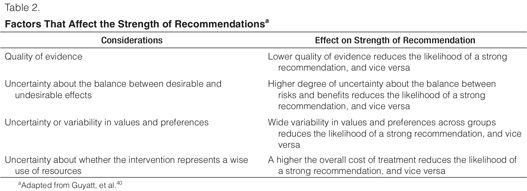
Subcommittees collectively reviewed the evidence profiles for each question, and using a nominal group technique, determined the overall quality of evidence (for both descriptive and actionable questions), the strength of recommendation (for actionable questions only), and drafted evidence summaries for review by other task force members. The strength of recommendations was defined as either strong (1) or weak (2), and either for (+) or against (–) an intervention, based on both the quality of evidence and the risks and benefits across all critical outcomes (Table 2).41,42 A no recommendation (0) could also be made due to either a lack of evidence or a lack of consensus among subcommittee members. Consensus statements based on expert opinion alone were not used when evidence could not support a recommendation. A strong recommendation either in favor of (+1) or against (–1) an intervention implied that the majority of task force members believed that the benefits of the intervention significantly outweighed the risks (or vice versa) and that the majority of patients and providers would pursue this course of action (or not), given the choice. A weak recommendation either in favor of (+2) or against (–2) an intervention implied that the benefits of the intervention likely outweighed the risks (or vice versa), but that task force members were not confident about these trade-offs, either because of a low quality of evidence or because the trade-offs between risks and benefits were closely balanced. On the basis of this information, most people might pursue this course of action (or not), but a significant number of patients and providers would choose an alternative course of action.40,43,44 Throughout these guidelines, for all strong recommendations, the phrase “We recommend …” was used, and for all weak recommendations, “We suggest …” was used.
Group consensus for all statements and recommendations was achieved using a modified Delphi method with an anonymous voting scheme.41,45 Task force members reviewed the subcommittees’ GRADE Evidence Summaries, and statements and recommendations, and voted and commented anonymously on each statement and recommendation using an on-line electronic survey tool (E-Survey, http://www.esurvey.com, Scottsdale, AZ). Consensus on the strength of evidence for each question required a majority (> 50%) vote. Consensus on the strength of recommendations was defined as follows: a recommendation in favor of an intervention (or the comparator) required at least 50% of all task force members voting in favor, with less than 20% voting against; failure to meet these voting thresholds resulted in no recommendation being made. For a recommendation to be graded as strong rather than weak, at least 70% of those voting had to vote for a strong recommendation, otherwise it received a weak recommendation. This method for reaching consensus has been proposed by the GRADE Working Group and was adopted by the 2008 Sepsis Guidelines Panel to ensure fairness, transparency, and anonymity in the creation of guideline recommendations.46,47 Polling results and comments were then summarized and distributed to all PAD guideline task force members for review. When one round of voting failed to produce group consensus, additional discussion and a second and/or third round of voting occurred. Polling for all questions was completed by December 2010. Distribution of the final voting tallies along with comments by task force members for each statement and recommendation is summarized in Supplemental Digital Content 2 (http://links.lww.com/CCM/A591).
Task force members completed required, annual, conflict of interest statements. Those with significant potential conflicts of interest (e.g., manuscript coauthorship) recused themselves from reviewing and grading evidence and from developing a subcommittee’s evidence statements and recommendations for related questions. All task force members voted anonymously on the final strength of evidence and strength of recommendations for all questions. No industry funding or support was used to develop any aspect of these guidelines.
Psychometric Analyses. These guidelines include statements and recommendations about using a variety of bedside behavioral assessment tools used to 1) detect and evaluate pain, 2) assess depth of sedation and degree of agitation, and 3) detect delirium in critically ill adult patients who are unable to communicate clearly. To date, a comparative assessment of the psychometric properties (i.e., reliability and validity) and feasibility related to the use of these tools in ICU patients has not been published. Scale reliability refers to the overall accuracy of the use of a scale in replicating pain, sedation, or delirium scores over time (i.e., test–retest reliability) or between raters (i.e., inter-rater reliability).48 Validity refers to the conclusions that can be drawn from the results of a test or scale (e.g., does a delirium assessment tool actually detect delirium?).49 Content, criterion, and discriminant validation are specific strategies of validity testing. A tool can be shown to be both reliable and valid when used for a specific purpose with specified individuals in a given context.48,49 Feasibility refers to the ease with which clinicians can apply a particular scale in the clinical setting (e.g., in the ICU).
