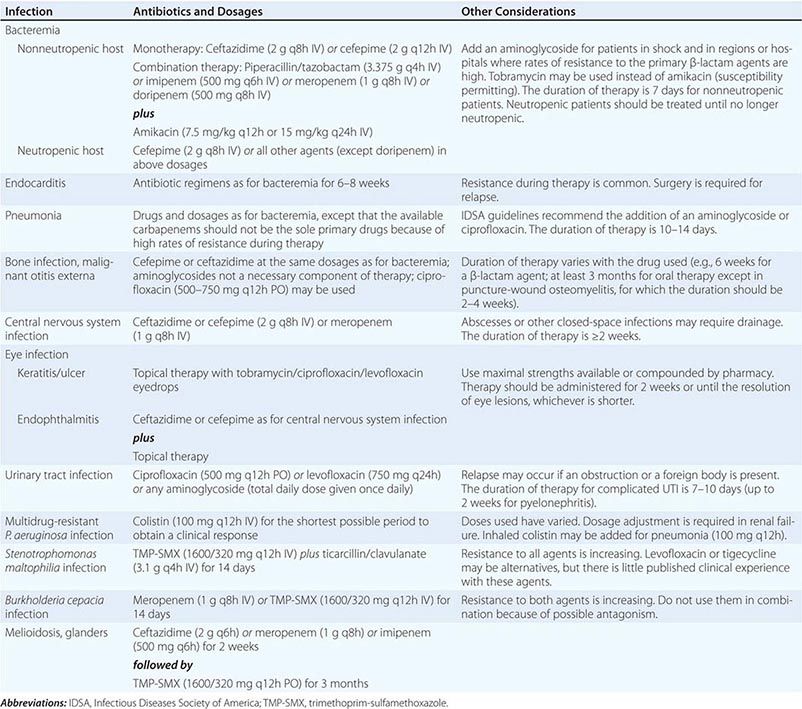
Morganella and Providencia may be extensively resistant to antibiotics. Most isolates are resistant to ampicillin, first-generation cephalosporins, nitrofurantoin, fosfomycin, tigecycline, and the polymyxins; 40% are resistant to fluoroquinolones. Morganella and Providencia possess inducible AmpC β-lactamases; clinically significant induction or selection of stably derepressed mutants may develop during therapy. Resistance to antipseudomonal penicillins, aztreonam, gentamicin, TMP-SMX, and second- and third-generation cephalosporins is emerging but is still variably prevalent. The β-lactamase inhibitor tazobactam increases susceptibility to β-lactam agents, but sulbactam and clavulanic acid do not. Carbapenems, amikacin, and cefepime are the most active agents (>90% of isolates susceptible); however, resistance to the carbapenems, when present, is a concern because of the inherent resistance of Morganella and Providencia to the polymyxins and tigecycline. Removal of a colonized catheter or stone is critical for eradication of UTI.
EDWARDSIELLA INFECTIONS
![]() E. tarda is the only member of the genus Edwardsiella that is associated with human disease. This organism is found predominantly in freshwater and marine environments and in the associated aquatic animal species. Human acquisition occurs primarily during interaction with these reservoirs and ingestion of inadequately cooked aquatic animals. E. tarda infection is rare in the United States; recently reported cases are mostly from Southeast Asia. This pathogen shares clinical features with Salmonella species (as an intestinal pathogen; Chap. 190), Vibrio vulnificus (as an extraintestinal pathogen; Chap. 193) and Aeromonas hydrophila (as both an intestinal and extraintestinal pathogen; Chap. 183e).
E. tarda is the only member of the genus Edwardsiella that is associated with human disease. This organism is found predominantly in freshwater and marine environments and in the associated aquatic animal species. Human acquisition occurs primarily during interaction with these reservoirs and ingestion of inadequately cooked aquatic animals. E. tarda infection is rare in the United States; recently reported cases are mostly from Southeast Asia. This pathogen shares clinical features with Salmonella species (as an intestinal pathogen; Chap. 190), Vibrio vulnificus (as an extraintestinal pathogen; Chap. 193) and Aeromonas hydrophila (as both an intestinal and extraintestinal pathogen; Chap. 183e).
INFECTIOUS SYNDROMES
Gastroenteritis is the predominant infectious syndrome (50–80% of infections). Self-limiting watery diarrhea is most common, but severe colitis also occurs. The most common extraintestinal infection is wound infection due to direct inoculation, which is often associated with freshwater, marine, or snake-related injuries. Other infectious syndromes result from invasion of the gastrointestinal tract and subsequent bacteremia. Most afflicted hosts have comorbidities (e.g., hepatobiliary disease, iron overload, cancer, or diabetes mellitus). A primary bacteremic syndrome, sometimes complicated by meningitis, has a 40% case-fatality rate. Visceral (primarily hepatic) and intraperitoneal abscesses also occur. Endocarditis and empyema have been described.
DIAGNOSIS
Although E. tarda can readily be isolated and identified, most laboratories do not routinely seek to identify it in stool samples. Production of hydrogen sulfide is a characteristic biochemical property.
TREATMENT | EDWARDSIELLA INFECTIONS |
E. tarda is susceptible to most antimicrobial agents appropriate for use against GNB. Gastroenteritis is generally self-limiting, but treatment with a fluoroquinolone may hasten resolution. In the setting of severe sepsis, fluoroquinolones, third- and fourth-generation cephalosporins, carbapenems, and amikacin—either alone or in combination—are the safest choices pending susceptibility data.
INFECTIONS CAUSED BY MISCELLANEOUS GENERA
Species of Hafnia, Kluyvera, Cedecea, Pantoea, Ewingella, Leclercia, and Photorhabdus are occasionally isolated from diverse clinical specimens, including blood, sputum, urine, cerebrospinal fluid, joint fluid, bile, and wounds. These organisms are rare and usually cause infection in a compromised host or in the setting of an invasive procedure or a foreign body. Cephalosporinases from Kluyvera have been implicated as the progenitors of CTX-M ESBLs.
187 | Acinetobacter Infections |
Infections with bacteria of the genus Acinetobacter are established as a significant problem worldwide. Acinetobacter baumannii is particularly formidable because of its propensity to acquire antibiotic resistance determinants. Endemic infections caused by strains of A. baumannii resistant to multiple antibiotic classes, including carbapenems, are a serious concern in many specialized hospital units, especially intensive care units (ICUs). The foremost implication of infection with carbapenem-resistant A. baumannii is the need to use “last-line” antibiotics such as colistin, polymyxin B, or tigecycline; these options have the potential to render these bacteria resistant to all available antibiotics.
DEFINITION
Acinetobacter species are oxidase-negative, nonfermenting, short, gram-negative bacilli. They were traditionally thought of as nonmotile—a characteristic from which the genus name was derived (from the Greek akineto, meaning “nonmotile”). However, recent work has shown that Acinetobacter organisms demonstrate motility under certain growth conditions. The bacteria grow well at 37°C in aerobic conditions on a range of laboratory media (e.g., blood agar). Some species may not grow on MacConkey agar. Differentiation of Acinetobacter species is difficult with the means typically available to most clinical microbiology laboratories, including commercial semiautomated identification systems. The commonly used matrix-assisted laser desorption ionization–time of flight mass spectrometry (MALDI-TOF MS) systems are undergoing evaluation for species-level identification of Acinetobacter. DNA–DNA hybridization is a method used for speciation in reference laboratories. Naturally occurring oxacillinase genes (blaOXA) have been identified in several Acinetobacter species, and their detection by polymerase chain reaction can aid in species identification.
ETIOLOGY
Widely distributed in nature, Acinetobacter species can be found in water, in soil, and on vegetables. Acinetobacter is a component of the human skin flora and is sometimes identified as a contaminant in blood samples collected for culture. Fecal carriage can be detected in both healthy and hospitalized individuals. However, despite the ubiquity of some Acinetobacter species, the natural habitat of the most clinically important species, A. baumannii, remains to be fully defined.
EPIDEMIOLOGY
![]() A. baumannii infections have been diagnosed in patients on all inhabited continents. The vast majority of infections occur in hospitalized patients and other patients with significant health-care contact. Outbreaks of carbapenem-resistant A. baumannii are particularly problematic. A significant issue is the introduction of carbapenem-resistant A. baumannii into hospitals as a result of medical transfers, especially from hospitals where the organism is highly endemic.
A. baumannii infections have been diagnosed in patients on all inhabited continents. The vast majority of infections occur in hospitalized patients and other patients with significant health-care contact. Outbreaks of carbapenem-resistant A. baumannii are particularly problematic. A significant issue is the introduction of carbapenem-resistant A. baumannii into hospitals as a result of medical transfers, especially from hospitals where the organism is highly endemic.
The Americas In 1991 and 1992, outbreaks of carbapenem-resistant A. baumannii infection occurred in a hospital in New York City. Subsequently, numerous other hospitals in the United States and South America have had outbreaks of carbapenem-resistant A. baumannii. Infections with A. baumannii among military personnel from the United States and Canada injured in Iraq or Afghanistan were widely observed beginning in 2002. Acinetobacter was one of the most common causes of bloodstream infections and bone and soft tissue infections after war-related injury. An epidemiologic investigation revealed that A. baumannii could be grown from environmental sites in field hospitals and that the environmental strains were closely related genotypically to clinical isolates.
Europe A. baumannii infections have posed a substantial clinical challenge in many parts of Europe since the early 1980s. Three clones (European clones I, II, and III) have been the predominant causes of A. baumannii infection in hospitals in Europe. Carbapenem resistance in A. baumannii is a significant issue in many European countries, most notably the United Kingdom, Greece, Italy, Spain, and Turkey.
Asia, Australia, the Middle East, and Africa Although surveillance data are sparse from many countries in these regions, problems with carbapenem-resistant A. baumannii abound. Community-acquired infections are well described in northern Australia and some parts of Asia. These infections may be more likely in men >45 years of age who have histories of cigarette smoking, alcoholism, diabetes mellitus, or chronic obstructive airway disease. Community-acquired strains are more susceptible to antimicrobial agents than are hospital-acquired strains, but the clinical presentation of community-acquired disease is quite distinct and is characterized by overwhelming infection with severe pneumonia, septic shock, and multiorgan failure.
