Patient Story
A 34-year-old woman with extensive papulopustular rosacea (Figures 113-1, 113-2, 113-3) has a history of easy facial flushing since her teen years. Her face has been persistently redder in the past 5 years and she is bothered by this. She acknowledges that her mom has similar redness in her face and that she is from northern European heritage. In the last 6 months, since her daughter was born, she has developed many “pimples.” Physical examination reveals papules, pustules, and telangiectasias. No comedones are seen. She knows that the sun makes it worse but finds that many sunscreens are irritating to her skin. The patient is started on oral tetracycline daily and 0.75% metronidazole cream to use once daily. She agrees to wear a hat and stay out of the sun during the middle of the day. She will continue to look for a sunscreen she can tolerate. She knows that precipitating factors for her include hot and humid weather, alcohol, hot beverages, and spicy foods. She will do her best to avoid those factors.



Introduction
Epidemiology
- Common in fair-skinned people of Celtic and northern European heritage.
- Women are more often affected than men.
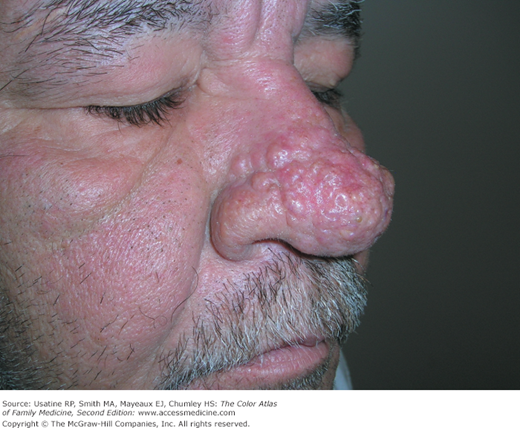
- Men are more prone to the extreme forms of hyperplasia, which causes rhinophymatous rosacea (Figures 113-4 and 113-5).

Etiology and Pathophysiology
- Although the exact etiology is unknown, the pathophysiology involves nonspecific inflammation followed by dilation around follicles and hyperreactive capillaries. These dilated capillaries become telangiectasias (Figures 113-6 and 113-7).
- As rosacea progresses, diffuse hypertrophy of the connective tissue and sebaceous glands ensues (Figures 113-4 and 113-5).
- Alcohol may accentuate erythema, but does not cause the disease. Rosacea runs in families.
- Sun exposure may precipitate an acute rosacea flare, but flare-ups can happen without sun exposure.
- A significant increase in the hair follicle mite Demodex folliculorum is sometimes found in rosacea.1 It is theorized that these mites play a role because they incite an inflammatory or allergic reaction by mechanical blockage of follicles.


Diagnosis
Rosacea has four stages or subtypes:
Erythematotelangiectatic rosacea (Figures 113-6 and 113-7)—This stage is characterized by frequent mild to severe flushing with persistent central facial erythema.

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


