Periodic acid-Schiff without diastase has granular cytoplasmic staining
• Exuberant rich capillary network immediately adjacent to epithelium
• May have stellate scar that can be calcified
Ancillary Tests
• Immunohistochemical reactivity
Cytokeratin, α-inhibin, calponin, GLUT1, MUC6 (+)
• von Hippel-Lindau ( VHL ) gene alteration detected even in sporadic cases
Top Differential Diagnoses
• von Hippel-Lindau-associated pancreatic cysts
• Serous cystadenocarcinoma
• Pseudocyst
• Mucinous cystic neoplasm
• Metastatic clear cell renal cell carcinoma
Graphic Representation Sponge-like or “honeycomb” mass in the pancreatic head is shown. Note the presence of innumerable small cysts and central scar. The pancreatic duct is not obstructed.
Honeycomb Appearance Round, well-circumscribed mass is shown in the tail of the pancreas with compact, small, thin, smooth-walled cysts containing clear serous fluid. The cysts did not communicate with the pancreatic duct.
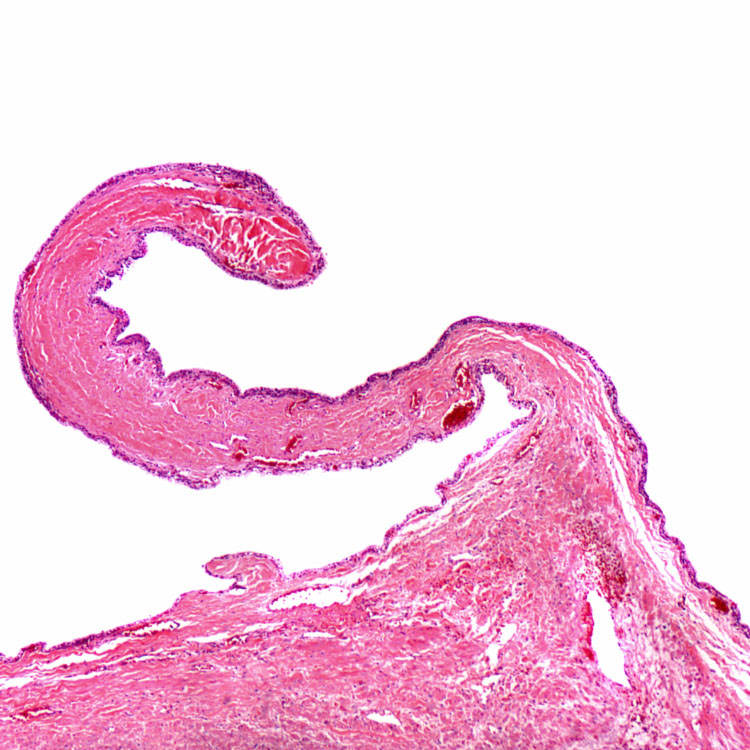
Flat Lining Epithelium The lining epithelium of the cyst is comprised of a single layer of epithelial cells that rests on a fibrous cyst wall.
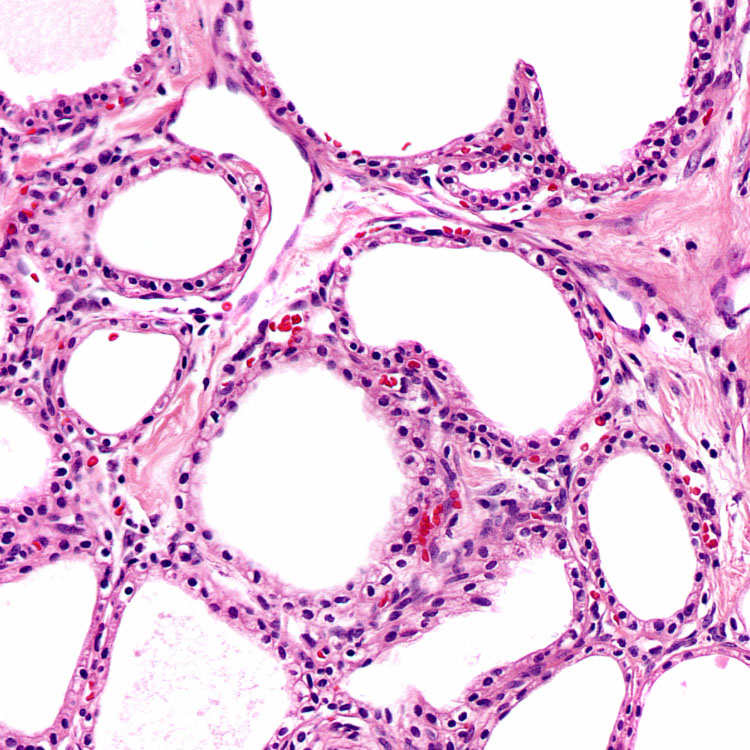
Multiloculated Appearance In its most typical presentation, serous cystadenoma is composed of multiple microcysts lined by bland cuboidal epithelium. The lining cells usually have pale cytoplasm. The presence of congested capillaries adjacent to the epithelial cells is a characteristic feature.
