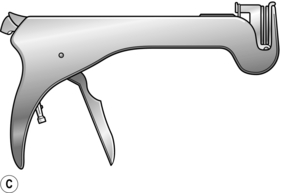
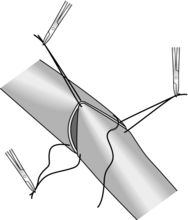
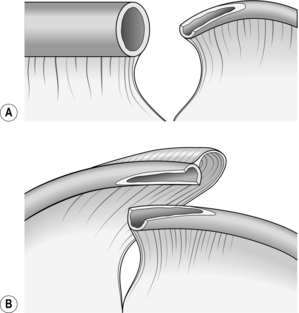
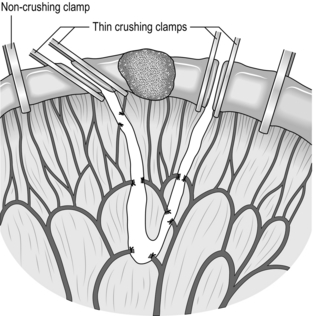
11 1. The duodenum [From Greek: duodekadaktulon = 12 fingers (breadth)] is 25 cm long. Apart from the proximal 2–3 cm, it is retroperitoneal. The remaining small bowel, which has a mesentery, is variable in total length (about 3–5 m) and difficult to measure with accuracy in vivo. It is arbitrarily divided into a proximal 40%, the jejunum (Latin: jejunus = hungry, empty), and a distal 60%, the ileum (Greek: eilios = twisted). On palpation the jejunal wall is thicker than that of the ileum, so that the examining fingers gain the impression of a double layer, rather like feeling a shirt through the sleeve of a jacket. 2. Examine the duodenal loop. Locate the duodenojejunal flexure by displacing the transverse colon upwards and tracing the coils of jejunum proximally to the ligament of Treitz. Pick up the small bowel at the duodenojejunal flexure and feed it through your fingers down to the ileocaecal valve. Note the diameter and contents of the bowel and the thickness and colour of its wall. 3. Examine the small-bowel mesentery throughout. Its thickness varies with the patient’s adiposity. In a thin patient mesenteric lymph nodes can often be seen: determine whether the nodes are enlarged or inflamed. 1. Diverticula. These are common. Meckel’s diverticulum, which arises from the distal ileum, is considered below. Acquired diverticula may affect the duodenum, jejunum and to a lesser extent the ileum, and are frequently multiple. Do not remove incidental diverticula unless they are inflamed, bleeding or appear diseased. 2. Inflammation. Crohn’s disease may affect any part of the alimentary tract but especially the terminal ileum. Affected segments of bowel are inflamed, thickened and narrowed, and often covered with fibrinous exudate. The mesentery is thickened and the mesenteric fat often extends over the serosa of the bowel towards the anti-mesenteric border (fat wrapping). Adjacent lymph nodes are often enlarged. Look for evidence of disease elsewhere in the small and large bowel. Segmental resection is often required for chronic Crohn’s enteritis. Tuberculous and Yersinial infection can produce similar changes of ileitis; if in doubt remove a lymph node for bacteriological and histological examination. Coeliac disease predominantly affects the jejunum. The diagnosis is indicated by dilatation of subserous and mesenteric lymphatics, thinning and pigmentation of the bowel wall and splenic atrophy. Severe refractory coeliac disease may cause ulcerative jejunitis and predispose to small bowel lymphoma.1 Full-thickness biopsy is usually required to make this diagnosis (see below). Small-bowel ulcers and strictures may occur spontaneously, follow radiotherapy or transient strangulation in an external hernia or after the ingestion of potassium tablets. 3. Infarction. The viability of the small bowel must be carefully checked after reduction of a strangulated hernia or untwisting of a volvulus in adhesional obstruction. Any frankly necrotic or perforated loops should be excised. If you are in doubt about the viability of a dusky segment, return it to the abdomen and wait for 5 minutes (timed by the clock). The return of a shiny, pink appearance, pulsation of the mesenteric vessels and peristalsis across the affected segment indicate viability. If doubt persists, resect. 4. Tumours. Serosal deposits occur in carcinomatosis peritonei and may cause kinking and obstruction of the small bowel, requiring side-to-side bypass (see below). Primary neoplasms are less common. Benign tumours such as adenoma, leiomyoma, lipoma and Peutz-Jeghers hamartomas can cause intussusception. Carcinoid tumours favour the ileum, but may be multiple and metastasizing; they are hard with a yellowish cut surface. Other malignant tumours comprise adenocarcinoma, lymphoma and leiomyosarcoma in that order of prevalence. Primary neoplasms should be resected or, if unresectable, bypassed and biopsied. 1. Duodenal lesions can be biopsied endoscopically under direct vision. 