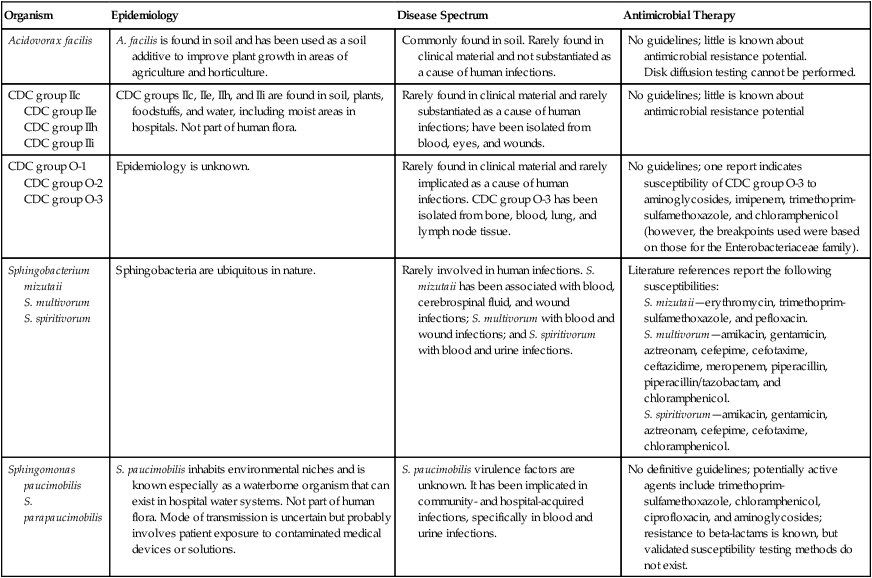
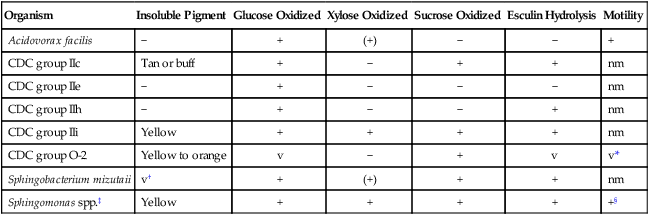
1. Identify cultivation methods and colonial characteristics for Sphingomonas paucimobilis and similar organisms. 2. State the initial clues that alert the CL to the presence of this group of organisms for clinical laboratorians. 3. Select identification approaches for this group of organisms. 4. Identify susceptibility testing methods appropriate for this group of organisms. As demonstrated in Table 27-1, these organisms are rarely or only occasionally isolated from human materials and have limited roles as agents of infection. Because they are infrequently encountered in the clinical setting, little information is available on their epidemiology, ability to cause human infections, and potential for antimicrobial resistance. For example, even though O-1 and O-2 organisms have been submitted to the Centers for Disease Control and Prevention (CDC) after being isolated from clinical materials such as blood, cerebrospinal fluid (CSF), wounds, and pleural fluid, their natural habitat is unknown. The genus Sphingobacterium is ubiquitous in nature, and Sphingomonas spp. are known for their waterborne nature. Some of these groups are present in hospital settings, such as hospital water supplies. When the organisms discussed in this chapter are encountered in clinical specimens, their clinical significance and potential as contaminants should be considered; human infections have been documented, so care must be taken to determine whether these organisms are infectious agents or contaminants. TABLE 27-1 Epidemiology, Spectrum of Disease, and Antimicrobial Therapy No special considerations are required for specimen collection and transport of the organisms discussed in this chapter. Refer to Table 5-1 for general information on specimen collection and transport. Table 27-2 describes the colonial appearance and distinguishing characteristics (e.g., pigment) of each organism on 5% sheep blood agar. When these organisms do grow on MacConkey agar, they appear as lactose nonfermenters. TABLE 27-2 Colonial Appearance and Characteristics BA, 5% sheep blood agar. The ability of many commercial identification systems to identify accurately the organisms discussed in this chapter may be limited or uncertain. Tables 27-3 through 27-6 show some biochemical tests that are helpful for presumptive differentiation among the various organisms in this group. TABLE 27-3 Key Biochemical and Physiologic Characteristics nm, Nonmotile; v, variable; +, >90% strains positive; −, >90% strains negative; (+), delayed. *Only 20% are motile; motility is only apparent upon wet mount or flagellar staining. †Yellow pigment production may be enhanced by incubation at room temperature. ‡Includes S. paucimobilis and S. parapaucimobilis. §Usually nonmotile in motility medium, but motility is present on wet mount. Data compiled from Daneshvar MI, Hill B, Hollis DG et al: CDC group O-3: phenotypic characteristics, fatty acid composition, isoprenoid quinone content, and in vitro antimicrobic susceptibilities of an unusual gram-negative bacterium isolated from clinical specimens, J Clin Microbiol 36:1674, 1998; Hollis DG, Moss CW, Daneshvar MI, Wallace-Shewmaker PL: CDC group IIc phenotypic characteristics, fatty acid composition, and isoprenoid quinone content, J Clin Microbiol 34:2322, 1996; and Weyant RS, Moss CW, Weaver RE et al, editors: Identification of unusual pathogenic gram-negative aerobic and facultatively anaerobic bacteria, ed 2, Baltimore, 1996, Williams & Wilkins.