PATHOGENESIS
A. baumannii colonizes patients exposed to heavily contaminated hospital environments or to the hands of health care workers in these locations. Emerging data suggest that the organism can be found in the air in rooms of patients infected with Acinetobacter. Colonization of the upper airways in mechanically ventilated patients may lead to nosocomial pneumonia. Colonization of the skin may lead to central line–associated bloodstream infection, catheter-associated urinary tract infection (UTI), wound infection, or postneurosurgical meningitis. Throat carriage and microaspiration may be involved in the pathogenesis of community-acquired pneumonia due to A. baumannii.
Much less is known about the virulence mechanisms of and host responses to A. baumannii than about these aspects of other pathogenic gram-negative bacteria. Because of the emergence of multidrug-resistant strains, including those resistant to all available antibiotics, the impetus to study A. baumannii pathogenesis has grown. Novel targets for antibacterial drug development are desperately required, and drugs that have antivirulence mechanisms may provide new therapeutic options. Specific virulence mechanisms in A. baumannii include iron acquisition and transport systems; outer-membrane protein A (OmpA), which mediates mammalian cell adhesion, invasion, and cytotoxicity through mitochondrial damage and initiation of caspase-dependent apoptosis; lipopolysaccharide (LPS); and proteins important in the formation of biofilm on abiotic and biotic surfaces. Biofilm formation on abiotic surfaces is dependent on a pilus assembly system, which in turn is controlled by a traditional two-component regulatory system mediated by bfmR. Also important in biofilm formation are a gene that encodes a biofilm-associated protein (Bap); OmpA; the quorum-sensing gene abaI, which controls the secretion of 3-hydroxy-C12-homoserine lactone; and the pga locus, which is essential for the production of the polysaccharide poly-β-1,6-N-acetylglucosamine. Most recently, a global virulence regulator known as GacSA was described as important in regulating A. baumannii biofilms, motility, growth in human serum, and virulence in a mammalian infection model.
New model systems for the study of A. baumannii infection, including both nonmammalian (invertebrate) and mammalian models, have been described. Furthermore, the use of A. baumannii transposon-generated mutant libraries to screen for mutants with attenuated growth in human biologic fluids (serum and ascites fluid) has allowed the identification of new virulence mechanisms. These include phospholipase D; capsule production mediated by ptk and epsA; penicillin-binding protein 7/8 encoded by the pbpG gene; and a glycosyltransferase important for LPS biosynthesis encoded by the lpsB gene.
The LPS of A. baumannii appears to play a significant role in eliciting host responses. In studies with knockout mice, Toll-like receptor 4 and CD14 were shown to be important in host recognition, signaling, and cytokine production in response to A. baumannii. Humoral responses targeting iron-regulated outer-membrane proteins and the O-polysaccharide component of LPS also have been described.
CLINICAL MANIFESTATIONS
Pneumonia It may be difficult to distinguish between upper-airway colonization with A. baumannii and hospital-acquired pneumonia. An estimated 5–10% of cases of ventilator-associated pneumonia are due to A. baumannii, although much regional variation exists. Typically, patients with A. baumannii ventilator-associated pneumonia have had a prolonged stay in an ICU; in outbreak situations, however, patients may acquire the infection within days of arrival in an ICU.
![]() Community-acquired pneumonia due to A. baumannii has been described in tropical regions of Australia and Asia. The disease typically occurs during the “wet” season among people with a history of alcohol abuse. Infection may result in fulminant pneumonia requiring admission to an ICU, with a mortality rate of ~50%.
Community-acquired pneumonia due to A. baumannii has been described in tropical regions of Australia and Asia. The disease typically occurs during the “wet” season among people with a history of alcohol abuse. Infection may result in fulminant pneumonia requiring admission to an ICU, with a mortality rate of ~50%.
Bloodstream Infection Although A. baumannii accounts for only ~1–2% of nosocomial bloodstream infections, crude mortality rates from these infections may be as high as 40%. Sources of bloodstream infection are typically a central line or underlying pneumonia, UTI, or wound infection.
Traumatic Battlefield and Other Wounds A. baumannii is a well-known pathogen in burn units. This organism is commonly isolated from wounds of combat casualties; it was the most commonly isolated organism in one assessment of combat victims with open tibial fractures but did not appear to contribute directly to persistent nonunion or the need for amputation.
Meningitis A. baumannii may cause meningitis following neurosurgical procedures. Patients typically have an external ventricular drain in situ.
Urinary Tract Infection A. baumannii is an occasional cause of catheter-associated UTI. It is highly unusual for this organism to cause uncomplicated UTI in healthy women.
Other Clinical Manifestations A small number of case reports describe Acinetobacter prosthetic-valve endocarditis and endophthalmitis/keratitis. The latter is sometimes related to contact lens use or eye surgery.
DIAGNOSIS
Acinetobacter infection should be suspected when plump coccobacilli are seen in Gram’s-stained respiratory tract secretions, blood cultures, or cerebrospinal fluid. Sometimes the organisms are difficult to de-stain. Given their small size, they may be misidentified as either gram-negative or gram-positive cocci.
TREATMENT | ACINETOBACTER INFECTION (TABLE 187-1) |
TREATMENT OPTIONS FOR ACINETOBACTER INFECTIONS |
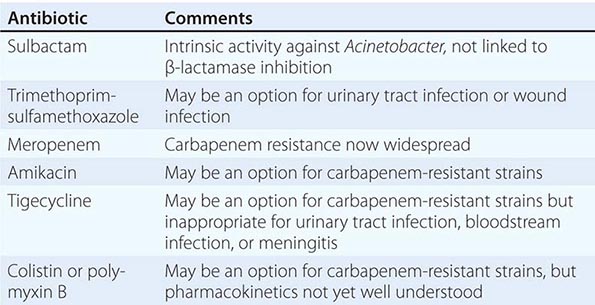
Treatment is hampered by the remarkable ability of A. baumannii to upregulate or acquire antibiotic resistance determinants. The most prominent example is that of β-lactamases, including those capable of inactivating carbapenems, cephalosporins, and penicillins. These enzymes, which include the OXA-type β-lactamases (e.g., OXA-23), the metallo-β-lactamases (e.g., NDM), and rarely KPC-type carbapenemases, are typically resistant to currently available β-lactamase inhibitors such as clavulanate or tazobactam. Plasmids that harbor genes encoding these β-lactamases may also harbor genes encoding resistance to aminoglycosides and sulfur antibiotics. The end result is that carbapenem-resistant A. baumannii may become truly multidrug resistant.
Selection of empirical antibiotic therapy when A. baumannii is suspected is challenging and must rely on a knowledge of local epidemiology. Receipt of prompt, effective antibiotic therapy is the goal. Given the diversity of resistance mechanisms in A. baumannii, definitive therapy should be based on the results of antimicrobial susceptibility testing. Carbapenems (imipenem, meropenem, and doripenem but not ertapenem) have long been thought of as the agents of choice for serious A. baumannii infections. However, the clinical utility of carbapenems is now widely jeopardized by the production of carbapenemases, as described above. Sulbactam may be an alternative to carbapenems. Unlike other β-lactamase inhibitors (e.g., clavulanic acid and tazobactam), sulbactam has intrinsic activity against Acinetobacter; this activity is mediated by the drug’s binding to penicillin-binding protein 2 rather than by its ability to inhibit β-lactamases. Sulbactam is commercially available in a combined formulation with either ampicillin or cefoperazone and may also be available as a single agent in some countries. Despite the absence of randomized clinical trials, sulbactam seems to be equivalent to carbapenems in clinical effectiveness against susceptible strains.
Therapy for carbapenem-resistant A. baumannii is particularly problematic. The only currently available choices are polymyxins (colistin and polymyxin B) and tigecycline. Neither option is perfect. Polymyxins may be nephrotoxic and neurotoxic. Definition of the optimal dose and schedule for administration of polymyxins to patients in vulnerable groups (e.g., those requiring renal replacement therapy) remains challenging, and emergence of resistance in association with monotherapy is a concern. Conventional doses of tigecycline may not result in serum concentrations adequate to treat bloodstream infections. Resistance of A. baumannii to tigecycline may develop during treatment with this drug.
As a consequence of these issues with the polymyxins and tigecycline, combination therapy is now favored for carbapenem-resistant Acinetobacter. However, in a randomized controlled trial, 30-day mortality was not reduced by the addition of rifampin to colistin. Nevertheless, a significant increase in microbiologic eradication was observed in the colistin plus rifampin arm over that attained with colistin alone. Combinations of polymyxins with a carbapenem look more promising and are being evaluated in prospective clinical trials. Fosfomycin has poor activity against Acinetobacter and should not be relied upon for treatment. Clearly, new treatment options are needed for serious Acinetobacter infections.
COMPLICATIONS AND PROGNOSIS
Given the propensity of A. baumannii to cause infections in seriously ill patients in ICUs, it is not surprising that A. baumannii infections are associated with high mortality rates. Thus a pertinent question is whether A. baumannii infections are associated with high attributable mortality rates after the severity of illness is controlled for. A number of studies have addressed this issue but have had disparate results. Whether the discrepant results can be explained purely by methodologic differences is unknown at present.
PREVENTION
Multidrug-resistant A. baumannii clearly causes outbreaks of infection and then establishes endemicity. In endemic situations, a small number of strain types predominate. In the 1991–1992 outbreaks in New York City, for example, two strain types accounted for more than 80% of carbapenem-resistant isolates. This “oligoclonality” plainly demonstrates the potential importance of infection control interventions in response to outbreaks of multidrug-resistant A. baumannii infection.
The hospital environment is an important reservoir of organisms capable of colonizing patients and causing infection. Environmental sources of A. baumannii include computer keyboards, glucometers, multidose medication vials, IV nutrition, inadequately sterilized reusable arterial pressure transducers, ventilator tubing, suction catheters, humidifiers, containers of distilled water, urine collection jugs, and moist bedding articles. Pulsatile-lavage wound treatment—a high-pressure irrigation system used to debride wounds—has been associated with an outbreak of A. baumannii infection.
Contaminated inanimate objects should be removed from the patient-care environment or subjected to enhanced environmental cleaning. Although contact-isolation procedures (use of gloves and gowns when dealing with colonized patients or their environment), accommodation of patients in single rooms, and improved hand hygiene are critical, attention to the patient-care environment may be the only measure that leads to control of outbreaks of A. baumannii infection. One study found that Acinetobacter can be cultured from the air in rooms of patients with A. baumannii infection; the infection-control implications are not yet clear.
