• Uniform round to oval nuclei with finely dispersed chromatin
• Neoplastic cells often have nuclear grooves
Ancillary Tests
• Immunohistochemistry: Nuclear β-catenin, cytoplasmic CD10, loss of membrane E-cadherin, nuclear progesterone receptor
Top Differential Diagnoses
• Pancreatic neuroendocrine tumor
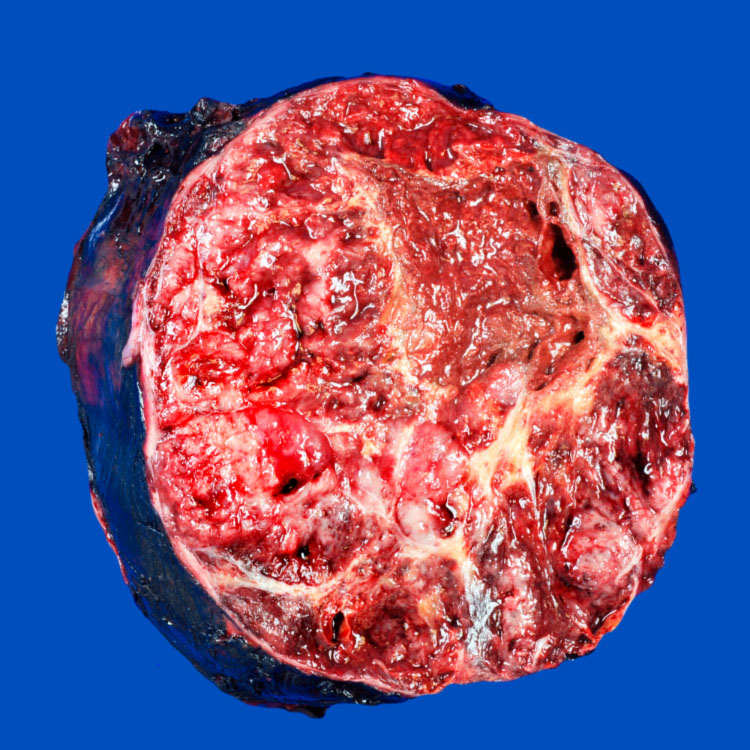
Gross Features This well-demarcated tumor has a soft and friable solid surface with hemorrhagic areas.
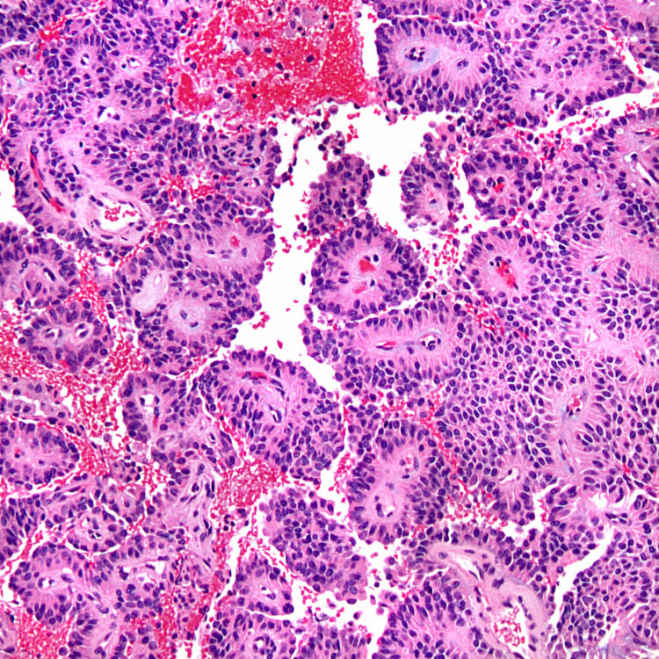
Pseudopapillary Architecture Solid sheets of tumor cells become dyscohesive and result in a characteristic pseudopapillary appearance with a central fibrovascular-like core surrounded by neoplastic cells.
Nuclear Grooves Tumor cells have round to oval nuclei and sometimes exhibit longitudinal nuclear grooves . These intra- and extracytoplasmic eosinophilic hyaline globules stain positive for PASD and α-1-antitrypsin.