Sphingomonas paucimobilis and Similar Organisms
Epidemiology, Spectrum of Disease, and Antimicrobial Therapy
Organism
Epidemiology
Disease Spectrum
Antimicrobial Therapy
Acidovorax facilis
A. facilis is found in soil and has been used as a soil additive to improve plant growth in areas of agriculture and horticulture.
Commonly found in soil. Rarely found in clinical material and not substantiated as a cause of human infections.
No guidelines; little is known about antimicrobial resistance potential.
Disk diffusion testing cannot be performed.
CDC group IIc
CDC group IIe
CDC group IIh
CDC group IIi
CDC groups IIc, IIe, IIh, and IIi are found in soil, plants, foodstuffs, and water, including moist areas in hospitals. Not part of human flora.
Rarely found in clinical material and rarely substantiated as a cause of human infections; have been isolated from blood, eyes, and wounds.
No guidelines; little is known about antimicrobial resistance potential
CDC group O-1
CDC group O-2
CDC group O-3
Epidemiology is unknown.
Rarely found in clinical material and rarely implicated as a cause of human infections. CDC group O-3 has been isolated from bone, blood, lung, and lymph node tissue.
No guidelines; one report indicates susceptibility of CDC group O-3 to aminoglycosides, imipenem, trimethoprim-sulfamethoxazole, and chloramphenicol (however, the breakpoints used were based on those for the Enterobacteriaceae family).
Sphingobacterium mizutaii
S. multivorum
S. spiritivorum
Sphingobacteria are ubiquitous in nature.
Rarely involved in human infections. S. mizutaii has been associated with blood, cerebrospinal fluid, and wound infections; S. multivorum with blood and wound infections; and S. spiritivorum with blood and urine infections.
Literature references report the following susceptibilities:
S. mizutaii—erythromycin, trimethoprim-sulfamethoxazole, and pefloxacin.
S. multivorum—amikacin, gentamicin, aztreonam, cefepime, cefotaxime, ceftazidime, meropenem, piperacillin, piperacillin/tazobactam, and chloramphenicol.
S. spiritivorum—amikacin, gentamicin, aztreonam, cefepime, cefotaxime, chloramphenicol.
Sphingomonas paucimobilis
S. parapaucimobilis
S. paucimobilis inhabits environmental niches and is known especially as a waterborne organism that can exist in hospital water systems. Not part of human flora. Mode of transmission is uncertain but probably involves patient exposure to contaminated medical devices or solutions.
S. paucimobilis virulence factors are unknown. It has been implicated in community- and hospital-acquired infections, specifically in blood and urine infections.
No definitive guidelines; potentially active agents include trimethoprim-sulfamethoxazole, chloramphenicol, ciprofloxacin, and aminoglycosides; resistance to beta-lactams is known, but validated susceptibility testing methods do not exist.
Laboratory Diagnosis
Specimen Collection and Transport
Cultivation
Media of Choice
Colonial Appearance
Organism
Medium
Appearance
Acidovorax facilis
BA
No distinctive appearance
CDC group IIc
BA
No distinctive appearance but colonies sticky
CDC group IIe
BA
No distinctive appearance
CDC group IIh
BA
No distinctive appearance
CDC group IIi
BA
No distinctive appearance
CDC group O-1, O-2, O-3
BA
Yellow pigment present in O-1 and O-2 but not in O-3
Sphingobacterium spp.
BA
Yellow pigment present in S. mizutaii
Sphingomonas paucimobilis
S. parapaucimobilis
BA
Small, circular, smooth, convex; bright yellow growth pigment
Approach to Identification
Organism
Insoluble Pigment
Glucose Oxidized
Xylose Oxidized
Sucrose Oxidized
Esculin Hydrolysis
Motility
Acidovorax facilis
−
+
(+)
−
−
+
CDC group IIc
Tan or buff
+
−
+
+
nm
CDC group IIe
−
+
−
−
−
nm
CDC group IIh
−
+
−
−
+
nm
CDC group IIi
Yellow
+
+
+
+
nm
CDC group O-2
Yellow to orange
v
−
+
v
v*
Sphingobacterium mizutaii
v†
+
(+)
+
+
nm
Sphingomonas spp.‡
Yellow
+
+
+
+
+§
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Sphingomonas paucimobilis and Similar Organisms