2. The small intestine can be examined using flexible endoscopy or capsule endoscopy. Capsule endoscopy is now widely used clinically, complementing other enteroscopic techniques.1 It employs a capsule containing a digital camera with a radio transmitter, an external receiving antenna and a computer workstation for review of images. The technique is increasingly used for the diagnosis of obscure gastrointestinal bleeding, iron-deficiency anaemia and Crohn’s disease.2,3 Biopsy of any identified abnormalities, on the other hand, requires small bowel enteroscopy. 3. Operative biopsy of the small intestine is seldom indicated. It is usually possible to excise the segment of bowel in question, and intestinal biopsy should be avoided in Crohn’s disease. If a full-thickness biopsy is required, however, the incision should be closed in two layers in the same fashion as an intestinal anastomosis. 4. Mesenteric lymph nodes can be biopsied with relative ease, either laparoscopically or at open surgery. Where possible, select a node close to the bowel wall and avoid dissecting deep into the root of the mesentery. Carefully incise the peritoneum and dissect out the entire node, using diathermy to coagulate small blood vessels. 1. Rubio-Tapia A, Murray JA. Classification and management of refractory coeliac disease. Gut 2010;59(4):547–57. 2. Liao Z, Gao R, Xu C, et al. 2010 Indications and detection, completion, and retention rates of small-bowel capsule endoscopy: a systematic review. Gastrointest Endosc 2010;71(2):280–6. 3. Maieron A, Hubner D, Blaha B, et al. Multicenter retrospective evaluation of capsule endoscopy in clinical routine. Endoscopy 2004;36:864–8. 1. Several hundred intestinal anastomoses are carried out each week in Britain, and the vast majority heal rapidly by primary intention. 2. Remember that most of the intestinal tract is contaminated with bacteria. Take appropriate precautions against disseminating faecal organisms before dividing and re-suturing the bowel; clamps are usually indicated to prevent spillage of faeces or small bowel contents. 3. Ensure that the bowel ends are pink and bleeding freely, and leave the mesentery attached to the bowel right up to the point of intestinal transection. If either cut end is bruised or dusky, it is usually sensible to sacrifice a few more centimetres of intestine, even if, in the case of the large bowel, this requires further mobilization. 4. Tension usually results from inadequate mobilization, especially of the colon. Though readily avoidable, twisting of the mesentery can also render an anastomosis ischaemic. Repair mesenteric/mesocolic defects after completing an intestinal anastomosis to prevent postoperative internal herniation, but take care not to compromise the vessels supplying the bowel ends. 5. Distended loops of bowel are heavy and difficult to handle. Moreover, healing is impaired because the bowel wall is somewhat ischaemic. Distended small bowel may be decompressed by milking contents upwards into the reach of the nasogastric tube or by enterotomy and insertion of a sucker (see below). Gaseous distension of the large bowel can be relieved by introducing a needle obliquely through its wall. 1. Traditionally, bowel is united in two layers, using absorbable suture material such as polyglactin 910 (Vicryl) for the inner, all-coats layers and an outer stitch, named after its inventor in 1826, the Parisian surgeon Antoine Lembert (1802–1851), to join the seromuscular layers. More recently, one-layered anastomoses have gained popularity and have proved safe. They are used in colorectal, small bowel and bilio-enteric anastomoses and in oesophago-jejunostomy. 2. Surgeons have long disputed the best suture material, the best type of stitch and the best methods of fashioning a suture line. These technical points are less important than the principle stated above: to achieve accurate and tension-free coaptation of two healthy mucosal surfaces. Nevertheless, each surgeon develops his own variations of technique which he believes to be the most appropriate. As an assistant, therefore, follow the method of your present chief and aim to experience a number of methods before you select one for yourself. 3. Surgical trainees are often uncertain whether to use continuous or interrupted sutures in a given situation. A continuous (running) stitch is undoubtedly quicker and it achieves good haemostasis. It can be used for straightforward gastric, enteric and colonic anastomoses. 