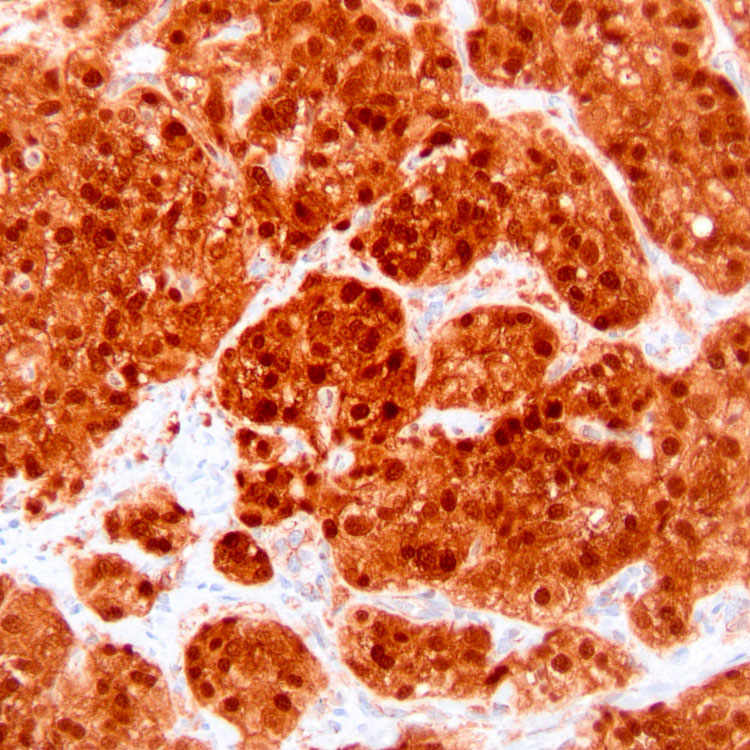
β-catenin Stain Immunohistochemistry for β-catenin shows nuclear and cytoplasmic staining in > 90% of tumors.
TERMINOLOGY
Abbreviations
• Solid-pseudopapillary tumor (SPT)
• Solid-pseudopapillary neoplasm (SPN)
Synonyms
• Solid and papillary epithelial neoplasm
• Solid cystic tumor
• Papillary and cystic neoplasm
• Frantz tumor
Definitions
• Low-grade malignant neoplasm of uncertain cellular differentiation
• Originally described in 1959
ETIOLOGY/PATHOGENESIS
Cellular Lineage
• Uncertain, electron microscopy shows evidence of epithelial differentiation
Molecular
• 90-100% harbor mutations in CTNNB1 gene
CLINICAL ISSUES
Epidemiology
• Incidence
Uncommon (1-2% of all exocrine pancreatic tumors)
• Age
Most patients in 20s and 30s
– Mean age: 25-35 years
– Overall age range: 7-79 years
• Sex
Female predominance (M:F = 1:9-20)
Site
• Evenly distributed throughout pancreas
Presentation
• Nonspecific symptoms related to intraabdominal mass
Vague abdominal pain, weight loss, anorexia
• May have palpable abdominal mass
• Up to 1/3 of cases discovered incidentally
• Complications: Rupture, hemoperitoneum
Laboratory Tests
• Serum oncomarkers, laboratory tests usually normal
Natural History
• Most are indolent, slow-growing, and nonaggressive
• May directly invade stomach, duodenum, spleen
• Metastasis
10-15% of cases
Liver, peritoneum, lymph nodes
– Peritoneal metastases more common in patients with trauma, rupture, or drainage of neoplasm
• Rare, clinically aggressive variant
Treatment
• Surgical resection is treatment of choice
• Can recur if incompletely resected
Prognosis
• Excellent
> 80% cured with surgical resection
10-15% of cases have metastases or recurrence
Even patients with metastases have favorable long-term survival
• No proven morphologic predictors of outcome
Only gold members can continue reading. Log In or Register to continue
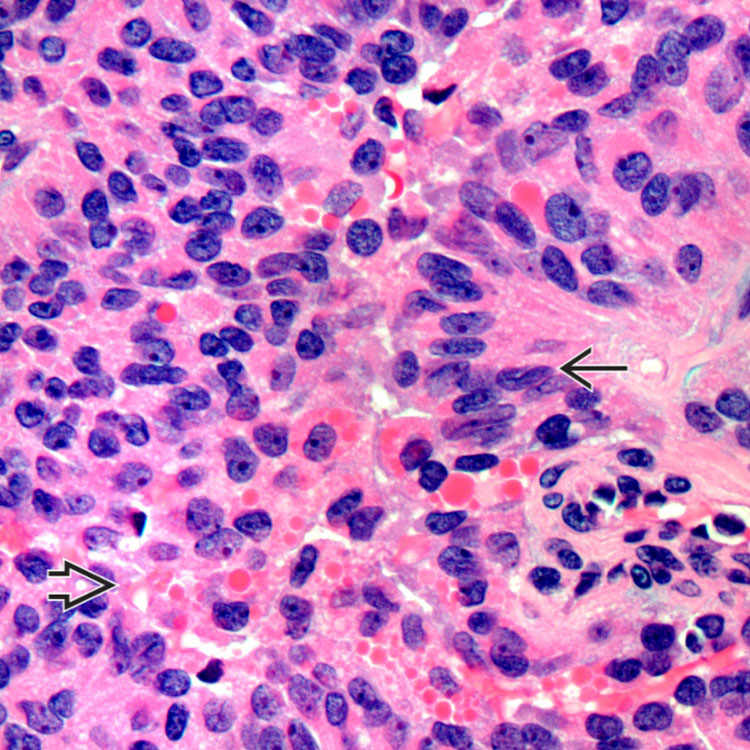
 . These intra- and extracytoplasmic eosinophilic hyaline globules
. These intra- and extracytoplasmic eosinophilic hyaline globules  stain positive for PASD and α-1-antitrypsin.
stain positive for PASD and α-1-antitrypsin.