The task force evaluated and compared the psychometric properties of behavioral pain scales (BPSs) used in adult ICU patients and compared their analyses to a previously published process.50 Similar scoring systems were not available to evaluate and compare the psychometric properties of sedation and delirium scales, which have different validation strategies from those used for pain scales. With input from three psychometric testing experts (D.S., C.J., C.W.), the task force developed similar scoring systems to assess and compare sedation and delirium scales.48
The psychometric properties of pain, sedation, and delirium scales were evaluated based on: 1) item selection and content validation, 2) reliability, 3) validity, 4) feasibility, and 5) relevance or impact of implementation on patient outcomes. Psychometric raw scores ranged from 0 to 25 for pain scales, 0 to 18 for sedation scales, and 0 to 21 for delirium scales. Weighted scores were established for each criterion to address variations in scores and to facilitate the interpretation of results, resulting in a total weighted score 0 to 20 for all three domains. The details of each of the three psychometric scoring systems used are summarized in Supplemental Digital Content 3 (http://links.lww.com/CCM/A592). Scales with weighted scores ranging from 15 to 20 had very good psychometric properties, 12 to 14.9 had moderate psychometric properties, 10 to 11.9 had some acceptable psychometric properties which required validation in additional studies, and 0 to 9.9 had very few psychometric properties reported and/or unacceptable results. Scales with moderate to very good psychometric properties (i.e., weighted score ≥ 12) were considered to be sufficiently valid and reliable scales for use in adult ICU patients. The quality of evidence for each individual scale was also evaluated using categories similar to those used in the GRADE system, with modifications adapted for the psychometric analyses. All studies were reviewed, and all scales were scored independently by two reviewers.
Pain and Analgesia. Incidence of pain in ICU patients. The International Association for the Study of Pain defines pain as an “unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage.”51 This definition highlights the subjective nature of pain and suggests that it can be present only when reported by the person experiencing it. Most critically ill patients will likely experience pain sometime during their ICU stay52 and identify it as a great source of stress.53–56 However, many critically ill patients may be unable to self-report their pain (either verbally or with other signs) because of an altered level of consciousness, the use of mechanical ventilation, or high doses of sedative agents or neuromuscular blocking agents.57 Yet, the ability to reliably assess patient’s pain is the foundation for effective pain treatment. As the International Association for the Study of Pain also states, “the inability to communicate verbally does not negate the possibility that an individual is experiencing pain and is in need of appropriate pain-relieving treatment.”58 Therefore, clinicians must be able to reliably detect pain, using assessment methods adapted to a patient’s diminished communication capabilities. In such situations, clinicians should consider patients’ behavioral reactions as surrogate measures of pain, as long as their motor function is intact.59 Detection, quantification, and management of pain in critically ill adults are major priorities and have been the subject of research for over 20 yr.60 Despite this fact, the incidence of significant pain is still 50% or higher in both medical and surgical ICU patients.61,62
In addition to experiencing pain at rest61 and pain related to surgery, trauma, burns, or cancer, patients also experience procedural pain.63–70 This was highlighted in the first practice guideline published on acute pain management 20 yr ago by the Agency for Health Care Policy and Research.71 Pain related to procedures is ubiquitous, and inadequate treatment of procedural pain remains a significant problem for many ICU patients.68
The negative physiologic and psychological consequences of unrelieved pain in ICU patients are significant and long-lasting. For many years, ICU patients have identified pain as their greatest concern and a leading cause of insufficient sleep.72 More recently, studies on ICU-discharged but still-hospitalized patients showed that 82% (n = 75)56 remembered pain or discomfort associated with the endotracheal tube and 77% (n = 93) remembered experiencing moderate to severe pain during their ICU stay.73 One week after discharge from the ICU, 82% (n = 120) of cardiac surgery patients reported pain as the most common traumatic memory of their ICU stay; 6 months later, 38% still recalled pain as their most traumatic ICU memory.74 Granja and colleagues75 noted that 17% (n = 313) of patients remembered experiencing severe pain 6 months after an ICU stay and 18% were at high risk of developing posttraumatic stress disorder (PTSD). Schelling and colleagues25 conducted a long-term follow-up (median, 4 yr) questionnaire study of 80 patients who had been treated in the ICU for acute respiratory distress syndrome. In comparison with normal controls, both medical and surgical patients who recalled pain and other traumatic situations while in the ICU had a higher incidence of chronic pain (38%) and PTSD symptoms (27%), and a lower health-related quality of life (21%).
