Spindle Cell Rhabdomyosarcoma
Khin Thway, BSc, MBBS, FRCPath
Key Facts
Terminology
Uncommon subtype of rhabdomyosarcoma occurring in both children and adults; composed of largely cellular proliferation of predominantly spindled cells
Clinical Issues
Behavior appears to vary significantly between children and adults, suggesting these are distinct clinicopathological subtypes
Good prognosis in children (when compared to other RMS subtypes)
Clinically aggressive in adults
Children
Most tumors occur in paratesticular region
Adults
Most common in head and neck region (> 50% of cases)
Retroperitoneum
Extremities
Trunk
Vulva
Microscopic Pathology
Long or intersecting fascicles
Atypical spindle cells
Elongated, vesicular nuclei
Scattered spindle or polygonal rhabdomyoblasts
Ancillary Tests
Desmin(+)
Myogenin(+) and MYOD1(+)
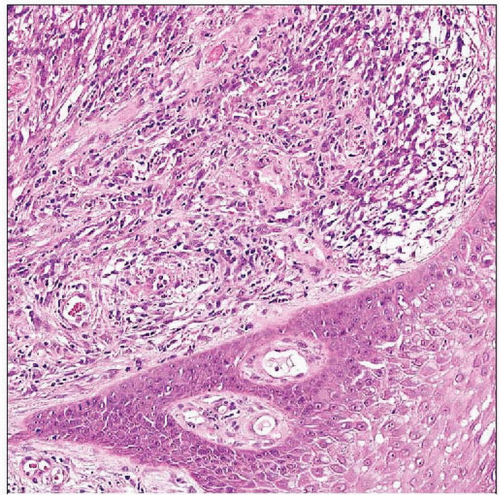 Low-power view of adult-type spindle cell rhabdomyosarcoma, in which laryngeal squamous epithelium overlies cellular tumor, shows sheets of mildly atypical cells within collagenous stroma. |
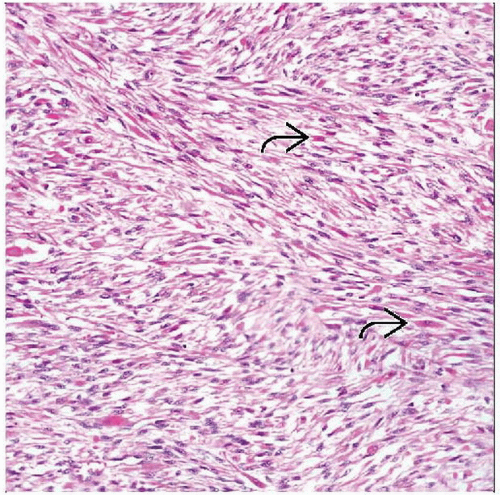 Juvenile-type spindle cell rhabdomyosarcoma shows sweeping fascicles of spindled cells present in a collagenous matrix. Focal rhabdomyoblastic differentiation is evident  , even at low power. , even at low power. |
TERMINOLOGY
Abbreviations
Spindle cell rhabdomyosarcoma (RMS)
Definitions
Uncommon subtype of rhabdomyosarcoma occurring in both children and adults; composed of largely cellular proliferation of predominantly spindled cells
Spindle cell RMS in children is considered variant of embryonal RMS
Carries good prognosis compared to other RMS subtypes
Adult-type spindle cell rhabdomyosarcoma is aggressive neoplasm
CLINICAL ISSUES
Epidemiology
Age
Children
< 10 years
Adults
All adult age groups (2nd-8th decades)
Median: Approximately 4th-5th decades
Gender
Male preponderance
Site
Children
Most tumors occur in paratesticular region
Adults
Most common in head and neck region
> 50% of cases
Retroperitoneum
Extremities
Trunk
Vulva
Paratesticular region
Tumors usually deeply located
Presentation
Suddenly enlarging mass
Local symptoms pertaining to site of origin
Prognosis
Behavior varies significantly between children and adults, suggesting distinct clinicopathologic subtypes
Good prognosis in children (when compared to other RMS subtypes)
Clinically aggressive in adults
Lymph node or blood-borne metastases
MACROSCOPIC FEATURES
General Features
Firm white mass
Size
Variable: 1-30 cm
Mean: 8 cm
MICROSCOPIC PATHOLOGY
Histologic Features
Juvenile type
Fascicular architecture
Sweeping or loose fascicles
Some tumors have storiform pattern
Usually hypercellular
Spindle cells
Elongated nuclei
Nuclei can be vesicular or hyperchromatic
Nucleoli may be prominent
Pale or amphophilic fibrillary cytoplasm
Cross-striations
Prominent cell borders
Rhabdomyoblasts
Variable numbers
Spindle or polygonal
Variable amounts of intervening collagen
Collagen-rich type shows abundant collagen fibers, with cells in short fascicles or storiform arrangements
Collagen-poor type is more cellular
Mitotic figures usually prominent
Frankly pleomorphic areas absent
No round cell foci
Adult type
Long or intersecting fascicles
Atypical spindle cells
Elongated, vesicular nuclei
Pale or amphophilic fibrillary cytoplasm
Scattered spindle or polygonal rhabdomyoblasts
Usually present in small numbers
Abundant eosinophilic cytoplasm
Prominent mitoses with atypical forms
Necrosis in some tumors
Sclerosing pseudovascular features in a smaller number
No round cell or pleomorphic areas
ANCILLARY TESTS
Immunohistochemistry
Desmin(+)
Characteristically strong and diffuse cytoplasmic expression
Myogenin(+) and MYOD1(+)
Myogenic nuclear regulatory proteins
Nuclear expression is specific for RMS
May be scanty or focal
Any cytoplasmic staining should be disregarded
HHF-35 (muscle specific actin)(+)
SMA frequently positive
Occasional cases cytokeratin and epithelial membrane antigen positive
H-caldesmon(-)
S100 protein(-)
DIFFERENTIAL DIAGNOSIS
Rhabdomyoma
Predilection for head and neck
Especially fetal type
Fetal rhabdomyoma
No atypia or necrosis
Mitoses usually absent
Adult rhabdomyoma
Male preponderance
Circumscribed lesion
Large polygonal cells, abundant cytoplasm
Genital rhabdomyoma
Mostly middle-aged women
Mostly vagina; also vulva and cervix
Desmoid Fibromatosis
Long fascicles of spindle and stellate myofibroblasts
Vesicular nuclei
Small pinpoint nucleoli
Fibrillary cytoplasm
No cytologic atypia
Distinct vascular pattern
Small thick-walled and larger thin-walled vessels
Prominent collagenous stroma
Nuclear β-catenin expression
Desmin usually negative
Focal and weak expression of actins
β-catenin or APC mutations
Nodular Fasciitis
Short history
Typically smaller lesions in younger adults
Mostly superficially located
Loose storiform rather than fascicular pattern
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