188 | Helicobacter pylori Infections |
DEFINITION
![]() Helicobacter pylori colonizes the stomach in ~50% of the world’s human population, essentially for life unless eradicated by antibiotic treatment. Colonization with this organism is the main risk factor for peptic ulceration (Chap. 348) as well as for gastric adenocarcinoma and gastric mucosa-associated lymphoid tissue (MALT) lymphoma (Chap. 109). Treatment for H. pylori has revolutionized the management of peptic ulcer disease, providing a permanent cure in most cases. Such treatment also represents first-line therapy for patients with low-grade gastric MALT lymphoma. Treatment of H. pylori is of no benefit in the treatment of gastric adenocarcinoma, but prevention of H. pylori colonization could potentially prevent gastric malignancy and peptic ulceration. In contrast, increasing evidence indicates that lifelong H. pylori colonization may offer some protection against complications of gastroesophageal reflux disease (GERD), including esophageal adenocarcinoma. Recent research has focused on whether H. pylori colonization is also a risk factor for some extragastric diseases and whether it is protective against some recently emergent medical problems, such as childhood-onset asthma and obesity.
Helicobacter pylori colonizes the stomach in ~50% of the world’s human population, essentially for life unless eradicated by antibiotic treatment. Colonization with this organism is the main risk factor for peptic ulceration (Chap. 348) as well as for gastric adenocarcinoma and gastric mucosa-associated lymphoid tissue (MALT) lymphoma (Chap. 109). Treatment for H. pylori has revolutionized the management of peptic ulcer disease, providing a permanent cure in most cases. Such treatment also represents first-line therapy for patients with low-grade gastric MALT lymphoma. Treatment of H. pylori is of no benefit in the treatment of gastric adenocarcinoma, but prevention of H. pylori colonization could potentially prevent gastric malignancy and peptic ulceration. In contrast, increasing evidence indicates that lifelong H. pylori colonization may offer some protection against complications of gastroesophageal reflux disease (GERD), including esophageal adenocarcinoma. Recent research has focused on whether H. pylori colonization is also a risk factor for some extragastric diseases and whether it is protective against some recently emergent medical problems, such as childhood-onset asthma and obesity.
ETIOLOGIC AGENT
Helicobacter pylori H. pylori is a gram-negative bacillus that has naturally colonized humans for at least 100,000 years, and probably throughout human evolution. It lives in gastric mucus, with a small proportion of the bacteria adherent to the mucosa and possibly a very small number of the organisms entering cells or penetrating the mucosa; the organism’s distribution is never systemic. Its spiral shape and flagella render H. pylori motile in the mucus environment. The organism has several acid-resistance mechanisms, most notably a highly expressed urease that catalyzes urea hydrolysis to produce buffering ammonia. H. pylori is microaerophilic (i.e., requires low levels of oxygen), is slow-growing, and requires complex growth media in vitro.
Other Helicobacter Species A very small proportion of gastric Helico-bacter infections are due to species other than H. pylori, possibly acquired as zoonoses. These non-pylori gastric helicobacters are associated with low-level inflammation and occasionally with disease. In immunocompromised hosts, several nongastric (intestinal) Helicobacter species can cause disease with clinical features resembling those of Campylobacter infections; these species are covered in Chap. 192.
EPIDEMIOLOGY
![]() Prevalence and Risk Factors The prevalence of H. pylori among adults is <30% in most parts of the United States and in other developed countries as opposed to >80% in most developing countries. In the United States, prevalence varies with age: up to 50% of 60-year-old persons, ~20% of 30-year-old persons, and fewer than 10% of children are colonized. H. pylori is usually acquired in childhood. The age association is due mostly to a birth-cohort effect whereby current 60-year-olds were more commonly colonized as children than are current children. Spontaneous acquisition or loss of H. pylori in adulthood is uncommon. Childhood acquisition explains why the main risk factors for infection are markers of crowding and social deprivation in childhood.
Prevalence and Risk Factors The prevalence of H. pylori among adults is <30% in most parts of the United States and in other developed countries as opposed to >80% in most developing countries. In the United States, prevalence varies with age: up to 50% of 60-year-old persons, ~20% of 30-year-old persons, and fewer than 10% of children are colonized. H. pylori is usually acquired in childhood. The age association is due mostly to a birth-cohort effect whereby current 60-year-olds were more commonly colonized as children than are current children. Spontaneous acquisition or loss of H. pylori in adulthood is uncommon. Childhood acquisition explains why the main risk factors for infection are markers of crowding and social deprivation in childhood.
![]() Transmission Humans are the only important reservoir of H. pylori. Children may acquire the organism from their parents (most often the primary caregiver) or from other children. The former is more common in developed countries and the latter in less developed countries. Whether transmission takes place more often by the fecal-oral or the oral-oral route is unknown, but H. pylori is easily cultured from vomitus and gastroesophageal refluxate and is less easily cultured from stool.
Transmission Humans are the only important reservoir of H. pylori. Children may acquire the organism from their parents (most often the primary caregiver) or from other children. The former is more common in developed countries and the latter in less developed countries. Whether transmission takes place more often by the fecal-oral or the oral-oral route is unknown, but H. pylori is easily cultured from vomitus and gastroesophageal refluxate and is less easily cultured from stool.
PATHOLOGY AND PATHOGENESIS
H. pylori colonization induces chronic superficial gastritis, a tissue response in the stomach that includes infiltration of the mucosa by both mononuclear and polymorphonuclear cells. (The term gastritis should be used specifically to describe histologic features; it has also been used to describe endoscopic appearances and even symptoms, but these features do not correlate with microscopic findings or even with the presence of H. pylori.) Although H. pylori is capable of numerous adaptations that prevent excessive stimulation of the immune system, colonization is accompanied by a considerable persistent local and systemic immune response, including the production of antibodies and cell-mediated responses. However, these responses are ineffective in clearing the bacterium. This inefficient clearing appears to be due in part to H. pylori’s downregulation of the immune system, which fosters its own persistence.
Most H. pylori–colonized persons do not develop clinical sequelae. That some persons develop overt disease whereas others do not is related to a combination of factors: bacterial strain differences, host susceptibility to disease, and environmental factors.
![]() Bacterial Virulence Factors Several H. pylori virulence factors are more common among strains that are associated with disease than among those that are not. The cag island is a group of genes that encodes a bacterial type IV secretion system. Through this system, an effector protein, CagA, is translocated into epithelial cells, where it may be transformed by phosphorylation and induces host cell signal transduction; proliferative, cytoskeletal, and inflammatory changes in the cell result. The protein at the tip of the secretory apparatus, CagL, binds to integrins on the cell surface, transducing further signaling. Finally, soluble components of the peptidoglycan cell wall enter the cell, mediated by the same secretory system. These components are recognized by the emergency intracellular bacterial receptor Nod1, which stimulates a proinflammatory cytokine response resulting in enhanced gastric inflammation. Carriage of cag-positive strains increases the risk of peptic ulcer or gastric adenocarcinoma. A second major virulence factor is the vacuolating cytotoxin VacA, which forms pores in cell membranes. VacA is polymorphic, and carriage of more active forms also increases the risk of disease. Other bacterial factors that are associated with increased disease risk include adhesins, such as BabA (which binds to blood group antigens on epithelial cells), and incompletely characterized factors, such as another recently described bacterial type 4 secretion system.
Bacterial Virulence Factors Several H. pylori virulence factors are more common among strains that are associated with disease than among those that are not. The cag island is a group of genes that encodes a bacterial type IV secretion system. Through this system, an effector protein, CagA, is translocated into epithelial cells, where it may be transformed by phosphorylation and induces host cell signal transduction; proliferative, cytoskeletal, and inflammatory changes in the cell result. The protein at the tip of the secretory apparatus, CagL, binds to integrins on the cell surface, transducing further signaling. Finally, soluble components of the peptidoglycan cell wall enter the cell, mediated by the same secretory system. These components are recognized by the emergency intracellular bacterial receptor Nod1, which stimulates a proinflammatory cytokine response resulting in enhanced gastric inflammation. Carriage of cag-positive strains increases the risk of peptic ulcer or gastric adenocarcinoma. A second major virulence factor is the vacuolating cytotoxin VacA, which forms pores in cell membranes. VacA is polymorphic, and carriage of more active forms also increases the risk of disease. Other bacterial factors that are associated with increased disease risk include adhesins, such as BabA (which binds to blood group antigens on epithelial cells), and incompletely characterized factors, such as another recently described bacterial type 4 secretion system.
Host Genetic and Environmental Factors The best-characterized host determinants of disease are genetic polymorphisms leading to enhanced activation of the innate immune response, including polymorphisms in cytokine genes or in genes encoding bacterial recognition proteins such as Toll-like receptors. For example, colonized people with polymorphisms in the interleukin 1 gene that increase the production of this cytokine in response to H. pylori infection are at increased risk of gastric adenocarcinoma. In addition, environmental cofactors are important in pathogenesis. Smoking increases the risks of duodenal ulcers and gastric cancer in H. pylori–positive individuals. Diets high in salt and preserved foods increase cancer risk, whereas diets high in antioxidants and vitamin C are modestly protective.
Distribution of Gastritis and Differential Disease Risk The pattern of gastric inflammation is associated with disease risk: antral-predominant gastritis is most closely linked with duodenal ulceration, whereas pan-gastritis is linked with gastric ulceration and adenocarcinoma. This difference probably explains why patients with duodenal ulceration are not at high risk of developing gastric adenocarcinoma later in life, despite being colonized by H. pylori.
PATHOGENESIS OF DUODENAL ULCERATION How gastric colonization causes duodenal ulceration is now becoming more clear. H. pylori–induced inflammation of the gastric antrum diminishes the number of somatostatin-producing D cells. Because somatostatin inhibits gastrin release, gastrin levels are higher than in H. pylori–negative persons, and these higher levels lead to increased meal-stimulated acid secretion from the relatively spared gastric corpus. How this situation increases duodenal ulcer risk remains controversial, but the increased acid secretion may contribute to the formation of the potentially protective gastric metaplasia found in the duodenum of duodenal ulcer patients. Gastric metaplasia in the duodenum may become colonized by H. pylori and subsequently inflamed and ulcerated.