The stress response evoked by pain can have deleterious consequences for ICU patients. Increased circulating catecholamines can cause arteriolar vasoconstriction, impair tissue perfusion, and reduce tissue-oxygen partial pressure.76 Other responses triggered by pain include catabolic hypermetabolism resulting in hyperglycemia, lipolysis, and breakdown of muscle to provide protein substrate.77 Catabolic stimulation and hypoxemia also impair wound healing and increase the risk of wound infection. Pain suppresses natural killer cell activity,78,79 a critical function in the immune system, with a decrease in the number of cytotoxic T cells and a reduction in neutrophil phagocytic activity.80 Acute pain may be the greatest risk factor for developing debilitating chronic, persistent, often neuropathic pain.81 Unrelieved acute pain in adult ICU patients is ubiquitous and far from benign, with both short- and long-term consequences. Adequately identifying and treating pain in these patients require focused attention.
Pain assessment in ICU patients. Treating pain in critically ill patients depends on a clinician’s ability to perform a reproducible pain assessment and to monitor patients over time to determine the adequacy of therapeutic interventions to treat pain. A patient’s self-report of pain is considered the “gold standard,” and clinicians should always attempt to have a patient rate his or her own pain first. Chanques and colleagues82 demonstrated that a 0–10 visually enlarged horizontal numeric rating scale was the most valid and feasible of five pain intensity rating scales tested in over 100 ICU patients. Yet when critically ill patients are unable to self-report their pain, clinicians must use structured, valid, reliable, and feasible tools to assess patients’ pain.83 It is essential that pain in ICU patients be assessed routinely and repetitively in a manner that is efficient and reproducible. No objective pain monitor exists, but valid and reliable bedside pain assessment tools that concentrate primarily on patients’ behaviors as indicators of pain do exist.
Although reviews of behavioral pain assessment tools have been published, an updated discussion is needed about their development, validation, and applicability to ICU patients.50,84 A detailed, systematic review of the processes of item selection and psychometric properties of pain scales (i.e., validity and reliability) may encourage clinicians to adopt pain scales and to standardize their use in ICU patients. Recent studies have demonstrated that implementing behavioral pain scales improves both ICU pain management and clinical outcomes, including better use of analgesic and sedative agents and shorter durations of mechanical ventilation and ICU stay.2,3,85
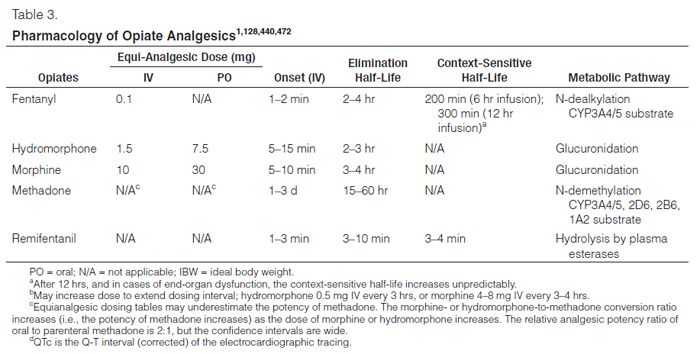
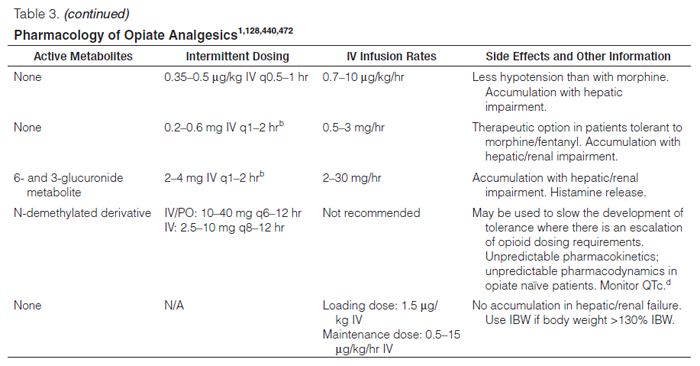