4. Interrupted sutures allow greater precision and may be more convenient than a continuous stitch when there is marked disparity in the size of the bowel ends to be united or the anastomosis is technically difficult. In inaccessible situations, such as a colorectal anastomosis deep in the pelvis or hepaticojejunostomy, it may be wise to insert the entire posterior row of interrupted sutures before trying any individual stitch. 5. Many surgeons routinely use two layers of continuous absorbable sutures for gastric and intestinal anastomoses. If impaired healing is anticipated, as in Crohn’s disease, an inner layer of continuous Vicryl and an outer layer of interrupted 2/0 polyester (Ethibond) or similar non-absorbable suture may provide additional security. Non-absorbable sutures are often also used when joining small bowel to the oesophagus, pancreas or rectum. 6. Whichever type of suture and suture material you employ, take care to achieve the correct degree of tension when pulling through and tying the stitch. Insert each stitch separately and invert the bowel edges as the suture is tightened. Once the bowel edge is inverted, prevent the suture material from slipping by getting your assistant to ‘follow’, keeping the tension on the suture already placed. Alternatively, follow for yourself, using the taut suture as a means of steadying the bowel against the thrust of the needle. The objective is a snug, watertight anastomosis. Excessive tension risks strangulating the bowel incorporated in the stitch and perhaps causing subsequent leakage. 7. Do not place the sutures so close to the edge of the bowel that they might tear out or so deep that they turn in an enormous cuff of tissue and narrow the bowel: usually 3–5 mm is about the correct depth of ‘bite’. Be sure that the all-coats suture does in fact incorporate all coats of the bowel wall. The best way to master these important technical points is to assist at, and then perform under supervision, a number of intestinal anastomoses. 8. The seromuscular stitch unites the adjacent bowel walls outside the all-coats stitch. Sometimes the posterior seromuscular layer is inserted before opening the gut, as in side-to-side anastomoses (Fig. 11.1). After the all-coats stitches have been inserted, carry the seromuscular sutures round the ends of the anastomosis and across the front wall, ultimately encircling the anastomosis so that the all-coats stitches can no longer be seen. For end-to-end anastomoses in small and large intestine it may be simpler to complete the all-coats layer before placing any Lembert sutures. Thereafter, the seromuscular layer can be inserted all the way round by rotating the bowel. 9. There are many ways of inserting the all-coats stitch; two popular methods are described here: 1. Stapling devices can be used to carry out most types of gastrointestinal anastomoses. Disposable and angled instruments are available for use in particular circumstances, and the metal staples come in different lengths to accommodate the different tissue thicknesses encountered. For end-to-end anastomosis (e.g. colorectal, oesophagojejunal) a circular stapling gun (Fig. 11.4A) is introduced into the intestinal lumen downstream, brought out through the distal cut end of bowel and then insinuated into the proximal cut end. Choose the largest anvil that will fit comfortably into the proximal lumen. Tightly snug the proximal and distal gut around the central rod using a polypropylene purse-string suture, and then approximate the anvil to the cartridge by closing the instrument. When the gun is fired, a circular double row of titanium staples is inserted and at the same time a complete 5-mm rim of each bowel end (the ‘doughnut’) is resected. Withdraw the machine and check the ‘doughnuts’ to confirm that they are complete and that the anastomosis is perfect. 2. For side-to-side anastomoses a different instrument called a linear stapler/cutter is used. It resembles a pair of scissors (Fig. 11.4B). One ‘blade’ is inserted into each of the two intestinal segments to be united, and the blades are closed. Firing the gun advances a knife, which divides the adjacent surfaces of bowel between three parallel rows of staples. The resulting opening can then either be sutured or stapled closed using a further staple cartridge. KEY POINTS Stapled anastomosis 3. Stapling devices reduce the time involved in creating an anastomosis and are used extensively in laparoscopic bariatric and oesophago-gastric surgery. 