PATHOGENESIS OF GASTRIC ULCERATION AND GASTRIC ADENOCARCINOMA The pathogenesis of these conditions is less well understood, although both arise in association with pan- or corpus-predominant gastritis. The hormonal changes described above still occur, but the inflammation in the gastric corpus means that it produces less acid (hypochlorhydria) despite hypergastrinemia. Gastric ulcers usually occur at the junction of antral and corpus-type mucosa, an area that is often particularly inflamed. Gastric cancer probably stems from progressive DNA damage and the survival of abnormal epithelial cell clones. The DNA damage is thought to be due principally to reactive oxygen and nitrogen species arising from inflammatory cells, perhaps in relation to other bacteria that survive in a hypochlorhydric stomach. Longitudinal analyses of gastric biopsy specimens taken years apart from the same patient show that the common intestinal type of gastric adenocarcinoma follows stepwise changes from simple gastritis to gastric atrophy, intestinal metaplasia, and dysplasia. A second, diffuse type of gastric adenocarcinoma found more commonly in younger adults may arise directly from chronic gastritis without atrophic changes.
CLINICAL MANIFESTATIONS
Essentially all H. pylori–colonized persons have histologic gastritis, but only ~10–15% develop associated illnesses such as peptic ulceration, gastric adenocarcinoma, or gastric lymphoma (Fig. 188-1). Rates among women are less than half of those among men for both diseases.
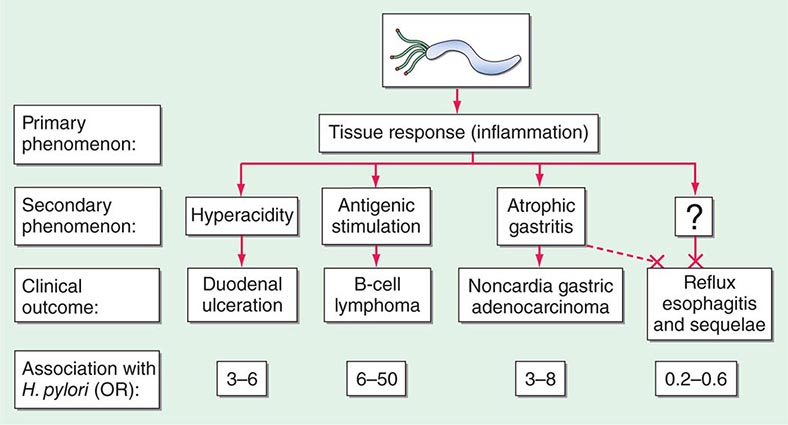
FIGURE 188-1 Schematic of the relationships between colonization with Helicobacter pylori and diseases of the upper gastrointestinal tract. Essentially all persons colonized with H. pylori develop a host response, which is generally termed chronic gastritis. The nature of the host’s interaction with the particular bacterial population determines the clinical outcome. H. pylori colonization increases the lifetime risk of peptic ulcer disease, noncardia gastric cancer, and B-cell non-Hodgkin’s gastric lymphoma (odds ratios [ORs] for all, >3). In contrast, a growing body of evidence indicates that H. pylori colonization (especially with cagA+ strains) protects against adenocarcinoma of the esophagus (and the sometimes related gastric cardia) and premalignant lesions such as Barrett’s esophagus (OR, <1). Although the incidences of peptic ulcer disease (cases not due to nonsteroidal anti-inflammatory drugs) and noncardia gastric cancer are declining in developed countries, the incidence of adenocarcinoma of the esophagus is increasing. (Adapted from MJ Blaser: Hypothesis: The changing relationships of Helicobacter pylori and humans: Implications for health and disease. J Infect Dis 179:1523, 1999, with permission.)
![]() Peptic Ulcer Disease Worldwide, >80% of duodenal ulcers and >60% of gastric ulcers are related to H. pylori colonization (Chap. 348). However, in particular, the proportion of gastric ulcers caused by aspirin and nonsteroidal anti-inflammatory drugs (NSAIDs) is increasing, and in many developed countries these drugs have overtaken H. pylori as a cause of gastric ulceration. The main lines of evidence supporting an ulcer-promoting role for H. pylori are that (1) the presence of the organism is a risk factor for the development of ulcers, (2) non-NSAID-induced ulcers rarely develop in the absence of H. pylori, (3) eradication of H. pylori virtually abolishes long-term ulcer relapse, and (4) experimental H. pylori infection of gerbils can cause gastric ulceration.
Peptic Ulcer Disease Worldwide, >80% of duodenal ulcers and >60% of gastric ulcers are related to H. pylori colonization (Chap. 348). However, in particular, the proportion of gastric ulcers caused by aspirin and nonsteroidal anti-inflammatory drugs (NSAIDs) is increasing, and in many developed countries these drugs have overtaken H. pylori as a cause of gastric ulceration. The main lines of evidence supporting an ulcer-promoting role for H. pylori are that (1) the presence of the organism is a risk factor for the development of ulcers, (2) non-NSAID-induced ulcers rarely develop in the absence of H. pylori, (3) eradication of H. pylori virtually abolishes long-term ulcer relapse, and (4) experimental H. pylori infection of gerbils can cause gastric ulceration.
Gastric Adenocarcinoma and Lymphoma Prospective nested case-control studies have shown that H. pylori colonization is a risk factor for adenocarcinomas of the distal (noncardia) stomach (Chap. 109). Long-term experimental infection of gerbils also may result in gastric adenocarcinoma. Moreover, H. pylori may induce primary gastric lymphoma, although this condition is much less common. Many low-grade gastric B-cell lymphomas are dependent on H. pylori for continuing growth and proliferation, and these tumors may regress either fully or partially after H. pylori eradication. However, they require careful short- and long-term monitoring, and some necessitate additional treatment with chemotherapeutic agents.
Functional Dyspepsia Many patients have upper gastrointestinal symptoms but have normal results on upper gastrointestinal endoscopy (so-called functional or nonulcer dyspepsia; Chap. 348). Because H. pylori is common, some of these patients will be colonized with the organism. H. pylori eradication leads to symptom resolution a little more commonly (from 0 to 7% in different studies) than does placebo treatment. Whether such patients have peptic ulcers in remission at the time of endoscopy or whether a small subgroup of patients with “true” functional dyspepsia respond to H. pylori treatment is unclear.
Protection Against Peptic Esophageal Disease, Including Esophageal Adenocarcinoma Much interest has focused on a protective role for H. pylori against GERD (Chap. 347), Barrett’s esophagus (Chap. 347), and adenocarcinoma of the esophagus and gastric cardia (Chap. 109). The main lines of evidence for this role are (1) that there is a temporal relationship between a falling prevalence of gastric H. pylori colonization and a rising incidence of these conditions; (2) that, in most studies, the prevalence of H. pylori colonization (especially with proinflammatory cagA+ strains) is significantly lower among patients with these esophageal diseases than among control participants; and (3) that, in prospective nested studies (see above), the presence of H. pylori is inversely related to these cancers. The mechanism underlying this protective effect is likely H. pylori–induced hypochlorhydria. Because, at the individual level, GERD symptoms may decrease, worsen, or remain unchanged after H. pylori treatment, concerns about GERD should not affect decisions about whether to treat H. pylori when an indication exists.
Other Pathologies H. pylori has an increasingly recognized role in other gastric pathologies. It may be one initial precipitant of autoimmune gastritis and pernicious anemia and also may predispose some patients to iron deficiency through occult blood loss and/or hypochlorhydria and reduced iron absorption. In addition, several extragastrointestinal pathologies have been linked with H. pylori colonization, although evidence of causality is less strong. Studies of H. pylori treatment in idiopathic thrombocytopenic purpura have consistently described improvement in or even normalization of platelet counts. Potentially important but even more controversial associations are with ischemic heart disease and cerebrovascular disease. However, the strength of the latter associations is reduced if confounding factors are taken into account, and most authorities consider the associations to be noncausal. Several studies have shown an inverse association of cagA+ H. pylori with childhood-onset asthma, hay fever, and atopic disorders. These associations have been shown to be causal in animal models, but causality in humans and the size of any effect have not been established.
DIAGNOSIS
Tests for H. pylori fall into two groups: tests that require upper gastrointestinal endoscopy and simpler tests that can be performed in the clinic (Table 188-1).
TESTS COMMONLY USED TO DETECT HELICOBACTER PYLORI |
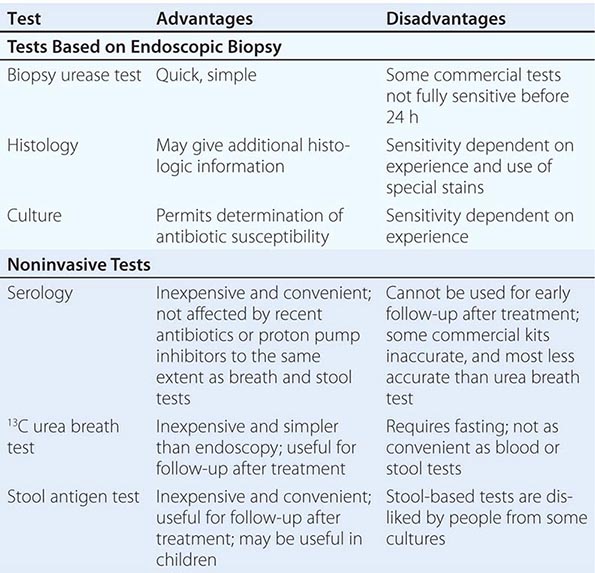
Endoscopy-Based Tests Endoscopy is usually unnecessary in the initial management of young patients with simple dyspepsia but is commonly used to exclude malignancy and make a positive diagnosis in older patients or those with “alarm” symptoms. If endoscopy is performed, the most convenient biopsy-based test is the biopsy urease test, in which one large or two small gastric biopsy specimens are placed into a gel containing urea and an indicator. The presence of H. pylori urease leads to a pH alteration and therefore to a color change, which often occurs within minutes but can require up to 24 h. Histologic examination of biopsy specimens for H. pylori also is accurate, provided that a special stain (e.g., a modified Giemsa or silver stain) permitting optimal visualization of the organism is used. If biopsy specimens are obtained from both antrum and corpus, histologic study yields additional information, including the degree and pattern of inflammation and the presence of any atrophy, metaplasia, or dysplasia. Microbiologic culture is most specific but may be insensitive because of difficulty with H. pylori isolation. Once the organism is cultured, its identity as H. pylori can be confirmed by its typical appearance on Gram’s stain and its positive reactions in oxidase, catalase, and urease tests. Moreover, the organism’s susceptibility to antibiotics can be determined, and this information can be clinically useful in difficult cases. The occasional biopsy specimens containing the less common non-pylori gastric helicobacters give only weakly positive results in the biopsy urease test. Positive identification of these bacteria requires visualization of the characteristic long, tight spirals in histologic sections; they cannot easily be cultured.
