Squamous Metaplasia of Lactiferous Ducts
Key Facts
Terminology
Squamous metaplasia of lactiferous ducts (SMOLD) is also known as recurrent subareolar abscess, periductal mastitis, and Zuska disease
Etiology/Pathogenesis
Keratin-producing cells extend abnormally deep into lactiferous sinuses
“Epidermal inclusion cyst” filled with keratin forms in sinuses
When ruptured, an intense inflammatory response ensues
Almost all men and women affected by SMOLD have history of tobacco use
May reduce vitamin A levels resulting in abnormal metaplasia
Clinical Issues
Presents with an erythematous painful subareolar mass
Recurrences are common if the lesion is treated as a bacterial abscess
Fistula track may develop
Effective surgical management reduces likelihood of recurrence
Secondary infections, often due to mixed anaerobes, may occur after surgical intervention
Top Differential Diagnoses
Bacterial abscess
Duct ectasia
Biopsy site changes
Granulomatous lobular mastitis
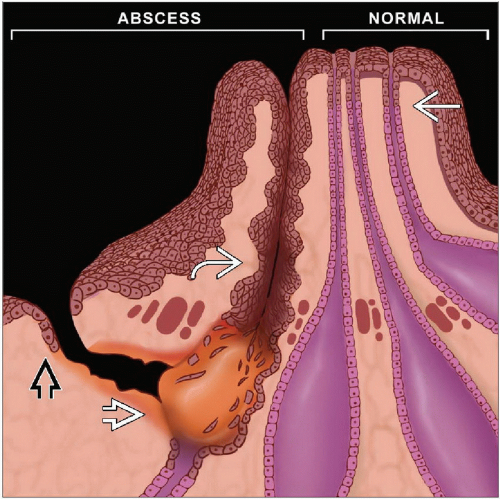 The normal keratinizing surface epithelium normally dips into the nipple orifice for only 2-3 mm  . If keratin production occurs deeper in the duct . If keratin production occurs deeper in the duct  , the keratin is trapped and causes distension of the duct. If rupture occurs, an intense foreign body inflammatory response to the keratin ensues , the keratin is trapped and causes distension of the duct. If rupture occurs, an intense foreign body inflammatory response to the keratin ensues  . The patient develops an erythematous painful subareolar mass, often mistaken for a bacterial infection. Incision and drainage procedure does not remove the pathologic lesion, and recurrences are common. The path of least resistance is beneath the smooth muscle of the nipple. Patients may develop a fistula track opening at the edge of the areola . The patient develops an erythematous painful subareolar mass, often mistaken for a bacterial infection. Incision and drainage procedure does not remove the pathologic lesion, and recurrences are common. The path of least resistance is beneath the smooth muscle of the nipple. Patients may develop a fistula track opening at the edge of the areola  . Definitive surgery removes the offending duct. . Definitive surgery removes the offending duct. |
TERMINOLOGY
Abbreviations
Squamous metaplasia of lactiferous ducts (SMOLD)
Synonyms
Recurrent subareolar abscess
Zuska disease
Periductal mastitis
Definitions
Abnormal keratin formation in lactiferous sinuses leads to rupture and intense inflammatory response to keratin debris
ETIOLOGY/PATHOGENESIS
Etiology
Tobacco use
Almost all men and women affected by SMOLD have history of tobacco use
It has been proposed that smoking leads to vitamin A deficiency, which results in abnormal squamous metaplasia
Inverted nipple
Many patients with SMOLD have inverted nipple
Inversion of nipple is more likely a result of retroareolar inflammation and fibrosis rather than a cause of the condition
Recurrent episodes of inflammation and healing with fibrosis lead to nipple retraction
Subareolar abscess formation
Keratinizing cells extend abnormally deep into lactiferous sinuses
Keratin becomes trapped and equivalent of an epidermal inclusion cyst is formed
If duct ruptures, keratin is released into surrounding tissue
Intense inflammatory response ensues, causing erythema, swelling, and pain
If involved duct is not removed, recurrences are common
CLINICAL ISSUES
Epidemiology
Incidence
Rare: < 1% of all breast biopsies
Age
Occurs at any adult age
Gender
Occurs in both females and males
Presentation
Patients initially present with erythematous painful subareolar mass
Usually mistaken for bacterial abscess
Initial lesions are sterile; inflammatory response is to keratin debris
Typical treatment is incision and drainage (I&D) and antibiotics for Staphylococcus species
Surgeons avoid surgery involving nipple due to cosmetic and functional concerns
Symptoms may be relieved temporarily
Recurrences are common
Often mystify patient and clinicians, as adequate treatment for an infection has been provided
Patients have been suspected of having Munchausen syndrome
Subsequent treatment may again be I&D and antibiotics
Secondary infections may occur
Fistula track may form after recurrences
Path of least resistance is below smooth muscle of areola
Track opens at edge of areola
Only 1 track is present
Treatment
Effective treatment requires surgical removal of keratin-producing epithelium
Wedge resection of nipple to remove involved duct may be performed
If a fistula track is present, it should be removed in continuity with involved duct
Antibiotics may be required for recurrent lesions with secondary infections
Secondary infections are often due to mixed anaerobic bacteria
Cultures are often helpful to establish type of bacteria and sensitivity to antibiotics
Prognosis
After effective surgical management, recurrences are uncommon
Termination of tobacco use may reduce likelihood of recurrence
IMAGE FINDINGS
Mammographic Findings
Patient may not tolerate compression due to painful mass
Location of lesion below nipple also makes it difficult to visualize
In some patients, a density may be present due to inflammatory reaction
Ultrasonographic Findings
May not be possible, as patient may not tolerate pressure from transducer
In some patients, a mass with irregular margins is present
MR Findings
MR may be better tolerated, as compression is not required
In 1 study, MR was effective in imaging abscess cavity and associated fistula track
MACROSCOPIC FEATURES
General Features
1st specimen is often an I&D
Specimen consists of multiple fragments of tissue that cannot be oriented
If a definitive procedure is performed, there should be a small fragment of nipple skin and the underlying abscess cavity
If possible, sections should be oriented perpendicular to nipple skin
MICROSCOPIC PATHOLOGY
Histologic Features
I&D specimens usually consist of tissue from center of abscess
Findings may be nonspecific, consisting of chronic active inflammation
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