1. This is the simplest way of restoring intestinal continuity after partial enterectomy where there is little or no size disparity. After removal of the resected specimen, clean and approximate the bowel ends. The anastomosis is usually created in one layer, using interrupted absorbable sutures (e.g. 2/0 or 3/0 Vicryl). Interrupted sero–muscular suture. Insert three stay sutures from out to in and in to out evenly spaced around the bowel circumference. Clip the ends and get your assistant to hold the clips to exert traction on the cut edges of bowel. This causes the bowel lumen to adopt a triangular appearance (Fig. 11.5). Between two of the stay sutures, held taught, insert a row of sutures 2–3 mm apart, taking serosa and muscularis only and tying the knots on the serosal surface. 2. Now rotate the anastomosis using the stays and place a further row of sutures between the next adjacent stay sutures. Finally turn the anastomosis over and suture the third side of the triangle. All knots should lie uniformly on the outside of the anastomosis. 1. When the ends of bowel are disproportionate in size, they may be matched by incising the antimesenteric border of the narrow bowel longitudinally (Fig. 11.6A). 2. This manoeuvre is useful in joining obstructed bowel to collapsed bowel or ileum to colon. In neonates with congenital intestinal atresia, the lumen of the distal bowel is particularly narrow and this type of ‘end-to-back’ anastomosis is necessitated. When two segments of narrow intestine must be united, they may both be opened along their antimesenteric borders, which are then joined back-to-back (Fig. 11.6B). The mesenteries are now on opposite sides of the anastomosis and cannot always be neatly approximated. 1. This is most commonly used when creating a Roux-en-Y anastomosis. Approximate the cut end to the side of bowel to which it will be joined and insert a posterior seromuscular suture (Fig. 11.7). 2. Incise the antimesenteric border of the side of bowel to accommodate the cut end. Insert the all-coats stitch as before, remove the clamps and complete the seromuscular stitch. Lastly, join the cut edge of mesentery to the side of the intact mesentery. 1. This can be used to joint two loops of bowel without resection, or to unite intestine to stomach, bile duct, etc. (Fig. 11.8). 2. It may also be employed as an alternative to end-to-end anastomosis after intestinal resection, in which case the cut ends of bowel should first be closed and invaginated. The advantages of the side-to-side anastomosis are that the segments of bowel to be united have no interruption to their blood supply at all and that the incisions can be made exactly congruous. The disadvantages are that there are more suture lines involved and that there may be some degree of stasis and bacterial overgrowth. 3. Lay the segments to be joined side by side in contact for 8–10 cm and insert a posterior seromuscular stitch. Incise the antimesenteric borders for about 5 cm and insert an all-coats stitch. Remove the clamps and complete the anterior seromuscular layer of stitches. When side-to-side anastomosis follows bowel resection, suture the cut edge of mesentery to the adjacent intact mesentery on each side of the anastomosis. 1. Resection is often indicated for congenital lesions of the small bowel such as atresia and duplication; traumatic perforation; critical ischaemia from mesenteric trauma, strangulation or arteriosclerosis; Crohn’s disease or other cause of stricture; tumours of the bowel or its mesentery. Resection is sometimes indicated for fistula, diverticulitis, intussusception and a symptomatic blind loop. Small portions of the duodenum and ileum are removed during partial gastrectomy and right hemicolectomy respectively. 