Treatment of pain. Opioids, such as fentanyl, hydromorphone, methadone, morphine, and remifentanil, are the primary medications for managing pain in critically ill patients (Table 3).62 The optimal choice of opioid and the dosing regimen used for an individual patient depends on many factors, including the drug’s pharmacokinetic and pharmacodynamic properties.52 The use of meperidine is generally avoided in ICU patients because of its potential for neurologic toxicity.52
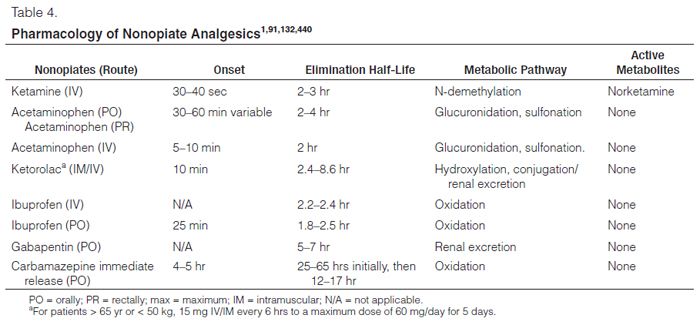
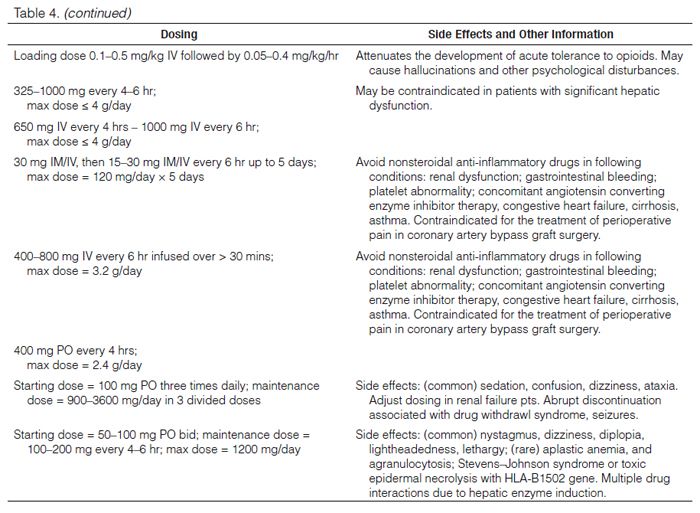
Several other types of analgesics or pain-modulating medications, such as local and regional anesthetics (e.g., bupivacaine), nonsteroidal anti-inflammatory medications (e.g., ketorolac, ibuprofen), IV acetaminophen, and anticonvulsants, can be used as adjunctive pain medications to reduce opioid requirements (Table 4). However, their safety profile and effectiveness as sole agents for pain management have not been adequately studied in critically ill patients. Pharmacologic treatment principles extrapolated from non-ICU studies may not be applicable to critically ill patients.52 IV acetaminophen has been recently approved for use in the United States and has been shown to be safe and effective when used in conjunction with opioids for postoperative pain in surgical ICU patients following major or cardiac surgery.80,86–89 Neuropathic pain, poorly treated with opioids alone, can be treated with enterally administered gabapentin and carbamazepine in ICU patients with sufficient gastro-intestinal absorption and motility.90,91
Methods of dosing analgesics are another treatment consideration. The choice of intermittent vs. continuous IV strategies may depend on drug pharmacokinetics, frequency and severity of pain, and/or the patient’s mental status.92 Enteral administration of opioids and other pain medications should be limited to patients with adequate gastrointestinal absorptive capacity and motility. Regional or neuraxial (spinal or epidural) modalities may also be used for postoperative analgesia following selected surgical procedures.93,94
Complementary, nonpharmacologic interventions for pain management, such as music therapy and relaxation techniques, may be opioid-sparing and analgesia-enhancing; they are low cost, easy to provide, and safe. Although a multimodal approach to pain management in ICU patients has been recommended, few studies have been published on the effectiveness of nonpharmacologic interventions in these patients.52,95
Pain occurs commonly in adult ICU patients, regardless of their admitting diagnoses. Pain can preclude patients from participating in their ICU care (e.g., early mobilization, weaning from mechanical ventilation). Thus, clinicians should frequently reassess patients for pain and carefully titrate analgesic interventions to prevent potential negative sequelae due to either inadequate or excessive analgesic therapy. Clinicians should perform routine and reproducible pain assessments in all critically ill patients, using either patient self-report or systematically applied behavioral measures. Pain management can be facilitated by identifying and treating pain early rather than waiting until it becomes severe.52
Pain and Analgesia: Questions, Statements, and Recommendations.