Noninvasive Tests Noninvasive H. pylori testing is the norm if gastric cancer does not need to be excluded by endoscopy. The best-established test (and a very accurate one) is the urea breath test. In this simple test, the patient drinks a solution of urea labeled with the nonradioactive isotope 13C and then blows into a tube. If H. pylori urease is present, the urea is hydrolyzed, and labeled carbon dioxide is detected in breath samples. The stool antigen test, a simple and accurate test using monoclonal antibodies specific for H. pylori antigens, is more convenient and potentially less expensive than the urea breath test, but some patients dislike sampling stool. The simplest tests for ascertaining H. pylori status are serologic assays measuring specific IgG levels in serum by enzyme-linked immunosorbent assay or immunoblot. The best of these tests are as accurate as other diagnostic methods, but many commercial tests—especially rapid office tests—do not perform well.
Use of Tests to Assess Treatment Success The urea breath test, the stool antigen test, and biopsy-based tests can all be used to assess the success of treatment (Fig. 188-2). However, because these tests are dependent on H. pylori load, their use <4 weeks after treatment may yield false-negative results. Furthermore, these tests are unreliable if performed within 4 weeks of intercurrent treatment with antibiotics or bismuth compounds or within 2 weeks of the discontinuation of proton pump inhibitor (PPI) treatment. In the assessment of treatment success, noninvasive tests are normally preferred; however, after gastric ulceration, endoscopy should be repeated to ensure healing and to exclude gastric carcinoma by further histologic sampling. Serologic tests are not used to monitor treatment success, as the gradual drop in titer of H. pylori–specific antibodies is too slow to be of practical use.
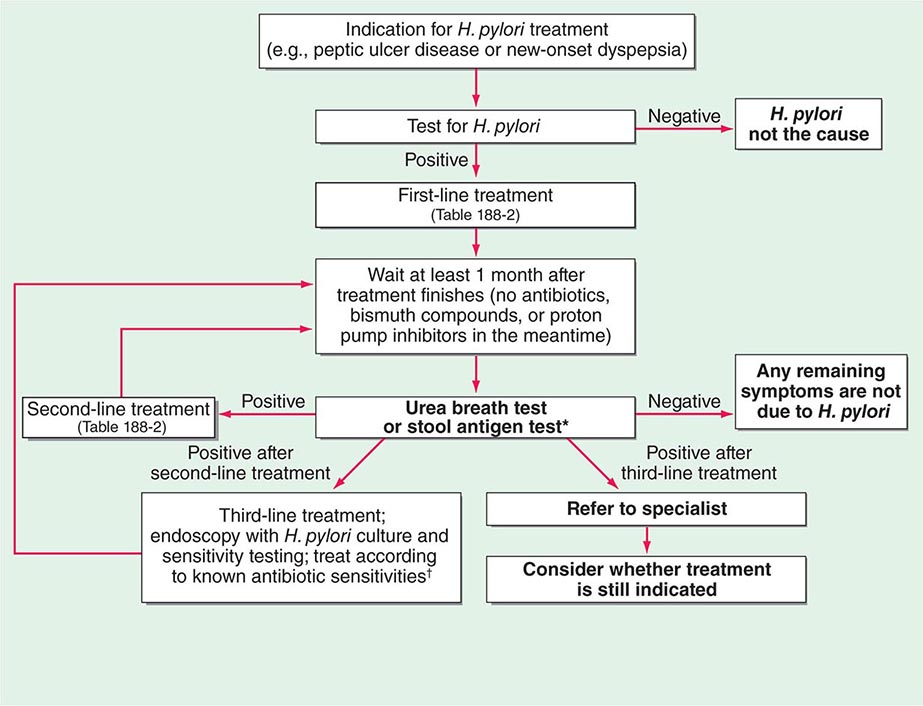
FIGURE 188-2 Algorithm for the management of Helicobacter pylori infection. *Note that either the urea breath test or the stool antigen test can be used in this algorithm. Occasionally, endoscopy and a biopsy-based test are used instead of either of these tests in follow-up after treatment. The main indication for these invasive tests is gastric ulceration; in this condition, as opposed to duodenal ulceration, it is important to check healing and to exclude underlying gastric adenocarcinoma. However, even in this situation, patients undergoing endoscopy may still be receiving proton pump inhibitor therapy, which precludes H. pylori testing. Thus a urea breath test or a stool antigen test is still required at a suitable interval after the end of therapy to determine whether treatment has been successful (see text). †Some authorities use empirical third-line regimens, of which several have been described.
TREATMENT | HELICOBACTER PYLORI INFECTION |
INDICATIONS
The most clear-cut indications for treatment are H. pylori–related duodenal or gastric ulceration or low-grade gastric B-cell lymphoma. Whether or not the ulcers are currently active, H. pylori should be eradicated in patients with documented ulcer disease to prevent relapse (Fig. 188-2). Testing for H. pylori and treatment if the results are positive also have been advocated in uninvestigated simple dyspepsia, but only when the prevalence of H. pylori in the community is >20% are these measures more cost-effective than simply treating the dyspepsia with PPIs. Guidelines have recommended H. pylori treatment in functional dyspepsia in case the patient is one of the perhaps 0–7% who will benefit from such treatment (beyond placebo effects). Some guidelines also recommend treatment of conditions not definitively known to respond to H. pylori eradication, including idiopathic thrombocytopenic purpura, vitamin B12 deficiency, and iron-deficiency anemia (in the last instance, only when other causes have been carefully excluded). Test-and-treat has emerged as a common clinical practice in recent years despite the lack of direct evidence that it is advantageous; whether this practice will survive the scrutiny of time and further study remains to be determined. For individuals with a strong family history of gastric cancer, treatment to eradicate H. pylori in the hope of reducing their cancer risk is reasonable but of unproven value. Currently, widespread community screening for and treatment of H. pylori as primary prophylaxis for gastric cancer and peptic ulcers are not recommended in most countries, mainly because the extent of the consequent reduction in cancer risk is not known. Several studies have found a modestly reduced cancer risk after treatment, but the period of follow-up is still fairly short and the size of the effect in different populations remains unclear. Other reasons not to treat H. pylori in asymptomatic populations at present include (1) the adverse side effects (which are common and can be severe in rare cases) of the multiple-antibiotic regimens used; (2) antibiotic resistance, which may emerge in H. pylori or other incidentally carried bacteria; (3) the anxiety that may arise in otherwise healthy people, especially if treatment is unsuccessful; and (4) the existence of a subset of people who will develop GERD symptoms after treatment, although, on average, H. pylori treatment does not affect GERD symptoms or severity. Despite the absence of screening strategies, many doctors treat H. pylori if it is known to be present (particularly in children and younger adults), even when the patient is asymptomatic. The rationale is that it reduces patient concern and may reduce future gastric cancer risk and that any reduction in risk is likely to be greater in younger patients. However, such practices do not factor in any potential benefits of H. pylori colonization. Overall, despite widespread clinical activity in this area, most treatment of asymptomatic H. pylori carriage is given without a firm evidence base.
REGIMENS
Although H. pylori is susceptible to a wide range of antibiotics in vitro, monotherapy is not usually successful, probably because of inadequate antibiotic delivery to the colonization niche. Failure of monotherapy prompted the development of multidrug regimens, the most successful of which are triple and quadruple combinations. Current regimens consist of a PPI and two or three antimicrobial agents given for 7–14 days (Table 188-2). Research on optimizing drug combinations to increase efficacy continues, and guidelines are likely to change as the field develops and as countries increasingly tailor treatment to suit local antibiotic resistance patterns and economic needs.
COMMONLY RECOMMENDED TREATMENT REGIMENS FOR HELICOBACTER PYLORI |
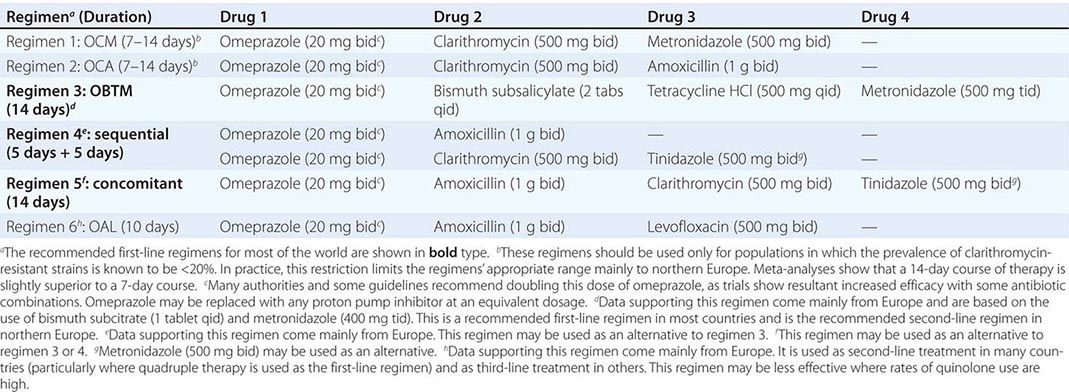
![]() The two most important factors in successful H. pylori treatment are the patient’s close compliance with the regimen and the use of drugs to which the patient’s strain of H. pylori has not acquired resistance. Treatment failure following minor lapses in compliance is common and often leads to acquired resistance to metronidazole or clarithromycin. To stress the importance of compliance, written instructions should be given to the patient, and minor side effects of the regimen should be explained. Increasing levels of H. pylori resistance to clarithromycin, quinolones, and—to a lesser extent—metronidazole are of growing concern and are thought to be responsible for the reduced efficacy of previously popular clarithromycin-based triple-therapy regimens worldwide. Treatment with these regimens is now virtually confined to certain northern European countries where the use of clarithromycin (or azithromycin) for respiratory infections has not been widespread and resistance rates in H. pylori are still low. Strains of H. pylori with some degree of in vitro resistance to metronidazole are common but still may be eradicated with metronidazole-containing regimens, which have only slightly reduced efficacy in vivo. Assessment of antibiotic susceptibilities before treatment would be optimal but is not usually undertaken because endoscopy and mucosal biopsy are necessary to obtain H. pylori for culture and because most microbiology laboratories are inexperienced in H. pylori culture. In the absence of susceptibility information, the patient’s history of (even distant) antibiotic use for other conditions should be ascertained; use of the previously administered agent(s) should then be avoided if possible, particularly in the case of clarithromycin (e.g., previous use for upper respiratory infection) and quinolones. If initial H. pylori treatment fails, the usual approach is empirical re-treatment with another drug regimen (Table 188-2). The third-line approach should ideally be endoscopy, biopsy, and culture plus treatment based on documented antibiotic sensitivities. However, empirical third-line therapies are often used.