2. There are several reasons for being conservative in the management of Crohn’s disease: the indolent nature of the disease, its relapsing course and its strong tendency (> 50%) to recur anywhere in the intestinal tract, but especially at and just proximal to the anastomosis. Despite many advances in the treatment of Crohn’s disease, the course of the disease in any given patient remains unpredictable. A multivariate analysis has shown that the only independent predictors of earlier postoperative recurrence after initial operation are an initial presentation with peritonitis secondary to perforation, and a longer preoperative disease duration.1 3. On the other hand, most patients with chronic Crohn’s enteritis eventually require resection of the affected segment because of subacute obstruction, fistula or abscess. Bypass is obsolete: although it may achieve remission of active disease in the defunctioned segment, bacterial overgrowth of the blind loop may aggravate diarrhoea and there is a long-term risk of carcinoma. For short stenotic areas of bowel strictureplasty (see below) is an alternative to resection. 4. When operating for radiation enteropathy, establish the extent both of the original cancer and of the radiation damage. Where possible, avoid bypass or exclusion procedures: the defunctioned bowel may still give rise to problems such as bleeding and fistula. Wide resection is the optimal approach, ensuring that at least one side of the subsequent anastomosis employs healthy, non-irradiated, bowel. 1. In the presence of an obstructing lesion, ensure that the patient is adequately resuscitated before operation with nasogastric intubation and intravenous rehydration. 2. Healthy ileum has a resident bacterial flora, and in the presence of obstruction the entire small bowel may be colonized. It is sensible to employ appropriate prophylactic antibiotic cover, such as a cephalosporin plus metronidazole given preoperatively in a single injection, in all operations likely to involve intestinal resection. 3. Nutritional status may be impaired in some patients requiring small-bowel resection, for example those with Crohn’s disease, cancer, radiation enteropathy or enterocutaneous fistula. In the absence or obstruction or fistula, supplemental enteric feeds may reverse the nutritional defect, but some patients require a period of preoperative parenteral nutrition. 1. Employ a midline incision that skirts the umbilicus and can be extended in either direction as necessary. 2. Remember that the small bowel quite often adheres to the back of a previous laparotomy incision, so take particular care during abdominal re-entry. An accidental perforation is unlikely to be located in a segment of bowel you intended to remove. 1. Expose and examine the entire small bowel. Continue by examining the stomach, large bowel and remaining abdominal viscera. 2. If a loop of small bowel has been strangulated in an external hernia, release the obstruction and check the viability of the bowel after allowing a period of 5 minutes for possible recovery in doubtful cases. 3. Do not gratuitously sacrifice healthy bowel, particularly terminal ileum which has specialized transport functions. Except when operating for primary malignant tumours it is quite unnecessary to excise a deep wedge of mesentery, which might increase the extent of small bowel requiring removal. In Crohn’s disease do not remove more than a few centimetres of gut on either side of the affected segment, but include any fistulas or sinuses. It is more than likely that further resection will be required in future, and microscopic inflammation of the bowel at the resection margin does not appear to increase subsequent anastomotic recurrence. Formal right hemicolectomy is unnecessary for Crohn’s disease of the terminal ileum; undertake a limited ileocaecal resection. 4. Sometimes a partial resection of small bowel can be performed, leaving the mesentery intact. Appropriate conditions include Richter’s hernia, Meckel’s diverticulum and small benign tumours arising on the antimesenteric border. 1. Determine the proximal and distal sites for dividing the bowel, and select the line of vascular section in between; keep close to the bowel wall (Fig. 11.9) except when resecting a neoplasm (Fig. 11.10). Incise the peritoneum along this line on each aspect of the mesentery. This manoeuvre is most easily accomplished by inserting one blade of a pair of fine, curved scissors beneath the peritoneum and cutting superficially to expose the mesenteric vessels. Fig. 11.10 Resection of a small-bowel tumour. A deeper wedge of mesentery is included than in operations for benign disease (see Fig. 11.9). As before, the narrower segment of bowel (on the left) is transected obliquely, removing more of the mesenteric border with the specimen. 