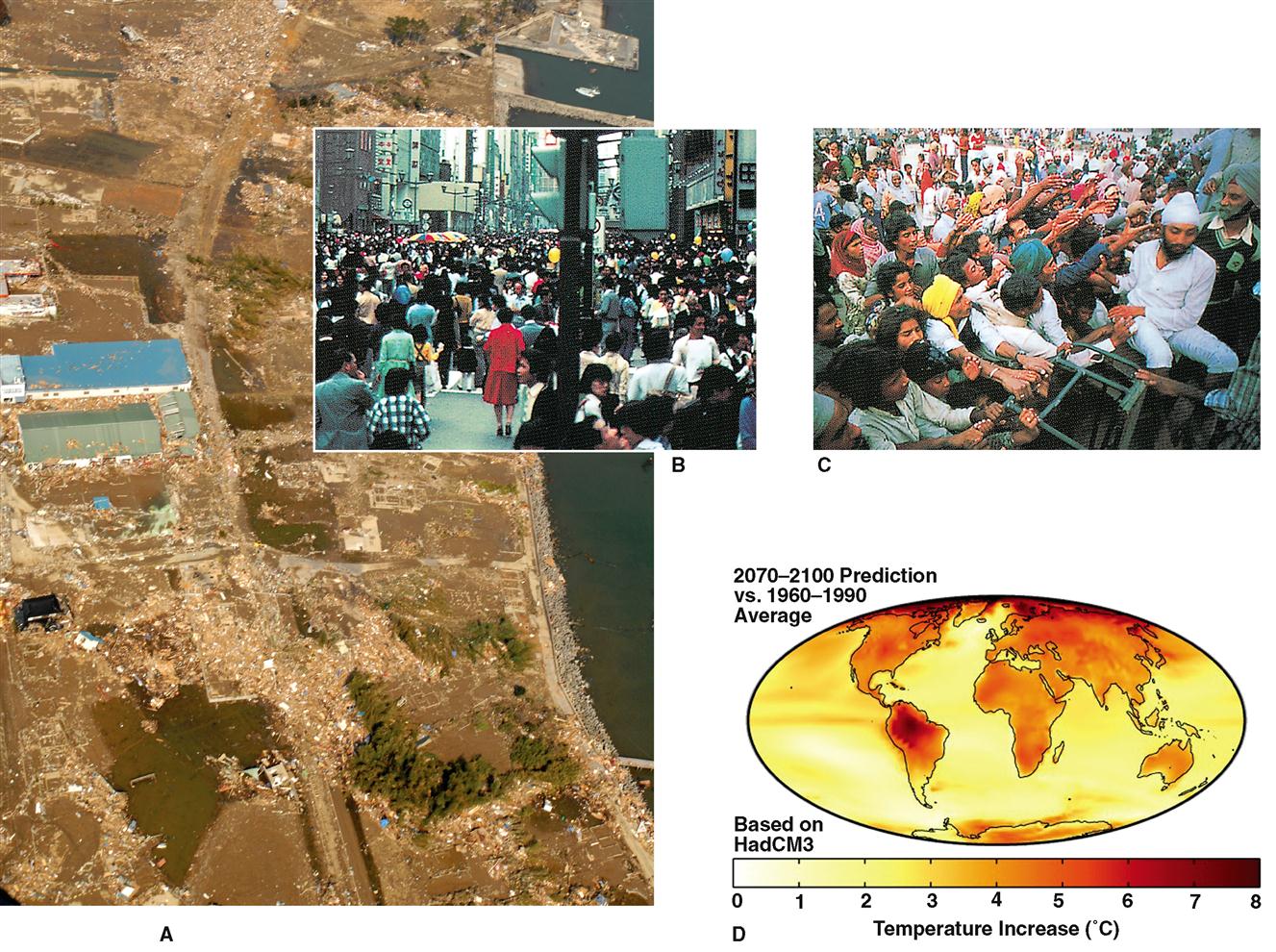
1. Stressors are extreme stimuli—too much or too little of almost anything. The perception of the individual is critical. A particular event or circumstance that is viewed as undesirable or goes beyond what the individual is capable of coping with may be viewed as “extreme” and cause one or more of the psychological or physiological responses associated with stress. In contrast, almost anything in moderation or that engenders only mild stimuli are nonstressors. Thus coolness, warmth, and soft sounds are nonstressors, whereas extreme cold, extreme heat, and extremely loud sounds almost always act as stressors. Not only extreme excesses but also extreme deficiencies may be perceived as stressors. One example of this kind of stressor is an extreme lack of social contact stimuli. Solitary confinement in a prison, space travel, social isolation because of blindness or deafness, and in some cases, old age have all been identified as stressors. But the opposite extreme, an excess of social contact stimuli (e.g., caused by overcrowding), also acts as a stressor (Figure 25-1). We now know that various types of stress in young children and even prenatal infants may occur as a result of negative stimuli that are experienced by a parent. For example, severe psychological or physical trauma, environmental hazards, and nutritional deficiencies or abuses, when encountered by a pregnant or nursing woman, can all have a stress-related impact on her child that may result in immediate or delayed behavioral, physiological, or anatomical anomalies. Intrauterine stress is discussed in detail later in the chapter. Poverty and illness, typically associated with stress, are often coupled with alcoholism, drug abuse, and malnutrition. These conditions often result either directly or indirectly in premature births, developmental anomalies, increased susceptibility to many types of mental and physical diseases, and a myriad of other physical defects that may occur immediately in the children involved or these conditions may develop later in life.
