Seborrheic Keratosis (and Variants)
Elsa F. Velazquez, MD
Key Facts
Macroscopic Features
Sharply delineated plaques with greasy appearance
Verruciform or flat surface
Surface shows characteristic keratotic plugs
From flesh-colored to brown-black
Darkly pigmented lesions may be clinically mistaken for melanoma
Microscopic Pathology
Exophytic/endophytic
Ortho-hyperkeratosis typically present
Composed of basaloid and squamoid cells
Horn cysts/pseudocysts
Squamous eddies may be present
Often pigmented
Stromal amyloid deposition may be seen
Variable degree of inflammation
Several variants have been described
Acanthotic
Papillomatous (hyperkeratotic)
Adenoid (reticulated)
Clonal (Borst-Jadassohn epithelioma)
Inverted follicular keratosis (irritated SK)
Lichenoid SK
Inflammatory
Desmoplastic
Adamantinoid
Overlapping features are common
Top Differential Diagnoses
Verruca vulgaris
Hidroacanthoma simplex
Hypertrophic actinic keratosis
Squamous cell carcinoma in situ
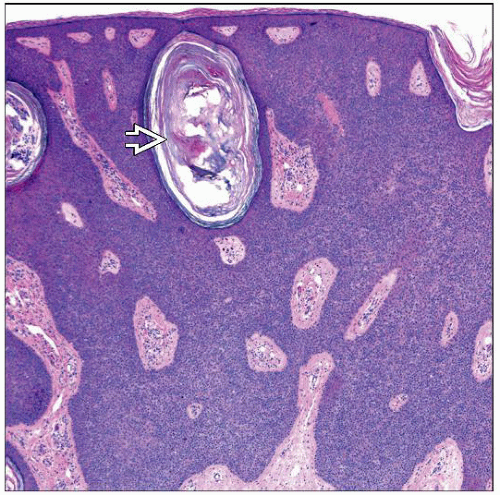 Seborrheic keratosis, acanthotic/endophytic variant. Note the smooth, rounded surface and thickened epithelium. The lesion is predominantly composed of basaloid cells with a prominent horn cyst  . . |
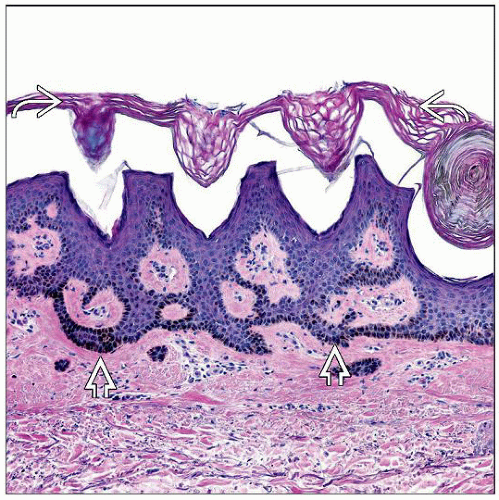 Adenoid seborrheic keratosis composed of narrow and hyperpigmented trabeculae  . This variant of SK often evolves from a solar lentigo. Note the “basket weave,” orthokeratotic surface . This variant of SK often evolves from a solar lentigo. Note the “basket weave,” orthokeratotic surface  . . |
TERMINOLOGY
Abbreviations
Seborrheic keratosis (SK)
Definitions
Benign epidermal proliferation
ETIOLOGY/PATHOGENESIS
Benign Epidermal Tumor
Monoclonal
Likely neoplasm rather than hyperplasia
CLINICAL ISSUES
Epidemiology
Incidence
Very common lesions
Age
Middle-aged and elderly
Affect approximately 20% of elderly population
Site
Most common on face, chest, and back
Unusual locations: Conjunctiva, areola, areas of cleavage
May be found anywhere except palms and soles
Presentation
Sharply delineated plaques with greasy appearance
Solitary or multiple
Measuring a few mm to a few cm
Verruciform or flat surface
Surface shows characteristic keratotic plugs
Soft and friable
Round or oval
From flesh-colored to brown-black
Darkly pigmented lesions may be clinically mistaken for melanoma
Often appearing as stuck on skin surface
Inverted follicular keratosis variant presents as warty papulonodule
Leser-Trélat sign
Sudden onset of multiple seborrheic keratoses
Usually associated with internal malignancies (most commonly gastric adenocarcinoma)
Prognosis
Excellent
MACROSCOPIC FEATURES
General Features
Exophytic tumors
Verruciform/warty or smooth surface
Size
A few mm to a few cm in diameter
Sections to Be Submitted
As lesions are small, they tend to be almost entirely sampled in most biopsies
Specimens may be bisected or serially sectioned before submission
Curettage specimens are received as multiple fragments
MICROSCOPIC PATHOLOGY
Histologic Features
Sharply defined tumors
Exophytic or endophytic or combination of both
Ortho-hyperkeratosis (“Van Gogh sky”)
Heavily inflamed, irritated, or infarcted SK may show foci of parakeratosis
Composed of bland-appearing basaloid and squamoid cells (variable amounts of each)
Keratin-filled invaginations and small pseudocysts (pseudohorn cysts) are characteristic
Nests of keratinocytes (squamous eddies) may be seen
Usually seen in irritated SK
Apparently related to acrotrichia
Frequently hyperpigmented
Pigmentation in SK has been linked to increased expression of keratinocyte-derived endothelin 1
Melanocytes may be increased in number and size
Melanoacanthomas are SKs with marked melanocytic proliferation and pigmentation
Tricholemmal differentiation (glycogen-rich) may be focally present
Sebaceous differentiation is uncommon and focal finding
Acantholysis &/or dyskeratosis may be rarely seen
Many different variants of SK have been described
Acanthotic SK
Smooth, rounded and ortho-hyperkeratotic surface
Acanthotic epithelium
Basaloid cells predominate over squamoid cells
Often pigmented
Horn cysts tend to be prominent
Papillomatous (keratotic) SK
Ortho-hyperkeratosis
Papillomatosis
Acanthosis
Squamoid cells predominate over basaloid cells
Prominent horn cysts
Adenoid (reticulated) SK
Ortho-hyperkeratosis
Flat or papillomatous surface
Thin proliferating strands emanating from epidermis
Basaloid cells predominate over squamoid cells
Often pigmented
Horn cysts are absent or sparse
Clonal SK (type of irritated SK)
Borst-Jadassohn phenomenon: Oval to round aggregates of intraepidermal keratinocytes
Inverted follicular keratosis (type of irritated SK)
Endophytic growth pattern
Prominent squamous eddies
Lichenoid SK
Prominent lymphoid infiltrate
Apoptotic cells (Civatte bodies)
Some cases probably evolve to lichenoid keratosis (lichen planus-like keratosis)
Any of the variants of SK may show lichenoid features
Inflammatory SK
Any variant of SK may be heavily inflamed
Rarely, neutrophils may be abundant in inflammatory infiltrate
Overlapping features with lichenoid SK
Desmoplastic SK
Irregular cords and strands of squamous cells surrounded by desmoplastic stroma
These trapped strands and cords may mimic infiltrative squamous cell carcinoma (SCC)
Bulk of lesion is typical SK
Analogous to desmoplastic tricholemmoma
Adamantinoid SK
Very unusual
Small basaloid keratinocytes with spindled cytoplasm
Intercellular mucin
SK with pseudorosettes
Very rare
Basaloid cells arranged around central small spaces
Overlapping features of different variants is common finding
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


