Different clinical features: Multiple cutaneous lesions, may have joint &/or internal organ involvement in multicentric cutaneous reticulohistiocytosis
• Juvenile xanthogranuloma
• Langerhans cell histiocytosis
• Rosai-Dorfman disease (sinus histiocytosis with massive lymphadenopathy)
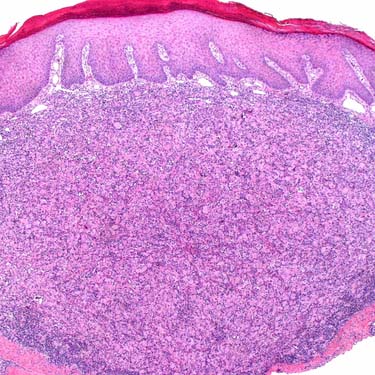
Solitary Reticulohistiocytoma at Low Magnification Low magnification shows a nodular dermal infiltrate composed of large, eosinophilic-staining histiocytic cells, associated with mixed inflammatory infiltrate, including many lymphocytes and eosinophils.
Solitary Reticulohistiocytoma Higher magnification shows a population of large histiocytic-appearing cells with dense, eosinophilic-staining cytoplasm , associated with an infiltrate, including many lymphocytes and eosinophils .
Solitary Reticulohistiocytoma at High Magnification High magnification shows the large, eosinophilic-staining histiocytic cells with dense, glassy cytoplasm and focal emperipolesis of lymphocytes. Note the mixed background inflammatory infiltrate, including many eosinophils .
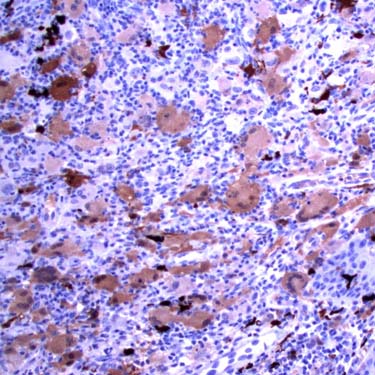
S100 Immunohistochemistry in Reticulohistiocytoma This case showed greater S100 staining than usual, although it is relatively weak and mostly cytoplasm. Entrapped dendritic cells show much stronger staining.
TERMINOLOGY
Synonyms
• Solitary cutaneous reticulohistiocytoma
• Reticulohistiocytic granuloma
• Giant cell reticulohistiocytoma
Definitions
• Proliferation of histiocytes with abundant dense, glassy-appearing eosinophilic cytoplasm
ETIOLOGY/PATHOGENESIS
Environmental Exposure
• May be related to stimuli, such as insect bites, infection, trauma, or ruptured folliculitis or cyst in some cases
CLINICAL ISSUES
Epidemiology
• Incidence
Rare tumor
• Age
Usually occurs in adults > 40 years old
– However, some cases have been reported in adolescents
• Sex
M:F = 1:1
• Ethnicity
Most cases occur in Caucasians
Site
• Usually head and neck region, including mucosal sites
However, may present at almost any cutaneous site
Presentation
• Skin papule or nodule
Usually single lesion, but several may be present in some cases
• Firm, rapidly growing lesion
• Usually appear as red-brown or yellow-brown
• May be preceded by trauma in some cases
• Lack of systemic symptoms, including fever, weight loss, or weakness (which may be seen in multicentric reticulohistiocytosis)
Treatment
• Surgical approaches
Complete conservative excision is curative
– Usually not required, unless lesion is very large or fails to resolve
Prognosis
• Excellent; lesions often involute spontaneously
• No definite relationship with more aggressive multicentric reticulohistiocytosis
However, multiple skin lesions should suggest possibility of generalized cutaneous reticulohistiocytosis
MACROSCOPIC
General Features
• Dermal-based, nodular, well-circumscribed, but unencapsulated, lesion
Size
• Lesions typically range in size from 0.5-2.0 cm
MICROSCOPIC
Histologic Features
• Dermal-based nodular proliferation of large mononuclear and multinucleated histiocytes
Cells show characteristic abundant glassy/hyalinized-appearing eosinophilic cytoplasm
Some cells may show finely granular cytoplasm
Occasional Touton-type giant cells containing lipid may be present but not prominent
Cytologic atypia is usually minimal, and mitoses are few and nonatypical
No infiltrative features are present
• Overlying epidermis may show atrophy/thinning
Often grenz zone separating infiltrate from epidermis
Only gold members can continue reading. Log In or Register to continue
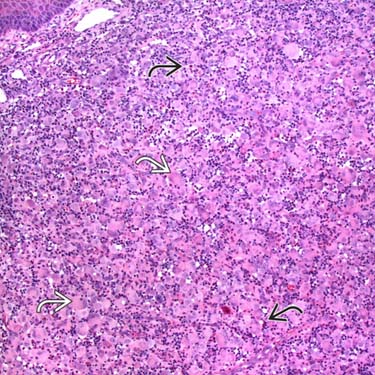
 , associated with an infiltrate, including many lymphocytes and eosinophils
, associated with an infiltrate, including many lymphocytes and eosinophils  .
.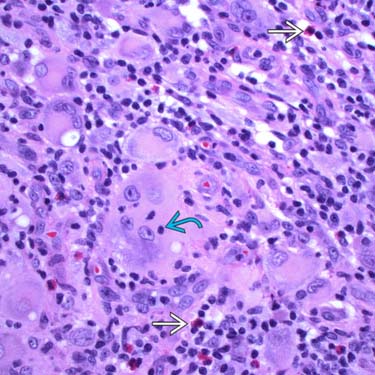
 of lymphocytes. Note the mixed background inflammatory infiltrate, including many eosinophils
of lymphocytes. Note the mixed background inflammatory infiltrate, including many eosinophils  .
.