2. Using small artery forceps, create a small mesenteric window right next to the bowel wall at each point chosen for intestinal transection. Starting at one end, insinuate a curved artery forceps through this window and back through the mesentery, denuded of peritoneum, 1–2 cm away, thus isolating a small leash of mesentery with its contained vessels. Divide the vessels between artery forceps, ligating the mesentery beneath each pair of forceps using 2/0 or 3/0 Vicryl ties, according to the thickness of the mesentery. Proceeding in this manner, divide the mesentery right up to the bowel wall at the further end of the line of peritoneal incision. Take care in placing and tying each ligature: if the knot slips, there can be troublesome haemorrhage. 3. Apply four intestinal clamps (Fig. 11.9). The first two clamps are crushing clamps (Payr’s, Lang Stevenson’s or Pringle’s). They should be applied obliquely at the points of intended intestinal transection, so that slightly more of the antimesenteric border is resected than of the mesenteric border; the obliquity reduces the risk of a tight anastomosis. Now apply a non-crushing clamp about 5 cm outside each crushing clamp, having milked the intervening bowel free of contents. 4. Place a clean gauze swab beneath the clamps at each end to catch spills, and divide the bowel with a knife flush against the outer aspect of each crushing clamp. Place the specimen and the soiled knife in a separate dish, which is then removed. 5. Cleanse each bowel end, using small swabs or pledgets of gauze soaked in 10% povidone-iodine. Then remove the protective gauze swab and proceed to intestinal anastomosis. In an attempt to limit contamination, some surgeons divide the intestine between two pairs of light crushing clamps (i.e. six clamps in all) and insert the posterior seromuscular layer of sutures before removing the outer clamps and excising the narrow rim of crushed tissue (Fig. 11.10). 6. Perform a single-layer, end-to-end anastomosis, as described in the previous section. 1. A diverticulum on the antimesenteric border may be locally excised. Clamp and cut it off at the neck, then close the defect in two layers as a transverse linear slit. Try to avoid narrowing the intestinal lumen during this procedure. 2. A diamond-shaped area of the antimesenteric border may be included in the resection of a localized tumour or wide-mouthed Meckel’s diverticulum. Apply two light crushing clamps (Lang Stevenson’s or Pringle’s) across the antimesenteric border, meeting in a ‘V’ (Fig. 11.11). Incise the bowel flush with the outer aspect of each clamp, and close the wall in two layers, leaving a transverse suture line.
Small bowel and operations for obesity
EXAMINATION OF THE SMALL BOWEL
Normal appearance
Abnormalities
Biopsy
REFERENCES
INTESTINAL ANASTOMOSIS
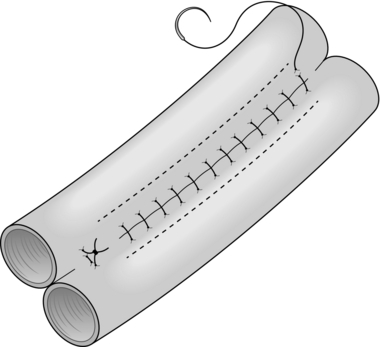
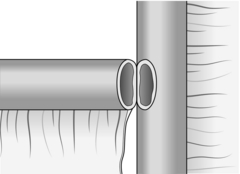
General principles
Hand-suturing techniques
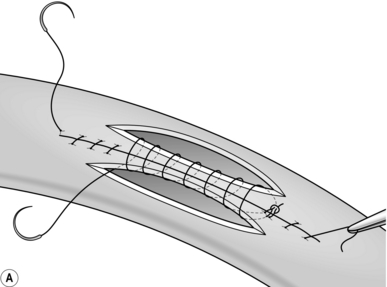
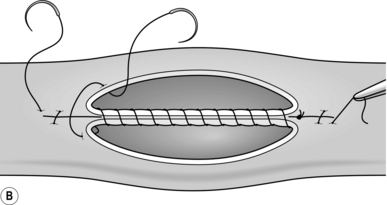
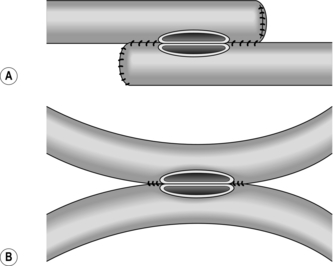
 Continuous over–and–over suture. Approximate the two edges of cut bowel. Starting at one end, insert a corner stitch from outside to in, then over the adjacent edges of bowel and out through the other corner. Tie the suture and clip the short end. Pass the stitch back through the nearest bowel wall, over the contiguous cut edges and back through the full thickness of both walls. Continue over-and-over stitches to the opposite corner (Fig. 11.2A). After the last stitch is inserted right into the corner, take it back through the nearest corner leaving a loop on the mucosa so that the stitch emerges from the outer wall of the bowel (Fig. 11.2B). Now sew the front walls together by passing the stitch over and over, from out to in and then from in to out (Fig. 11.2C). Continue until the anastomosis has been encircled and the edges inverted, then tie off the ends of suture material. This over-and-over stitch is haemostatic.