The two most important factors in successful H. pylori treatment are the patient’s close compliance with the regimen and the use of drugs to which the patient’s strain of H. pylori has not acquired resistance. Treatment failure following minor lapses in compliance is common and often leads to acquired resistance to metronidazole or clarithromycin. To stress the importance of compliance, written instructions should be given to the patient, and minor side effects of the regimen should be explained. Increasing levels of H. pylori resistance to clarithromycin, quinolones, and—to a lesser extent—metronidazole are of growing concern and are thought to be responsible for the reduced efficacy of previously popular clarithromycin-based triple-therapy regimens worldwide. Treatment with these regimens is now virtually confined to certain northern European countries where the use of clarithromycin (or azithromycin) for respiratory infections has not been widespread and resistance rates in H. pylori are still low. Strains of H. pylori with some degree of in vitro resistance to metronidazole are common but still may be eradicated with metronidazole-containing regimens, which have only slightly reduced efficacy in vivo. Assessment of antibiotic susceptibilities before treatment would be optimal but is not usually undertaken because endoscopy and mucosal biopsy are necessary to obtain H. pylori for culture and because most microbiology laboratories are inexperienced in H. pylori culture. In the absence of susceptibility information, the patient’s history of (even distant) antibiotic use for other conditions should be ascertained; use of the previously administered agent(s) should then be avoided if possible, particularly in the case of clarithromycin (e.g., previous use for upper respiratory infection) and quinolones. If initial H. pylori treatment fails, the usual approach is empirical re-treatment with another drug regimen (Table 188-2). The third-line approach should ideally be endoscopy, biopsy, and culture plus treatment based on documented antibiotic sensitivities. However, empirical third-line therapies are often used.
Non-pylori gastric helicobacters are treated in the same way as H. pylori. However, in the absence of trials, it is unclear whether a positive outcome always represents successful treatment or whether it is sometimes due to natural clearance of the bacteria.
PREVENTION
![]() Carriage of H. pylori has considerable public health significance in developed countries, where it is associated with peptic ulcer disease and gastric adenocarcinoma, and in developing countries, where gastric adenocarcinoma may be an even more common cause of cancer death late in life. If mass prevention were contemplated, vaccination would be the most obvious method, and experimental immunization of animals has given promising results. However, given that H. pylori has co-evolved with its human host over millennia, preventing or eliminating colonization on a population basis may have biological and clinical costs. For example, lifelong absence of H. pylori is a risk factor for GERD complications, including esophageal adenocarcinoma. We have speculated that the disappearance of H. pylori may also be associated with an increased risk of other emergent diseases reflecting aspects of the current Western lifestyle, such as childhood-onset asthma and allergy.
Carriage of H. pylori has considerable public health significance in developed countries, where it is associated with peptic ulcer disease and gastric adenocarcinoma, and in developing countries, where gastric adenocarcinoma may be an even more common cause of cancer death late in life. If mass prevention were contemplated, vaccination would be the most obvious method, and experimental immunization of animals has given promising results. However, given that H. pylori has co-evolved with its human host over millennia, preventing or eliminating colonization on a population basis may have biological and clinical costs. For example, lifelong absence of H. pylori is a risk factor for GERD complications, including esophageal adenocarcinoma. We have speculated that the disappearance of H. pylori may also be associated with an increased risk of other emergent diseases reflecting aspects of the current Western lifestyle, such as childhood-onset asthma and allergy.
189 | Infections Due to Pseudomonas Species and Related Organisms |
The pseudomonads are a heterogeneous group of gram-negative bacteria that have in common an inability to ferment lactose. Formerly classified in the genus Pseudomonas, the members of this group have been assigned to three medically important genera—Pseudomonas, Burkholderia, and Stenotrophomonas—whose biologic behaviors encompass both similarities and marked differences and whose genetic repertoires differ in many respects. The pathogenicity of most pseudomonads is based on opportunism; the exceptions are the organisms that cause melioidosis (Burkholderia pseudomallei) and glanders (Burkholderia mallei), which can be considered as primary pathogens.
Pseudomonas aeruginosa, the major pathogen of the group, is a significant cause of infections in hospitalized patients and in patients with cystic fibrosis (CF; Chap. 313). Cytotoxic chemotherapy, mechanical ventilation, and broad-spectrum antibiotic therapy probably paved the way for colonization and infection of increasing numbers of hospitalized patients by this organism. Thus most conditions predisposing to P. aeruginosa infections have involved host compromise and/or broad-spectrum antibiotic use. The other members of the genus Pseudomonas—Pseudomonas putida, Pseudomonas fluorescens, and Pseudomonas stutzeri—infect humans infrequently.
The genus Burkholderia comprises more than 40 species, of which Burkholderia cepacia is most frequently encountered in Western countries. Like P. aeruginosa, B. cepacia is both a nosocomial pathogen and a cause of infection in CF. The other medically important members of this genus are B. pseudomallei and B. mallei, the etiologic agents of melioidosis and glanders, respectively.
The genus Stenotrophomonas contains one species of medical significance, Stenotrophomonas maltophilia (previously classified in the genera Pseudomonas and Xanthomonas). This organism is strictly an opportunist that “overgrows” in the setting of potent broad-spectrum antibiotic use.
PSEUDOMONAS AERUGINOSA
EPIDEMIOLOGY
P. aeruginosa is found in most moist environments. Soil, plants, vegetables, tap water, and countertops are all potential reservoirs for this microbe, as it has simple nutritional needs. Given the ubiquity of P. aeruginosa, simple contact with the organism is not sufficient for colonization or infection. Clinical and experimental observations suggest that P. aeruginosa infection often occurs concomitantly with host defense compromise, mucosal trauma, physiologic derangement, and antibiotic-mediated suppression of normal flora. Thus, it comes as no surprise that the majority of P. aeruginosa infections occur in intensive care units (ICUs), where these factors frequently converge. The organism is initially acquired from environmental sources, but patient-to-patient spread also occurs in clinics and families.
In the past, burned patients appeared to be unusually susceptible to P. aeruginosa. For example, in 1959–1963, Pseudomonas burn-wound sepsis was the principal cause of death in 60% of burned patients dying at the U.S. Army Institute of Surgical Research. For reasons that are unclear, P. aeruginosa infection in burns is no longer the major problem that it was during the 1950s and 1960s. Similarly, in the 1960s, P. aeruginosa appeared as a common pathogen in patients receiving cytotoxic chemotherapy at many institutions in the United States, but it subsequently diminished in importance. Despite this subsidence, P. aeruginosa remains one of the most feared pathogens in this population because of its high attributable mortality rate.
![]() In some parts of Asia and Latin America, P. aeruginosa continues to be the most common cause of gram-negative bacteremia in neutropenic patients.
In some parts of Asia and Latin America, P. aeruginosa continues to be the most common cause of gram-negative bacteremia in neutropenic patients.
In contrast to the trends for burned patients and neutropenic patients in the United States, the incidence of P. aeruginosa infections among patients with CF has not changed. P. aeruginosa remains the most common contributing factor to respiratory failure in CF and is responsible for the majority of deaths among CF patients.
LABORATORY FEATURES
P. aeruginosa is a nonfastidious, motile, gram-negative rod that grows on most common laboratory media, including blood and MacConkey agars. It is easily identified in the laboratory on primary-isolation agar plates by pigment production that confers a yellow to dark green or even bluish appearance. Colonies have a shiny “gun-metal” appearance and a characteristic fruity odor. Two of the identifying biochemical characteristics of P. aeruginosa are an inability to ferment lactose on MacConkey agar and a positive reaction in the oxidase test. Most strains are identified on the basis of these readily detectable laboratory features even before extensive biochemical testing is done. Some isolates from CF patients are easily identified by their mucoid appearance, which is due to the production of large amounts of the mucoid exopolysaccharide or alginate.
PATHOGENESIS
Unraveling the mechanisms that underlie disease caused by P. aeruginosa has proved challenging. Of the common gram-negative bacteria, no other species produces such a large number of putative virulence factors (Table 189-1). Yet P. aeruginosa rarely initiates an infectious process in the absence of host injury or compromise, and few of its putative virulence factors have been shown definitively to be involved in disease in humans. Despite its metabolic versatility and possession of multiple colonizing factors, P. aeruginosa exhibits no competitive advantage over enteric bacteria in the human gut; neither is it a normal inhabitant of the human gastrointestinal tract, despite the host’s continuous environmental exposure to the organism.
MAIN PUTATIVE VIRULENCE FACTORS OF PSEUDOMONAS AERUGINOSA |
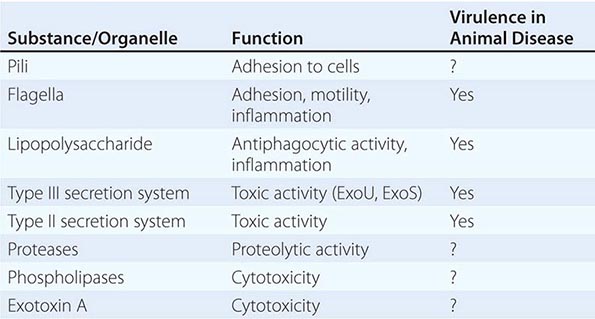
Virulence Attributes Involved in Acute P. aeruginosa Infections • MOTILITY AND COLONIZATION A general tenet of bacterial pathogenesis is that most bacteria must adhere to surfaces or colonize a host niche in order to initiate disease. Most pathogens examined thus far possess adherence factors called adhesins. P. aeruginosa is no exception. Among its many adhesins are its pili, which demonstrate adhesive properties for a variety of cells and adhere best to injured cell surfaces. In the organism’s flagellum, the flagellin molecule binds to cells, and the flagellar cap attaches to mucins through the recognition of glycan chains. Other P. aeruginosa adhesins include the outer core of the lipopolysaccharide (LPS) molecule, which binds to the cystic fibrosis transmembrane conductance regulator (CFTR) and aids in internalization of the organism, and the alginate coat of mucoid strains, which enhances adhesion to cells and mucins. In addition, membrane proteins and lectins have been proposed as colonization factors. The deletion of any given adhesin is not sufficient to abrogate the ability of P. aeruginosa to colonize surfaces. Motility is important in host invasion via mucosal surfaces in some animal models; however, nonmotile strains are not uniformly avirulent.