5. Stress can occur even in a developing fetus—a circumstance called prenatal stress. In many instances prenatal stress will result from a physical or nutritional stressor experienced by the mother. For example, in the United States alone, fetal alcohol syndrome (FAS) affects more than 40,000 infants each year (see Box 18-3 on p. 556). FAS involves signs ranging from poor prenatal and infant growth to mental retardation. In this context, alcohol consumed during pregnancy is a dangerous stressor. Even in small amounts it can produce prenatal brain damage that may permanently affect the ability of the child to concentrate, think abstractly, use appropriate judgment, or learn effectively. When a woman consumes alcohol during pregnancy, real or perceived stress is often the impetus for such behavior. Education that promotes healthy habits and teaches coping strategies must be a part of any social programs intended to eliminate alcohol consumption during pregnancy and the incidence of FAS.
General Adaptation Syndrome
MANIFESTATIONS
Stress, like health or any other state or condition, is an intangible phenomenon. It cannot be seen, heard, tasted, smelled, felt, or measured directly. How, then, can we know that stress exists? It can be inferred to exist when certain visible, tangible, and measurable responses occur. Selye, for example, inferred that the animals on which he experimented were in a state of stress when he found the syndrome of the three changes previously noted—hypertrophied adrenals, atrophied lymphatic organs, and bleeding gastrointestinal ulcers. Because this syndrome indicated the presence of stress and consisted of three changes, he called them the “stress triad.”
Eventually he found that many other changes also took place as a result of stress. He named the entire group of changes or responses the general adaptation syndrome (GAS). In coining this term, he reasoned that the word general suggested that the syndrome was “produced only by agents that have a general effect on large portions of the body.” The word adaptation was meant to imply that the syndrome of changes made it possible for the body to adapt, to cope successfully with stress. Selye thought that these responses seemed to protect the animals from serious damage by extreme stimuli and to promote their healthy survival. He looked on the general adaptation syndrome as a crucial part of the body’s complex defense mechanism.
STAGES
Changes that make up the general adaptation syndrome do not all take place simultaneously but over time in three stages. Selye named these stages: (1) the alarm reaction, (2) the stage of resistance or adaptation, and (3) the stage of exhaustion. A different syndrome of changes, he noted, characterized each stage.
