• RN/LGDN: Plates 1-2 cells thick, portal tracts present, no architectural or cytologic atypia
• HGDN: Plates focally up to 3 cells thick; small cell change with increased nuclear:cytoplasmic ratio
Unpaired arterioles and pseudoacinar architecture can be present
• Reticulin is preserved
May be focally lost in HGDN
Top Differential Diagnoses
• Small cell change, high nuclear:cytoplasmic ratio, pseudoacinar architecture, and unpaired arterioles favor HGDN over LGDN
• Uniformly thick plates (> 3 cells) are most important feature distinguishing HCC from HGDN
Prominent pseudoacinar architecture, numerous unpaired arterioles, and loss or fragmentation of reticulin favor HCC
• Stromal invasion distinguishes early HCC from HGDN
Lack of CK7(+) ductular reaction is useful in demonstrating stromal invasion
• Positive results with 2 out of 3 markers (GPC, GS, HSP70) favor HCC
Small Cell Change Small cell change (left 2/3 of image) is characterized by small cells with high nuclear:cytoplasmic ratio leading to increased cell density. When present in a nodule, it is the hallmark of high-grade dysplastic nodule (HGDN).
Large Cell Change Large cell change is characterized by large hyperchromatic nuclei but preserved nuclear:cytoplasmic ratio . This change is thought to be degenerative and not preneoplastic.
Large RN Large regenerative nodules (RNs) resemble other cirrhotic nodules but are > 1 cm. Ductular reaction is usually present at the interface of the nodule with the fibrous septa.
RN: Reticulin Stain Regenerative nodule containing a portal tract and an intact reticulin framework is shown. These features and the absence of cytoarchitectural atypia distinguish it from dysplastic nodule and hepatocellular carcinoma (HCC).




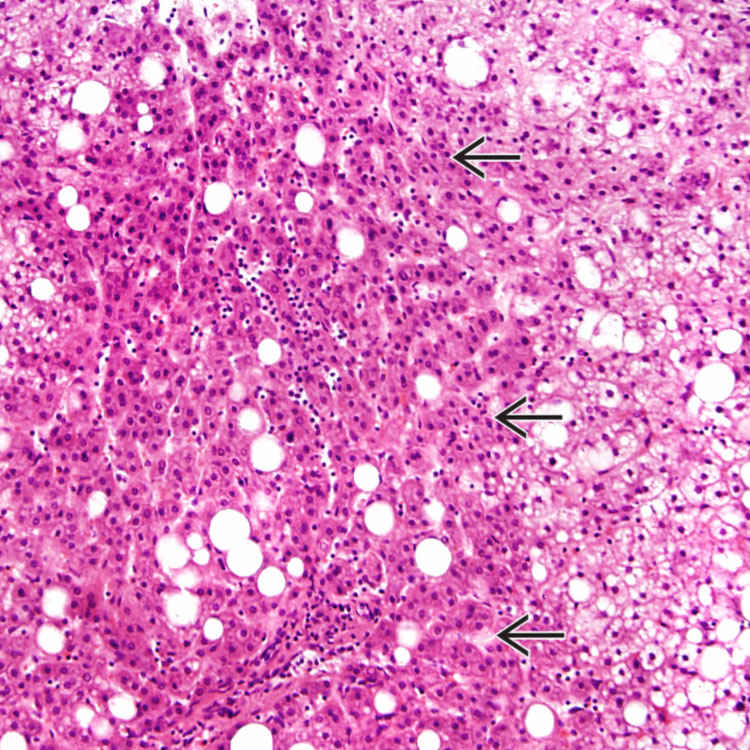
 is characterized by small cells with high nuclear:cytoplasmic ratio leading to increased cell density. When present in a nodule, it is the hallmark of high-grade dysplastic nodule (HGDN).
is characterized by small cells with high nuclear:cytoplasmic ratio leading to increased cell density. When present in a nodule, it is the hallmark of high-grade dysplastic nodule (HGDN).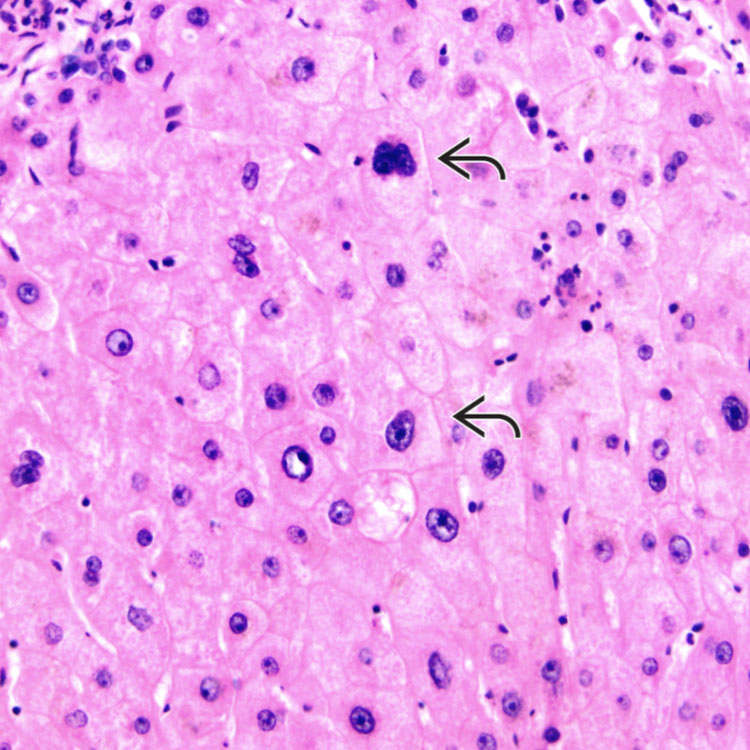
 . This change is thought to be degenerative and not preneoplastic.
. This change is thought to be degenerative and not preneoplastic.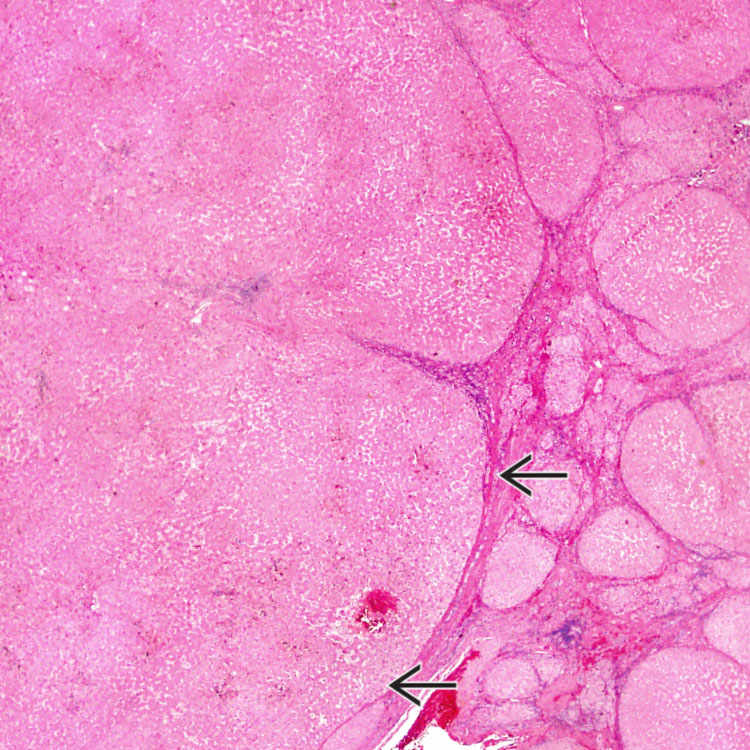
 resemble other cirrhotic nodules but are > 1 cm. Ductular reaction is usually present at the interface of the nodule with the fibrous septa.
resemble other cirrhotic nodules but are > 1 cm. Ductular reaction is usually present at the interface of the nodule with the fibrous septa.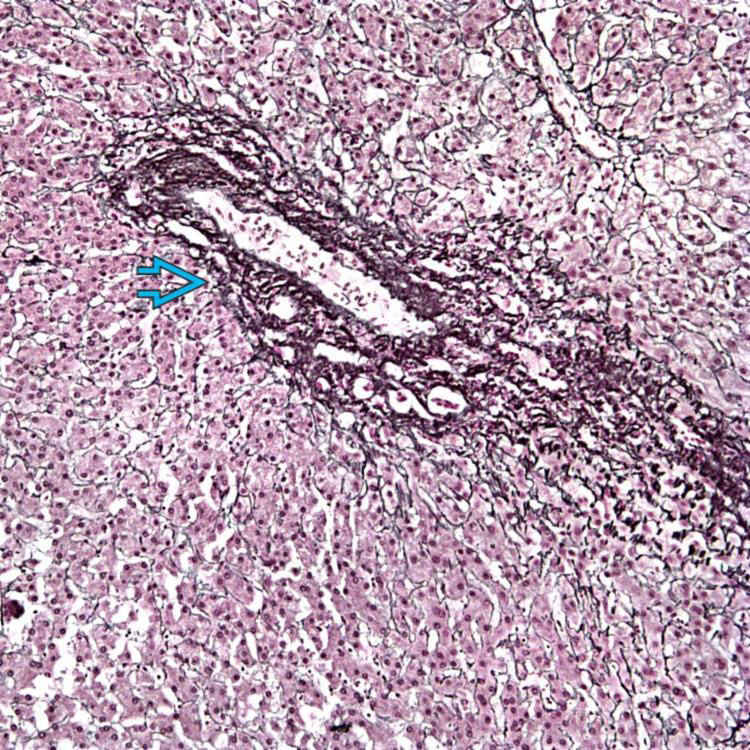
 and an intact reticulin framework is shown. These features and the absence of cytoarchitectural atypia distinguish it from dysplastic nodule and hepatocellular carcinoma (HCC).
and an intact reticulin framework is shown. These features and the absence of cytoarchitectural atypia distinguish it from dysplastic nodule and hepatocellular carcinoma (HCC).



 Large hepatocytes with nuclear enlargement, hyperchromasia, prominent nucleoli, often multinucleated
Large hepatocytes with nuclear enlargement, hyperchromasia, prominent nucleoli, often multinucleated