1. Incidence of Pain
a.Question: Do adult ICU patients experience nonprocedural pain in the ICU and, if so, what events or situations are related to pain? (descriptive) Answer: Adult medical, surgical, and trauma ICU patients routinely experience pain, both at rest and with routine ICU care (B). Pain in adult cardiac surgery patients is common and poorly treated; women experience more pain than men after cardiac surgery (B). Rationale: Medical, surgical, and trauma ICU patients experience significant pain, even at rest.61,63,73 Therefore, all adult patients in any ICU should be evaluated for pain. Pain at rest should be considered a major clinical diagnostic syndrome. In cardiac surgery patients, pain related to the surgery, coughing, respiratory care procedures, and mobilization remains prevalent and poorly treated; women experience more pain than men after cardiac surgery.73,96–98 Therefore, activity pain in cardiac surgery patients must be assessed and treated. Pain management should be individualized according to the patient’s experience of pain, with special attention to its occurrence in women.97
Question: What is the pain experienced by adult ICU patients undergoing procedures? (descriptive) Answer: Procedural pain is common in adult ICU patients (B).
Rationale: Pain associated with nonsurgical procedures such as chest tube removal or wound care is prevalent in adult ICU patients.68,99 Generally at a moderate level,68 pain is influenced by preprocedural pain levels and the administration of analgesics.100 Less than 25% of patients receive analgesics before the procedures.68 Procedural pain varies with age64,66 and is greater in non-Caucasians than in Caucasians.64,66,68 Differences in procedural pain between nonsurgical and surgical patients vary according to procedure.64,66 Hemodynamic changes are not valid correlates of procedural pain.99 Available information suggests that preemptive analgesia has benefits, but the risks of procedural pain and the lack of preemptive treatment are unclear.
2. Pain Assessment
a.Question: Should pain assessments be routinely performed in adult ICU patients? (actionable)
Answer: We recommend that pain be routinely monitored in all adult ICU patients (+1B).
Rationale: Routine pain assessments in adult ICU patients are associated with improved clinical outcomes. Pain assessment, especially if protocolized, has been significantly associated with a reduction in the use of analgesic medications, ICU length of stay (LOS), and duration of mechanical ventilation.3,62 Pain assessment is essential for appropriate treatment, especially when part of a comprehensive pain management protocol. Although the quality of evidence is moderate, a strong recommendation for performing routine pain assessments in all ICU patients is appropriate, as the benefits strongly outweigh the risks.
b.Question: What are the most valid and reliable behavioral measures of pain in critically ill adult patients who are unable to self-report? (descriptive)
Answer: The Behavioral Pain Scale (BPS) and the Critical-Care Pain Observation Tool (CPOT) are the most valid and reliable behavioral pain scales for monitoring pain in medical, postoperative, or trauma (except for brain injury) adult ICU patients who are unable to self-report, and in whom motor function is intact and behaviors are observable. Using these scales in other ICU patient populations and translating them into foreign languages other than French or English require further validation testing (B).
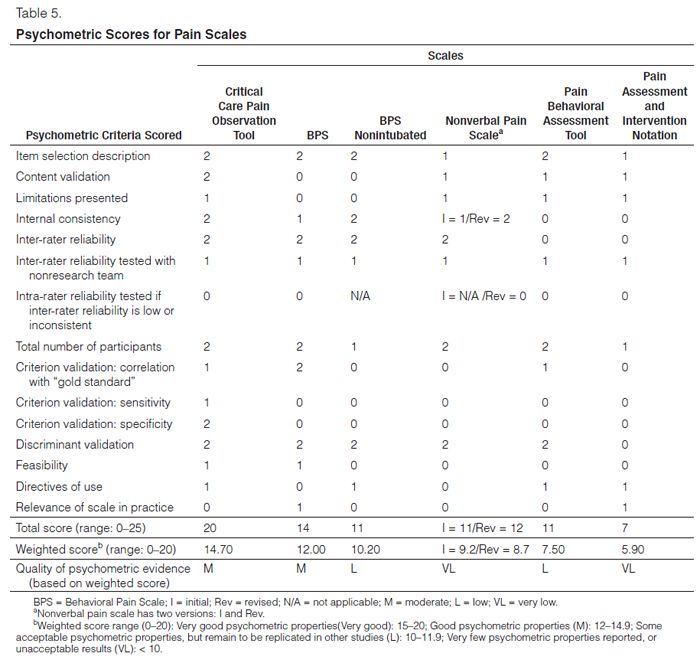
Rationale: A total of six behavioral pain scales were analyzed: BPS; BPS—Non-Intubated (BPS-NI); CPOT; Non-Verbal Pain Scale (NVPS), both initial and revised (NVPS-I, NVPS-R); Pain Behavioral Assessment Tool (PBAT); and the Pain Assessment, Intervention, and Notation (PAIN) Algorithm. Table 5 summarizes their psychometric scores. Observational studies, although somewhat limited, provide consistent evidence that the BPS (3–12 total score) and CPOT (0–8 total score) scales have good psychometric properties in terms of: inter-rater reliability,101–109 discriminant validity,101,102,104,107,109,110 and criterion validity,103–105,109,110 in medical, postoperative, and trauma ICU patients. A CPOT score of greater than 2 had a sensitivity of 86% and a specificity of 78% for predicting significant pain in postoperative ICU adults exposed to a nociceptive procedure.111,112 Investigators suggested a similar cutoff score for the BPS (> 5), on the basis of descriptive statistics in nonverbal ICU adults during nociceptive procedures compared with patients at rest.62 The CPOT and BPS can be successfully implemented in the ICU following short, standardized training sessions.2,85 Their regular use can lead to better pain management and improved clinical outcomes in ICU patients.2,3,85 The BPS-NI is derived from the BPS and adapted for nonintubated ICU patients,113 but it has been tested in a group of only 30 patients so far, and replication studies are needed to support its psychometric properties. More studies are also necessary to examine the psychometric properties of the NVPS,114 NVPS-R,115 PBAT,116 and PAIN.117