Continuous over–and–over suture. Approximate the two edges of cut bowel. Starting at one end, insert a corner stitch from outside to in, then over the adjacent edges of bowel and out through the other corner. Tie the suture and clip the short end. Pass the stitch back through the nearest bowel wall, over the contiguous cut edges and back through the full thickness of both walls. Continue over-and-over stitches to the opposite corner (Fig. 11.2A). After the last stitch is inserted right into the corner, take it back through the nearest corner leaving a loop on the mucosa so that the stitch emerges from the outer wall of the bowel (Fig. 11.2B). Now sew the front walls together by passing the stitch over and over, from out to in and then from in to out (Fig. 11.2C). Continue until the anastomosis has been encircled and the edges inverted, then tie off the ends of suture material. This over-and-over stitch is haemostatic.
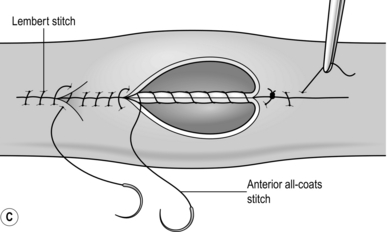
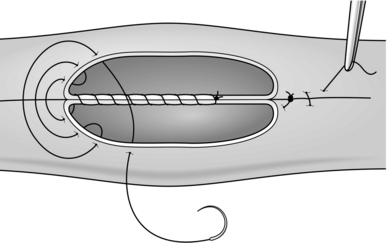
 Continuous over–and–over plus Connell suture. Commence in the middle of the posterior wall by placing a stitch between the adjacent cut edges of bowel and tying it on the luminal surface. Now continue towards one corner with over-and-over stitches. At the corner the needle passes from in to out on the nearside cut surface, then crosses to the far edge and is passed in and out to leave a loop on the mucosa (Fig. 11.3). The needle returns to the near edge and another loop-on-the-mucosa stitch (named after the American surgeon Gregory Connell born 1875, who popularized it) is inserted. These Connell stitches turn the corner neatly. Once you are round the corner, leave this stitch and return to the middle of the posterior wall. Use a new length of suture material, unless there is a needle at each end of the original length. Insert and tie a stitch close to the site of the original knot, and proceed towards the opposite corner, using Connell sutures to negotiate the corner again. Once round the corner, return to over-and-over stitches. Tie the ends of suture material together where they meet in the middle of the anterior wall.
Continuous over–and–over plus Connell suture. Commence in the middle of the posterior wall by placing a stitch between the adjacent cut edges of bowel and tying it on the luminal surface. Now continue towards one corner with over-and-over stitches. At the corner the needle passes from in to out on the nearside cut surface, then crosses to the far edge and is passed in and out to leave a loop on the mucosa (Fig. 11.3). The needle returns to the near edge and another loop-on-the-mucosa stitch (named after the American surgeon Gregory Connell born 1875, who popularized it) is inserted. These Connell stitches turn the corner neatly. Once you are round the corner, leave this stitch and return to the middle of the posterior wall. Use a new length of suture material, unless there is a needle at each end of the original length. Insert and tie a stitch close to the site of the original knot, and proceed towards the opposite corner, using Connell sutures to negotiate the corner again. Once round the corner, return to over-and-over stitches. Tie the ends of suture material together where they meet in the middle of the anterior wall.
Mechanical stapling techniques
Types of anastomosis
End-to-end anastomosis
Oblique anastomosis
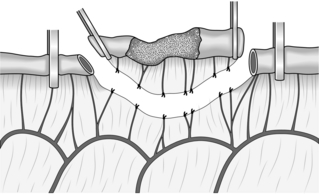
End-to-side anastomosis
Side-to-side anastomosis
ENTERECTOMY (SMALL-BOWEL RESECTION)
Appraise
Prepare
Access
Assess
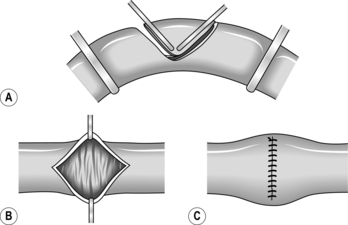
Standard resection
Partial resection
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree