Patient Story
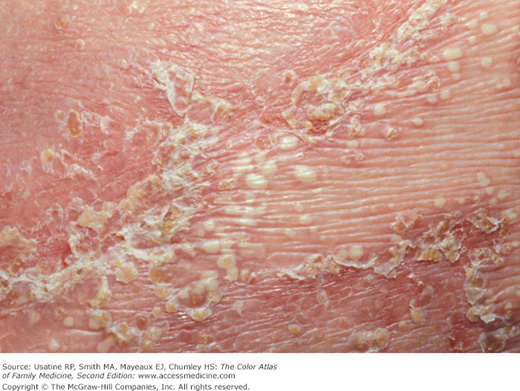
A 33-year-old woman presents with uncontrolled psoriasis for 20 years. In addition to the plaque psoriasis (Figure 152-1), she has inverse psoriasis (Figure 152-2). Topical ultrahigh-potency steroids and topical calcipotriol have not controlled her psoriasis. The options for phototherapy and systemic therapy were discussed. The patient chose to try narrowband UVB treatment in addition to her topical therapy.

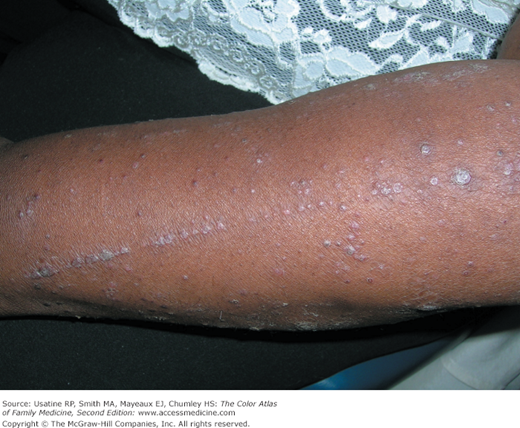
Figure 152-2

Inverse psoriasis in the inframammary folds of the patient in Figure 152-1. This is not a Candida infection. (Courtesy of Richard P. Usatine, MD.)
Introduction
Psoriasis is a chronic inflammatory papulosquamous and immune-mediated skin disorder. It is also associated with joint and cardiovascular comorbidities. Psoriasis can present in many different patterns from the scalp to the feet and cause psychiatric distress and physical disabilities. It is crucial to be able to identify psoriasis in all its myriad presentations so that patients receive the best possible treatments to improve their quality of life and avoid comorbidities.
Epidemiology
Psoriasis affects approximately 2% of the world population.1 The prevalence of psoriasis was 2.5% in white patients and was 1.3% in African American patients in one population study in the United States.2
- Sex—No gender preference.
- Age—Psoriasis can begin at any age. In one population study of the age of onset of psoriasis two peaks were revealed, one occurring at the age of 16 years (female) or 22 years (males) and a second peak at the age of 60 years (female) or 57 years (males).3
Etiology and Pathophysiology
- Immune-mediated skin disease, where the T cell plays a pivotal role in the pathogenesis of the disease.
- Langerhans cell (antigen-presenting cells in the skin) migrate from the skin to regional lymph nodes, where they activate T cells that migrate to the skin and release cytokines.
- Cytokines are responsible for epidermal and vascular hyperproliferation and proinflammatory effects.
Risk Factors
|
- Family history of psoriasis (odds ratio [OR] = 33.96; 95% confidence interval [CI] 14.14 to 81.57)
- Change in work conditions (OR = 8.34; 95% CI = 1.86 to 37.43)
- Divorce (OR = 5.69; 95% CI = 2.26 to 14.34)
- Urban dwellers (OR = 3.61; 95% CI = 0.99 to 13.18)
- Alcohol consumption (OR = 2.55; 95% CI = 1.26 to 5.17)
- Environmental tobacco smoke at home (OR = 2.29; 95% CI = 1.12 to 4.67)
Diagnosis
Psoriasis has many forms and locations. These nine categories were used to describe psoriasis in a consensus statement of the American Academy of Dermatology (AAD):6
Plaque (80% to 90% of patients with psoriasis) (Figures 152-1 and 152-3).
Scalp psoriasis (Figure 152-4).
Guttate psoriasis (Figure 152-5).
Inverse psoriasis (Figures 152-2 and 152-6).
Palmar-plantar psoriasis (Figure 152-7). Also known as palmoplantar psoriasis.
Erythrodermic psoriasis (Figure 152-8).
Pustular psoriasis—localized and generalized (Figure 152-9).
Nail psoriasis (Figure 152-10) (see Chapter 195, Psoriatic Nails).
Psoriatic arthritis (Figure 152-11).