TERMINOLOGY
Abbreviations
• Serous cystadenoma (SCA)
Synonyms
• Serous microcystic adenoma
• Clear cell or glycogen-rich adenoma
Definitions
• Benign, cystic epithelial neoplasm
Presumably originates from centroacinar cell/intercalated duct system
ETIOLOGY/PATHOGENESIS
No Uniform Consensus on Cellular Origin
• Acinar, centroacinar, and ductal origins have all been considered
Some immunohistochemical and ultrastructural features suggest centroacinar cell origin
CLINICAL ISSUES
Epidemiology
• Incidence
10% of surgically resected cystic pancreatic lesions
• Age
Mean: 66 years; range: 18-91 years
Rarely reported in infants (oligocystic variant)
• Sex
F:M ratio ranges from 3:1 to 7:3
Site
• Anywhere in pancreas
Presentation
• 2/3 of patients: Abdominal mass &/or pain
Larger SCA (> 4 cm) more likely to give rise to symptoms
• 1/3 of patients: Asymptomatic, incidentally discovered
Treatment
• Surgical resection if symptomatic
Prognosis
• Excellent, recurs in < 2% of cases
IMAGING
Radiographic Findings
• Grayscale ultrasound and contrast-enhanced computed tomography are best imaging modalities
Well-defined mass
Microlacunae separated by delicate septa
– Enhancement of septa on computed tomography
Central stellate scar
– Echogenic area that may be calcified resulting in sunburst appearance on ultrasound
Only gold members can continue reading. Log In or Register to continue



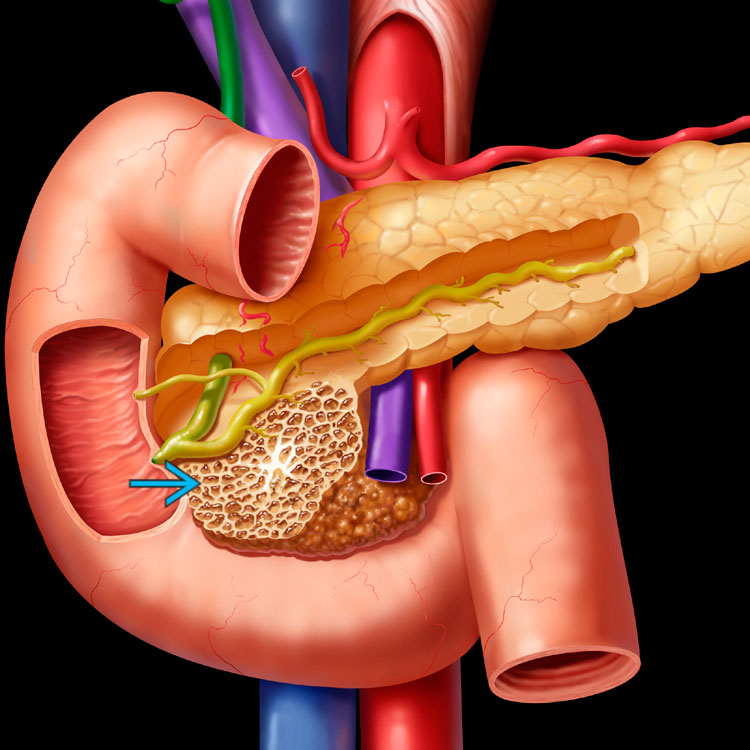
 is shown. Note the presence of innumerable small cysts and central scar. The pancreatic duct is not obstructed.
is shown. Note the presence of innumerable small cysts and central scar. The pancreatic duct is not obstructed.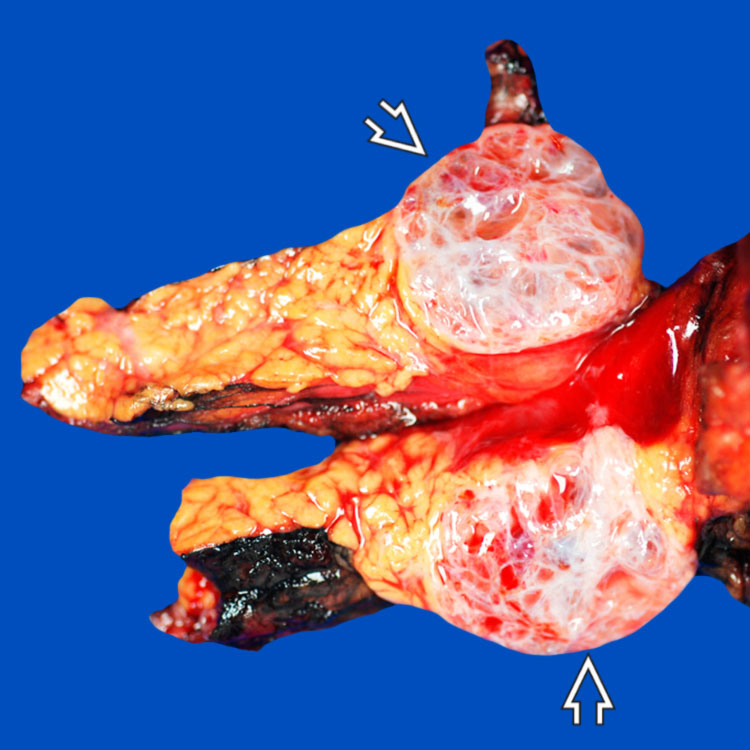
 is shown in the tail of the pancreas with compact, small, thin, smooth-walled cysts containing clear serous fluid. The cysts did not communicate with the pancreatic duct.
is shown in the tail of the pancreas with compact, small, thin, smooth-walled cysts containing clear serous fluid. The cysts did not communicate with the pancreatic duct.