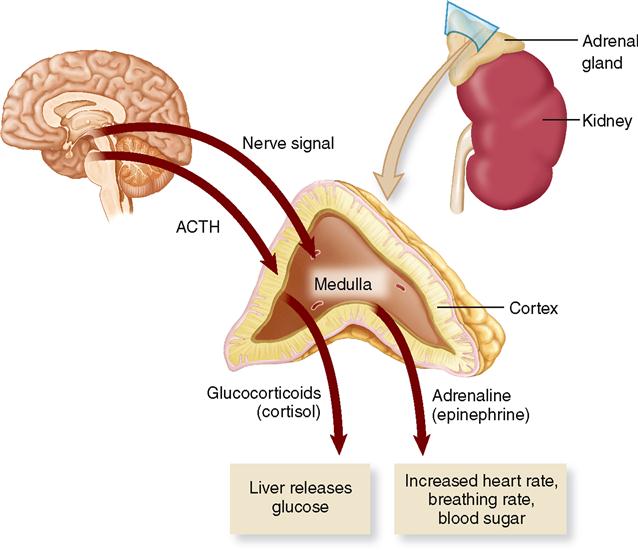
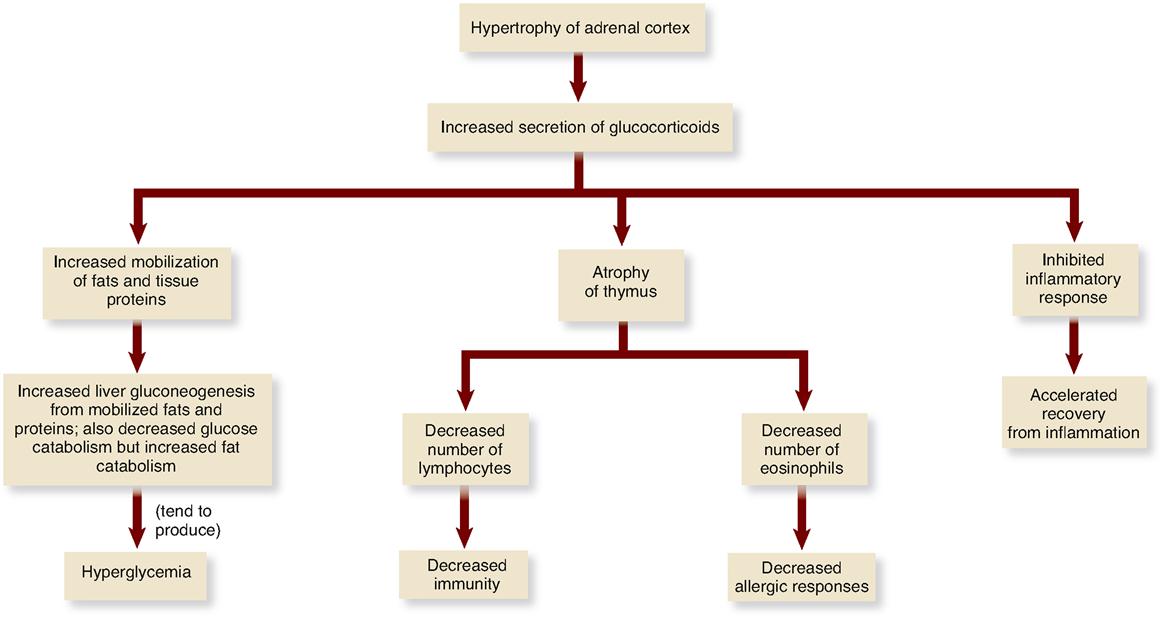
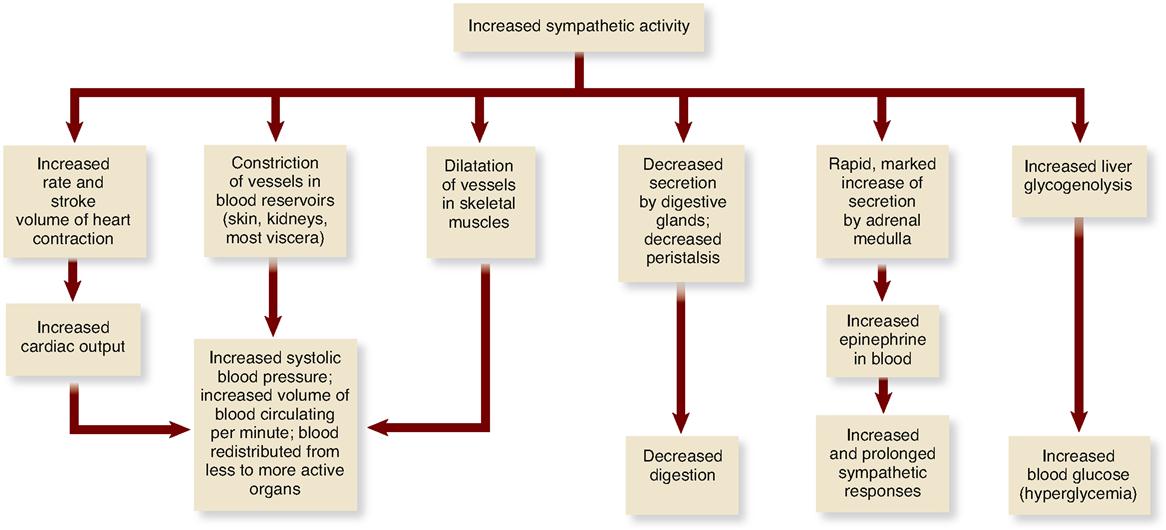
Among the responses characteristic of the alarm reaction, for example, were the stress triad already described—hypertrophied adrenal cortex, atrophied lymphatic organs (thymus, spleen, lymph nodes), and bleeding gastric and duodenal ulcers. In addition, the adrenal cortex increased its secretion of glucocorticoids, the number of lymphocytes decreased markedly, and so, too, did the number of eosinophils. Also, the sympathetic nervous system and the adrenal medulla greatly increased their activity (Figure 25-2). Each of these changes, in turn, produced other widespread changes. Figure 25-3 indicates some of the changes stemming from adrenal cortical hypertrophy. Figure 25-4 shows responses produced by increased sympathetic activity and increased secretion by the adrenal medulla of its hormone, epinephrine (adrenaline).