Figure 152-5


Two cases of guttate psoriasis that started 2 weeks after strep pharyngitis. A. Note the typical drop-like (guttate) lesions on the arm of this 11-year-old girl. B. The salmon patches of guttate psoriasis in a 7-year-old boy with prominent neck, ear, and scalp involvement. (Courtesy of Richard P. Usatine, MD.)

Figure 152-7


A. Palmoplantar psoriasis with pustulosis that started 3 months ago on the hands of a 62-year-old woman. B. Note the erythema, scale, brown macules (mahogany spots), and pustules that are typical of this condition. This is considered to be a localized form of pustular psoriasis. (Courtesy of Richard P. Usatine, MD.)



Typical distribution in general: elbows, knees, extremities, trunk, scalp, face, ears, hands, feet, genitalia and intertriginous areas, and nails. Table 152-2 provides percentages for the most common locations of lesions in patients with psoriasis.
Location | % of Psoriasis Patients |
|---|---|
Scalp | 80 |
Elbows | 78 |
Legs | 74 |
Knees | 57 |
Arms | 54 |
Trunk | 53 |
Lower part of the body | 47 |
Base of the back | 38 |
Palms and soles | 12 |
- White scale on an erythematous raised base with well-demarcated borders (Figures 152-1 and 152-3).
- Silvery scale with hyperpigmentation may be seen in patients with darker skin (Figures 152-12 and 152-13).
- Plaques can be appear in different colors including hypopigmented (Figure 152-14) and silvery gray (Figure 152-15). A tricolored presentation occurs when the inflammation leads to leukoderma (Figure 152-16).
- The thickness and extent of the scale is variable (Figure 152-15).
- Positive Auspitz sign in which the peeling of the scale produces pinpoint bleeding on the plaque below.
- Typical distribution includes the elbows and knees and other extensor surfaces. The plaques can be found from head to toe including the penis (Figure 152-17).
- Plaques tend to be symmetrically distributed.
- Plaques can be annular with central clearing (Figure 152-18).
- When plaques occur at a site of injury, it is known as the Koebner phenomenon (Figure 152-19).







- Plaque on the scalp that may be seen at the hairline and around the ears (Figure 152-4).
- The thickness and extent of the plaques are variable as seen in plaque psoriasis.
- Small round plaques that resemble water drops (guttate means like a water drop) (Figure 152-20).
- Classically described as occurring after strep pharyngitis or another bacterial infection. This is one type of psoriasis that occurs in childhood.
- Typical distribution: the trunk and extremities but may include the face and neck (Figure 152-21).



- Found in the intertriginous areas of the axilla, groin, inframammary folds, and intergluteal fold (Figures 152-2, 152-6, and 152-22). It can also be seen below the pannus or within adipose folds in obese individuals.
- The term inverse refers to the fact that the distribution is not on extensor surfaces but in areas of body folds.
- Morphologically the lesions have little to no visible scale.
- Color is generally pink to red but can be hyperpigmented in dark-skinned individuals.

- Psoriasis that occurs on the plantar aspects of the hands and feet (palms and soles) (Figure 152-23). The psoriasis can also be seen on other parts of the hands and feet.
- Patients with this type of psoriasis often experience severe foot and hand pain that can impair walking and other daily activities of living. Hand involvement can result in pain with many types of work.
- Morphologically this can be plaque-like, vesicular, or pustular (Figure 152-24). Brown spots may be present as macules or flat papules. These are called mahogany spots and although they are not always present, they are characteristic of palmar-plantar psoriasis. Exfoliation of the skin can occur on the palms and soles.
Figure 152-23

Palmar-plantar psoriasis that was biopsy proven. Note the widespread erythema and scale that could be mistaken for tinea pedis and tinea manus. The patient does not have pustules or mahogany spots but those lesions are often not present in palmar-plantar psoriasis. (Courtesy of Richard P. Usatine, MD.)

- Erythrodermic psoriasis is widespread and erythematosus covering most of the skin (Figure 152-25).
- Morphologically, it can have plaques and erythema or the erythroderma can appear with the desquamation of pustular psoriasis.
- Widespread distribution can impair the important functions of the skin and this can be a dermatologic urgency requiring hospitalization and IV fluids. Chills, fever, tachycardia, and orthostatic hypotension are all signs that the patient may need hospitalization.

- Pustular psoriasis comes in localized and generalized types. One example of the local type is pustular psoriasis on the feet (Figure 152-24

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


