Reticulohistiocytoma
David S. Cassarino, MD, PhD
Key Facts
Terminology
Proliferation of histiocytes with abundant dense, glassy-appearing eosinophilic cytoplasm
Clinical Issues
Usually occurs in adults > 40 years old, but cases have been reported in adolescents
Usually head and neck region, including mucosal sites, but may present at any cutaneous site
Usually red-brown or yellow-brown appearing
Microscopic Pathology
Dermal-based nodular proliferation of large mononuclear and multinucleated histiocytes
Cells show characteristic abundant glassy/hyalinized-appearing eosinophilic cytoplasm
Occasional Touton-type giant cells containing lipid may be present
Early lesions characterized by more mononuclear cells with lymphocytes
Ancillary Tests
Cells typically are typically positive for CD68 (KP1), CD163, and lysozyme
Top Differential Diagnoses
Multicentric reticulohistiocytosis and generalized cutaneous reticulohistiocytosis
Juvenile xanthogranuloma (JXG)
Langerhans cell histocytosis (LCH)
Rosai-Dorfman disease (sinus histiocytosis with massive lymphadenopathy)
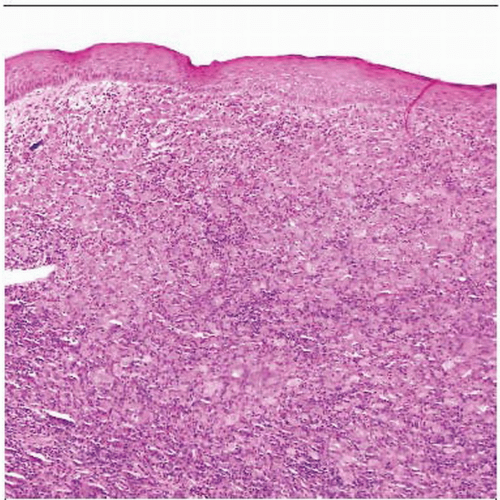 Low-power examination shows a dense nodular to sheetlike collection of large histiocytic cells in the dermis. |
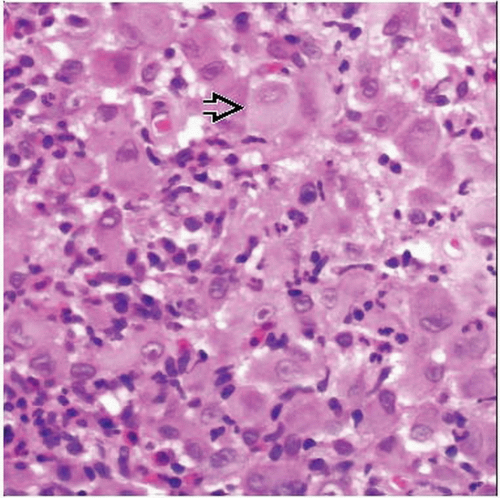 High-power view shows large histiocytic cells with abundant dense, glassy-appearing cytoplasm  and a background inflammatory infiltrate containing neutrophils and eosinophils. and a background inflammatory infiltrate containing neutrophils and eosinophils. |
TERMINOLOGY
Synonyms
Solitary cutaneous reticulohistiocytoma (SCR)
Reticulohistiocytic granuloma
Giant cell reticulohistiocytoma
Definitions
Proliferation of histiocytes with abundant dense, glassy-appearing, eosinophilic cytoplasm
ETIOLOGY/PATHOGENESIS
Environmental Exposure
May be related to stimuli, such as insect bites, infection, trauma, or ruptured folliculitis or cyst
CLINICAL ISSUES
Epidemiology
Incidence
Rare tumor
Age
Usually occurs in adults > 40 years old
However, some cases have been reported in adolescents
Gender
Equal male and female incidence
Ethnicity
Most cases occur in Caucasians
Site
Usually head and neck region, including mucosal sites
However, may present at any cutaneous site
Presentation
Skin papule or nodule
Usually single lesion, but several may be present in some cases
Firm, rapidly growing lesion
Usually appear as red-brown or yellow-brown
May be preceded by trauma in some cases
Lack of systemic symptoms, including fever, weight loss, or weakness (which may be seen in multicentric reticulohistiocytosis)
Treatment
Surgical approaches
Complete conservative excision is curative
Usually not required unless lesion is very large or fails to resolve
Prognosis
Excellent; lesions often involute spontaneously
No definite relationship with more aggressive multicentric reticulohistiocytosis
However, multiple skin lesions should suggest possibility of generalized cutaneous reticulohistiocytosis
MACROSCOPIC FEATURES
General Features
Dermal-based, nodular, well-circumscribed but unencapsulated lesion
Size
Lesions typically range in size from 0.5-2 cm
MICROSCOPIC PATHOLOGY
Histologic Features
Dermal-based nodular proliferation of large mononuclear and multinucleated histiocytes
Cells show characteristic abundant glassy/hyalinized-appearing eosinophilic cytoplasm
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