EVASION OF HOST DEFENSES The transition from bacterial colonization to disease requires the evasion of host defenses followed by invasion of the microorganism. P. aeruginosa appears to be well equipped for evasion. Attached bacteria inject four known toxins (ExoS or ExoU, ExoT, and ExoY) via a type III secretion system that allows the bacteria to evade phagocytic cells either by direct cytotoxicity or by inhibition of phagocytosis. Mutants with defects in this system fail to disseminate in some animal models of infection. The type II secretion system as a whole secretes toxins that can kill animals, and some of its secreted toxins, such as exotoxin A, have the potential to kill phagocytic cells. Multiple proteases secreted by this system may degrade host effector molecules, such as cytokines and chemokines, that are released in response to infection. Thus this system may also contribute to host evasion.
TISSUE INJURY Among gram-negative bacteria, P. aeruginosa probably produces the largest number of substances that are toxic to cells and thus may injure tissues. The toxins secreted by its type III secretion system are capable of tissue injury. However, their delivery requires the adherence of the organism to cells. Thus, the effects of these toxins are likely to be local or to depend on the presence of vast numbers of bacteria. On the other hand, diffusible toxins, secreted by the organism’s type II secretion system, can act freely wherever they come into contact with cells. Possible effectors include exotoxin A, four different proteases, and at least two phospholipases; in addition to these secreted toxins, rhamnolipids, pyocyanin, and hydrocyanic acid are produced by P. aeruginosa and are all capable of inducing host injury.
INFLAMMATORY COMPONENTS The inflammatory components of P. aeruginosa—e.g., the inflammatory responses to the lipid A component of LPSs and to flagellin, mediated through the Toll-like receptor (TLR) system (principally TLR4 and TLR5)—have been thought to represent important factors in disease causation. Although these inflammatory responses are required for successful defense against P. aeruginosa (i.e., in their absence, animals are defenseless against P. aeruginosa infection), florid responses are likely to result in disease. When the sepsis syndrome and septic shock develop in P. aeruginosa infection, they are probably the result of the host response to one or both of these substances, but injury to the lung by Pseudomonas toxins may also result in sepsis syndromes, possibly by causing cell death and the release of cellular components (e.g., heat-shock proteins) that may activate the TLR or another proinflammatory system.
Chronic P. aeruginosa Infections Chronic infection due to P. aeruginosa occurs mainly in the lungs in the setting of structural pulmonary diseases. The classic example is CF; others include bronchiectasis and chronic relapsing panbronchiolitis, a disease seen in Japan and some Pacific Islands. Hallmarks of these illnesses are altered mucociliary clearance leading to mucus stasis and mucus accumulation in the lungs. There is probably a common factor that selects for P. aeruginosa colonization in these lung diseases—perhaps the adhesiveness of P. aeruginosa for mucus, a phenomenon that is not noted for most other common gram-negative bacteria, and/or the ability of P. aeruginosa to evade host defenses in mucus. Furthermore, P. aeruginosa seems to evolve in ways that allow its prolonged survival in the lung without an early fatal outcome for the host. The strains found in CF patients exhibit minimal production of virulence factors. Some strains even lose the ability to produce pili and flagella, and most become complement-sensitive because of the loss of the O side chain of their LPS molecules. An example of the impact of these changes is found in the organism’s discontinuation of the production of flagellin (probably its most strongly proinflammatory molecule) when it encounters purulent mucus. This response probably dampens the host’s response, allowing the organism to survive in mucus. P. aeruginosa is also believed to lose the ability to secrete many of its injectable toxins during growth in mucus. Although the alginate coat is thought to play a role in the organism’s survival, alginate is not essential, as nonmucoid strains may also predominate for long periods. In short, virulence in chronic infections may be mediated by the chronic but attenuated host inflammatory response, which injures the lungs over decades.
CLINICAL MANIFESTATIONS
P. aeruginosa causes infections at almost all sites in the body but shows a rather strong predilection for the lungs. The infections encountered most commonly in hospitalized patients are described below.
Bacteremia Crude mortality rates exceeding 50% have been reported among patients with P. aeruginosa bacteremia. Consequently, this clinical entity has been much feared, and its management has been attempted with the use of multiple antibiotics. Recent publications report attributable mortality rates of 28–44%, with the precise figure depending on the adequacy of treatment and the seriousness of the underlying disease. In the past, the patient with P. aeruginosa bacteremia classically was neutropenic or had a burn injury. Today, however, a minority of such patients have bacteremic P. aeruginosa infections. Rather, P. aeruginosa bacteremia is seen most often in patients in ICUs.
The clinical presentation of P. aeruginosa bacteremia rarely differs from that of sepsis in general (Chap. 324). Patients are usually febrile, but those who are most severely ill may be in shock or even hypothermic. The only point differentiating this entity from gram-negative sepsis of other causes may be the distinctive skin lesions (ecthyma gangrenosum) of Pseudomonas infection, which occur almost exclusively in markedly neutropenic patients and patients with AIDS. These small or large, painful, reddish, maculopapular lesions have a geographic margin; they are initially pink, then darken to purple, and finally become black and necrotic (Fig. 189-1). Histopathologic studies indicate that the lesions are due to vascular invasion and are teeming with bacteria. Although similar lesions may occur in aspergillosis and mucormycosis, their presence suggests P. aeruginosa bacteremia as the most likely diagnosis.

FIGURE 189-1 Ecthyma gangrenosum in a neutropenic patient 3 days after onset.
TREATMENT | P. AERUGINOSA BACTEREMIA |
(Table 189-2) Antimicrobial treatment of P. aeruginosa bacteremia has been controversial. Before 1971, the outcome of Pseudomonas bacteremia in febrile neutropenic patients treated with the available agents—gentamicin and the polymyxins—was dismal. However, treatment with carbenicillin, with or without an aminoglycoside, significantly improved outcomes. Concurrently, several retrospective analyses suggested that the use of two agents that were synergistic against gram-negative pathogens in vitro resulted in better outcomes in neutropenic patients. Thus, combination therapy became the standard of care—first for P. aeruginosa bacteremia in febrile neutropenic patients and then for all P. aeruginosa infections in neutropenic or nonneutropenic patients.
ANTIBIOTIC TREATMENT OF INFECTIONS DUE TO PSEUDOMONAS AERUGINOSA AND RELATED SPECIES |
With the introduction of newer antipseudomonal drugs, a number of studies have revisited the choice between combination treatment and monotherapy for Pseudomonas bacteremia. Although the majority of experts still favor combination therapy, most of these observational studies indicate that a single modern antipseudomonal β-lactam agent to which the isolate is sensitive is as efficacious as a combination. Even in patients at greatest risk of early death from P. aeruginosa bacteremia (i.e., those with fever and neutropenia), empirical antipseudomonal monotherapy is deemed to be as efficacious as empirical combination therapy by the practice guidelines of the Infectious Diseases Society of America. One firm conclusion is that monotherapy with an aminoglycoside is not optimal.
![]() There are, of course, institutions and countries where rates of susceptibility of P. aeruginosa to first-line antibiotics are <80%. Thus, when a septic patient with a high probability of P. aeruginosa infection is encountered in such settings, empirical combination therapy should be administered until the pathogen is identified and susceptibility data become available. Thereafter, whether one or two agents should be continued remains a matter of individual preference. Recent studies suggest that extended infusions of β-lactams such as cefepime or piperacillin-tazobactam may result in better outcomes of Pseudomonas bacteremia and possibly Pseudomonas pneumonia.
There are, of course, institutions and countries where rates of susceptibility of P. aeruginosa to first-line antibiotics are <80%. Thus, when a septic patient with a high probability of P. aeruginosa infection is encountered in such settings, empirical combination therapy should be administered until the pathogen is identified and susceptibility data become available. Thereafter, whether one or two agents should be continued remains a matter of individual preference. Recent studies suggest that extended infusions of β-lactams such as cefepime or piperacillin-tazobactam may result in better outcomes of Pseudomonas bacteremia and possibly Pseudomonas pneumonia.
Acute Pneumonia Respiratory infections are the most common of all infections caused by P. aeruginosa. This organism appears first or second among the causes of ventilator-associated pneumonia (VAP). However, much debate centers on the actual role of P. aeruginosa in VAP. Many of the relevant data are based on cultures of sputum or endotracheal tube aspirates and may represent nonpathogenic colonization of the tracheobronchial tree, biofilms on the endotracheal tube, or simple tracheobronchitis.
Older reports of P. aeruginosa pneumonia described patients with an acute clinical syndrome of fever, chills, cough, and necrotizing pneumonia indistinguishable from other gram-negative bacterial pneumonias. The traditional accounts described a fulminant infection. Chest radiographs demonstrated bilateral pneumonia, often with nodular densities with or without cavities. This picture is now remarkably rare. Today, the typical patient is on a ventilator, has a slowly progressive infiltrate, and has been colonized with P. aeruginosa for days. While some cases may progress rapidly over 48–72 h, they are the exceptions. Nodular densities are not commonly seen. However, infiltrates may go on to necrosis. Necrotizing pneumonia has also been seen in the community (e.g., after inhalation of hot-tub water contaminated with P. aeruginosa). The typical patient has fever, leukocytosis, and purulent sputum, and the chest radiograph shows a new infiltrate or the expansion of a preexisting infiltrate. Chest examination generally detects rales or dullness. Of course, such findings are quite common among ventilated patients in the ICU. A sputum Gram’s stain showing mainly polymorphonuclear leukocytes (PMNs) in conjunction with a culture positive for P. aeruginosa in this setting suggests a diagnosis of acute P. aeruginosa pneumonia. There is no consensus about whether an invasive procedure (e.g., bronchoalveolar lavage or protected-brush sampling of the distal airways) is superior to tracheal aspiration to obtain samples for lung cultures in order to substantiate the occurrence of P. aeruginosa pneumonia and prevent antibiotic overuse.
