• Spitzoid melanoma; findings suspicious for melanoma include
Patients usually > 10 years old
Lesions usually > 1 cm
Ulceration and increased mitoses often present
Asymmetry and poor circumscription
Subcutaneous involvement
• Pigmented spindle cell nevus of Reed (usually leg of young adult female)
• Conventional melanocytic nevi
Clinical Photograph of Spitz Nevus A small, symmetric pink papule, typical of a Spitz nevus, is shown on the face of a child. (Courtesy R. J. Antaya, MD.)
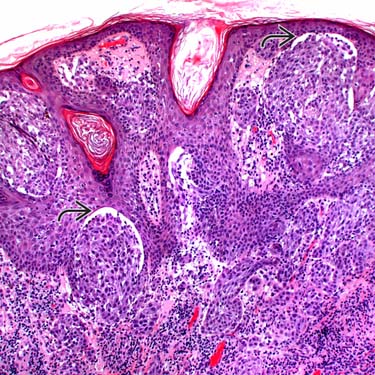
Classic Spitz Nevus Histologic examination of a classic Spitz nevus shows nests of spindled and epithelioid-shaped melanocytes at the dermal-epidermal junction and in the dermis. Note the clefting artifact overlying several of the nests .
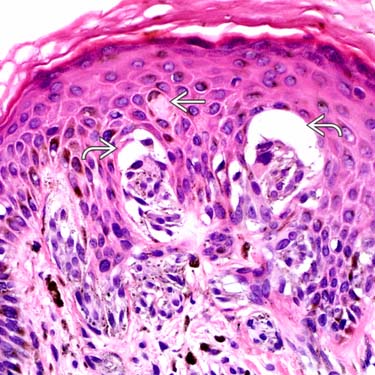
Spitz Nevus at High Magnification High-power examination of a Spitz nevus shows small nests of epithelioid to spindled melanocytes with overlying artifactual clefting and an eosinophilic Kamino body .
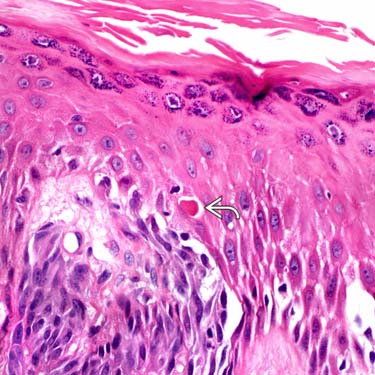
Kamino Body in Spitz Nevus High-power examination of this case shows a small, densely eosinophilic-staining Kamino body , which is an eosinophilic globule found at the dermal-epidermal junction. These are typical of Spitz nevi but are not seen in most cases.
TERMINOLOGY
Synonyms
• Spindle and epithelioid cell nevus
• Spindle cell nevus
• Epithelioid cell nevus
• Nevus of large spindle &/or epithelioid cells
• Benign juvenile melanoma (outdated term)
CLINICAL ISSUES
Site
• Trunk
• Head and neck
• Extremities, especially thigh
Presentation
• Most common in children and young adults
0.5-1.0% of all nevi in children and adolescents
May occur at all ages
• Solitary
Can be clustered or disseminated
Treatment
• Complete conservative excision
Prognosis
• Benign tumors; only very rare malignant transformation
• Low recurrence rate, even after incomplete excision
MACROSCOPIC
General Features
• Dome-shaped dermal nodule
• Pink or flesh colored
• Often misdiagnosed clinically as hemangioma or pyogenic granuloma
Size
• Usually < 1 cm
MICROSCOPIC
Histologic Features
• Junctional, compound, and dermal forms
Most common type is compound with prominent dermal component
• Symmetric, well-circumscribed proliferation
Usually no lateral extension of junctional nests beyond dermal component
• Varying proportions of spindled and epithelioid melanocytes
Spindle cells more common in most cases
– Completely spindle cells in ~ 45% of Spitz nevi
– Mixed spindle and epithelioid cells in ~ 35%
– Only epithelioid cells in ~ 20%
Epithelioid cells usually dispersed individually throughout lesion
• Spindle cells are arranged in fascicles perpendicular to epidermis
• Small clusters of melanocytes can be seen in epidermis
Can see pagetoid spread of few single melanocytes
• Artifactual clefting of junctional nests from overlying epidermis
• Kamino bodies
Eosinophilic globules at dermal-epidermal junction
Important diagnostic clue, but not always seen (may need step sections to find)
PAS(+) and trichrome (+)
• Melanocytes show “maturation” as they become smaller from superficial to deep
Melanocytes often taper to narrower areas in deep dermis, forming upside-down triangle
Only gold members can continue reading. Log In or Register to continue









 .
.
 and an eosinophilic Kamino body
and an eosinophilic Kamino body  .
.
 , which is an eosinophilic globule found at the dermal-epidermal junction. These are typical of Spitz nevi but are not seen in most cases.
, which is an eosinophilic globule found at the dermal-epidermal junction. These are typical of Spitz nevi but are not seen in most cases.