Quite different responses characterize the stage of resistance. For instance, the adrenal cortex and medulla return to their normal rates of hormone secretion. The changes that take place during the alarm stage as a result of increased corticoid secretion disappear during the stage of resistance. All of us go through the first and second stages of the stress syndrome many times in our lifetimes. Stressors of one kind or another act on most of us every day. They may upset or alarm us, but we soon resist them successfully. In short, we adapt; we cope.
The stage of exhaustion develops only when stress is extremely severe or when it continues over long periods. Otherwise, when stress is mild and of short duration, it ends with a successful stage of resistance and adaptation to the stressor. If stress continues until the body reaches the stage of exhaustion, corticoid secretion and adaptation eventually decrease markedly. The body can no longer cope successfully with the stressor and death may ensue as a result. For a brief summary of the changes characteristic of the three stages of the general adaptation syndrome, see Table 25-1.
TABLE 25-1
The Three Stages of the General Adaptation Syndrome
| ALARM | RESISTANCE | EXHAUSTION |
| Increased secretion of glucocorticoids and resultant changes (see Figure 25-2) | Glucocorticoid secretion returns to normal | Initially increased glucocorticoid secretion but eventually markedly decreased secretion |
| Increased activity of sympathetic nervous system | Sympathetic activity returns to normal | Stress triad (hypertrophied adrenals, atrophied thymus and lymph nodes, bleeding ulcers in stomach and duodenum) |
| Increased norepinephrine secretion by adrenal medulla | Norepinephrine secretion returns to normal | |
| Fight-or-flight reaction (see Figure 25-4) | Fight-or-flight reaction disappears | |
| Low resistance to stressors | High resistance (adaptation) to stressor | Loss of resistance to stressor; may lead to death |
Mechanism of Stress
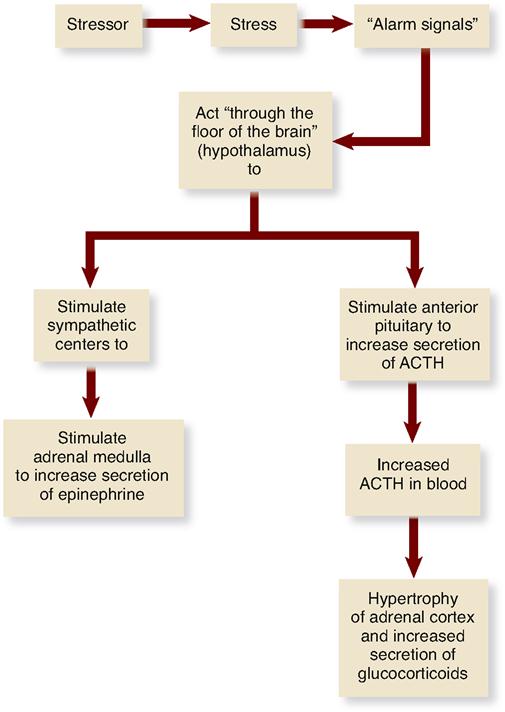
Stressors produce a state of stress. A state of stress in turn inaugurates a series of responses that Selye called the general adaptation syndrome. More simply, a state of stress turns on the stress response mechanism. It activates the organs that produce the responses that make up the general adaptation syndrome; but just how stress—a state of the body—does this is not clear. Selye could only guess about it, and his terms were vague. For instance, he postulated that, by some unknown “alarm signals,” stress “acted through the floor of the brain” (presumably the hypothalamus) to stimulate the sympathetic nervous system and the pituitary gland.
In Figure 25-5 you can see Selye’s hypothesis in diagram form. Many scientists refer to this process as the hypothalamic-pituitary-adrenal “axis,” or HPA mechanism.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