TREATMENT | ACUTE PNEUMONIA |
(Table 189-2) Therapy for P. aeruginosa pneumonia has been unsatisfactory. Reports suggest mortality rates of 40–80%, but how many of these deaths are attributable to underlying disease remains unknown. The drugs of choice for P. aeruginosa pneumonia are similar to those given for bacteremia. A potent antipseudomonal β-lactam drug is the mainstay of therapy. Failure rates were high when aminoglycosides were used as single agents, possibly because of their poor penetration into the airways and their binding to airway secretions. Thus a strong case cannot be made for the inclusion of the aminoglycoside component in regimens used against fully susceptible organisms, especially given the evidence that aminoglycosides are not optimally active in the lungs at concentrations normally reached after IV administration. Nonetheless, aminoglycosides are commonly used in clinical practice. Some experts suggest the combination of a β-lactam agent and an antipseudomonal fluoroquinolone instead when combination therapy is desired.
![]() Chronic Respiratory Tract Infections P. aeruginosa is responsible for chronic infections of the airways associated with a number of underlying or predisposing conditions—most commonly CF (Chap. 313). A state of chronic colonization beginning early in childhood is seen in some Asian populations with chronic or diffuse panbronchiolitis, a disease of unknown etiology. P. aeruginosa is one of the organisms that colonizes damaged bronchi in bronchiectasis, a disease secondary to multiple causes in which profound structural abnormalities of the airways result in mucus stasis.
Chronic Respiratory Tract Infections P. aeruginosa is responsible for chronic infections of the airways associated with a number of underlying or predisposing conditions—most commonly CF (Chap. 313). A state of chronic colonization beginning early in childhood is seen in some Asian populations with chronic or diffuse panbronchiolitis, a disease of unknown etiology. P. aeruginosa is one of the organisms that colonizes damaged bronchi in bronchiectasis, a disease secondary to multiple causes in which profound structural abnormalities of the airways result in mucus stasis.
TREATMENT | CHRONIC RESPIRATORY TRACT INFECTIONS |
Optimal management of chronic P. aeruginosa lung infection has not been determined. Patients respond clinically to antipseudomonal therapy, but the organism is rarely eradicated. Because eradication is unlikely, the aim of treatment for chronic infection is to quell exacerbations of inflammation. The regimens used are similar to those used for pneumonia, but an aminoglycoside is almost always added because resistance is common in chronic disease. However, it may be appropriate to use an inhaled aminoglycoside preparation in order to maximize airway drug levels.
Endovascular Infections Infective endocarditis due to P. aeruginosa is a disease of IV drug users whose native valves are involved. This organism has also been reported to cause prosthetic valve endocarditis. Sites of prior native-valve injury due to the injection of foreign material such as talc or fibers probably serve as niduses for bacterial attachment to the heart valve. The manifestations of P. aeruginosa endocarditis resemble those of other forms of endocarditis in IV drug users except that the disease is more indolent than Staphylococcus aureus endocarditis. While most disease involves the right side of the heart, left-sided involvement is not rare and multivalvular disease is common. Fever is a common manifestation, as is pulmonary involvement (due to septic emboli to the lungs). Hence, patients may also experience chest pain and hemoptysis. Involvement of the left side of the heart may lead to signs of cardiac failure, systemic emboli, and local cardiac involvement with sinus of Valsalva abscesses and conduction defects. Skin manifestations are rare in this disease, and ecthyma gangrenosum is not seen. The diagnosis is based on positive blood cultures along with clinical signs of endocarditis.
TREATMENT | ENDOVASCULAR INFECTIONS |
(Table 189-2) It has been customary to use synergistic antibiotic combinations in treating P. aeruginosa endocarditis because of the development of resistance during therapy with a single antipseudomonal β-lactam agent. Which combination therapy is preferable is unclear, as all combinations have failed. Cases of P. aeruginosa endocarditis that relapse during or fail to respond to therapy are often caused by resistant organisms and may require surgical therapy. Other considerations for valve replacement are similar to those in other forms of endocarditis (Chap. 155).
Bone and Joint Infections P. aeruginosa is an infrequent cause of bone and joint infections. However, Pseudomonas bacteremia or infective endocarditis caused by the injection of contaminated illicit drugs has been documented to result in vertebral osteomyelitis and sternoclavicular joint arthritis. The clinical presentation of vertebral P. aeruginosa osteomyelitis is more indolent than that of staphylococcal osteomyelitis. The duration of symptoms in IV drug users with vertebral osteomyelitis due to P. aeruginosa varies from weeks to months. Fever is not uniformly present; when present, it tends to be low grade. There may be mild tenderness at the site of involvement. Blood cultures are usually negative unless there is concomitant endocarditis. The erythrocyte sedimentation rate (ESR) is generally elevated. Vertebral osteomyelitis due to P. aeruginosa has also been reported in the elderly, in whom it originates from urinary tract infections (UTIs). The infection generally involves the lumbosacral area because of a shared venous drainage (Batson’s plexus) between the lumbosacral spine and the pelvis. Sternoclavicular septic arthritis due to P. aeruginosa is seen almost exclusively in IV drug users. This disease may occur with or without endocarditis, and a primary site of infection often is not found. Plain radiographs show joint or bone involvement. Treatment of these forms of disease is generally successful.
Pseudomonas osteomyelitis of the foot most often follows puncture wounds through sneakers and mostly affects children. The main manifestation is pain in the foot, sometimes with superficial cellulitis around the puncture wound and tenderness on deep palpation of the wound. Multiple joints or bones of the foot may be involved. Systemic symptoms are generally absent, and blood cultures are usually negative. Radiographs may or may not be abnormal, but the bone scan is usually positive, as are magnetic resonance imaging (MRI) studies. Needle aspiration usually yields a diagnosis. Prompt surgery, with exploration of the nail puncture tract and debridement of the involved bones and cartilage, is generally recommended in addition to antibiotic therapy.
Central Nervous System (CNS) Infections CNS infections due to P. aeruginosa are relatively rare. Involvement of the CNS is almost always secondary to a surgical procedure or head trauma. The entity seen most often is postoperative or posttraumatic meningitis. Subdural or epidural infection occasionally results from contamination of these areas. Embolic disease arising from endocarditis in IV drug users and leading to brain abscesses has also been described. The cerebrospinal fluid (CSF) profile of P. aeruginosa meningitis is no different from that of pyogenic meningitis of any other etiology.
TREATMENT | CENTRAL NERVOUS SYSTEM INFECTIONS |
(Table 189-2) Treatment of Pseudomonas meningitis is difficult; little information has been published, and no controlled trials in humans have been undertaken. However, the general principles involved in the treatment of meningitis apply, including the need for high doses of bactericidal antibiotics to attain high drug levels in the CSF. The agent with which there is the most published experience in P. aeruginosa meningitis is ceftazidime, but other antipseudomonal β-lactam drugs that reach high CSF concentrations, such as cefepime and meropenem, have also been used successfully. Other forms of P. aeruginosa CNS infection, such as brain abscesses and epidural and subdural empyema, generally require surgical drainage in addition to antibiotic therapy.
Eye Infections Eye infections due to P. aeruginosa occur mainly as a result of direct inoculation into the tissue during trauma or surface injury by contact lenses. Keratitis and corneal ulcers are the most common types of eye disease and are often associated with contact lenses (especially the extended-wear variety). Keratitis can be slowly or rapidly progressive, but the classic description is disease progressing over 48 h to involve the entire cornea, with opacification and sometimes perforation. P. aeruginosa keratitis should be considered a medical emergency because of the rapidity with which it can progress to loss of sight. P. aeruginosa endophthalmitis secondary to bacteremia is the most devastating of P. aeruginosa eye infections. The disease is fulminant, with severe pain, chemosis, decreased visual acuity, anterior uveitis, vitreous involvement, and panophthalmitis.
TREATMENT | EYE INFECTIONS |
(Table 189-2) The usual therapy for keratitis is the administration of topical antibiotics. Therapy for endophthalmitis includes the use of high-dose local and systemic antibiotics (to achieve higher drug concentrations in the eye) and vitrectomy.
Ear Infections P. aeruginosa infections of the ears vary from mild swimmer’s ear to serious life-threatening infections with neurologic sequelae. Swimmer’s ear is common among children and results from infection of moist macerated skin of the external ear canal. Most cases resolve with treatment, but some patients develop chronic drainage. Swimmer’s ear is managed with topical antibiotic agents (otic solutions). The most serious form of Pseudomonas infection involving the ear has been given various names: two of these designations, malignant otitis externa and necrotizing otitis externa, are now used for the same entity. This disease was originally described in elderly diabetic patients, in whom the majority of cases still occur. However, it has also been described in patients with AIDS and in elderly patients without underlying diabetes or immunocompromise. The usual presenting symptoms are decreased hearing and ear pain, which may be severe and lancinating. The pinna is usually painful, and the external canal may be tender. The ear canal almost always shows signs of inflammation, with granulation tissue and exudate. Tenderness anterior to the tragus may extend as far as the temporomandibular joint and mastoid process. A small minority of patients have systemic symptoms. Patients in whom the diagnosis is made late may present with cranial nerve palsies or even with cavernous venous sinus thrombosis. The ESR is invariably elevated (≥100 mm/h). The diagnosis is made on clinical grounds in severe cases; however, the “gold standard” is a positive technetium-99 bone scan in a patient with otitis externa due to P. aeruginosa. In diabetic patients, a positive bone scan constitutes presumptive evidence for this diagnosis and should prompt biopsy or empirical therapy.
TREATMENT | EAR INFECTIONS |
(Table 189-2) Given the infection of the ear cartilage, sometimes with mastoid or petrous ridge involvement, patients with malignant (necrotizing) otitis externa are treated as for osteomyelitis.
Urinary Tract Infections UTIs due to P. aeruginosa generally occur as a complication of a foreign body in the urinary tract, an obstruction in the genitourinary system, or urinary tract instrumentation or surgery. However, UTIs caused by P. aeruginosa have been described in pediatric outpatients without stones or evident obstruction.
TREATMENT | URINARY TRACT INFECTIONS |
(Table 189-2) Most P. aeruginosa UTIs are considered complicated infections that must be treated longer than uncomplicated cystitis. In general, a 7- to 10-day course of treatment suffices, with up to 2 weeks of therapy in cases of pyelonephritis. Urinary catheters, stents, or stones should be removed to prevent relapse, which is common and may be due not to resistance but rather to factors such as a foreign body that has been left in place or an ongoing obstruction.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