c.Question: Should vital signs be used to assess pain in adult ICU patients? (actionable)
Answer: We do not suggest that vital signs (or observational pain scales that include vital signs) be used alone for pain assessment in adult ICU patients (–2C). We suggest that vital signs may be used as a cue to begin further assessment of pain in these patients, however (+2C).
Rationale: Observational studies with major limitations provide inconsistent evidence of the validity of vital signs for the purpose of pain assessment in medical, postoperative, and trauma ICU patients. Even if there is a trend for vital signs to increase when critically ill patients are exposed to painful procedures, these increases are not reliable predictors of pain.66,101,105,107,110 Vital signs have been reported to increase both during nociceptive and nonnociceptive procedures109 or to remain stable during nociceptive exposure.99 Vital signs do not correlate with either patients’ self-report of pain105,110 or behavioral pain scores.101,107 But because vital signs may change with pain, distress, or other factors, they can be a cue to perform further pain assessments in these patients.118
3. Treatment of Pain
a.Question: Should procedure-related pain be treated pre-emptively in adult ICU patients? (actionable)
Answer: We recommend that preemptive analgesia and/or nonpharmacologic interventions (e.g., relaxation) be administered to alleviate pain in adult ICU patients prior to chest tube removal (+1C). We suggest that for other types of invasive and potentially painful procedures in adult ICU patients, preemptive analgesic therapy and/or nonpharmacologic interventions may also be administered to alleviate pain (+2C).
Rationale: Our strong recommendation is that patients undergoing chest tube removal should be preemptively treated for pain, both pharmacologically and non-pharmacologically. Significantly lower pain scores were reported by patients if they received IV morphine plus relaxation,119 topical valdecoxib,120 IV sufentanil, or fentanyl121 prior to chest tube removal. According to these studies, the desirable consequences outweigh undesirable effects. One can reasonably assume that most ICU patients would want their pain preemptively treated with nonpharmacologic and/or pharmacologic interventions prior to other painful procedures as well.
b.Question: What types of medications should be administered for pain relief in adult ICU patients? (actionable)
Answer: We recommend that IV opioids be considered as the first-line drug class of choice to treat non-neuropathic pain in critically ill patients (+1C). All available IV opioids, when titrated to similar pain intensity endpoints, are equally effective (C). We recommend that either enterally administered gabapentin or carbamazepine, in addition to IV opioids, be considered for the treatment of neuropathic pain (+1A). We suggest that nonopioid analgesics be considered to decrease the amount of opioids administered (or to eliminate the need for IV opioids altogether) and to decrease opioid-related side effects (+2C).
Rationale: For non-neuropathic pain, evidence supports using an opiate-based regimen to decrease pain intensity.87,90,91,122–136 Apart from drug cost and resource utilization, all opioids administered IV appear to exhibit similar analgesic efficacy and are associated with similar clinical outcomes (e.g., duration of mechanical ventilation, LOS) when titrated to similar pain intensity endpoints. For non-neuropathic pain, nonopioids such as IV acetaminophen,87 oral, IV, or rectal cyclooxygenase inhibitors,122,123,135 or IV ketamine132,137 can be used in addition to opioids. Using nonopioids may also decrease the overall quantity of opioids administered and the incidence and severity of opioid-related side effects. In patients with neuropathic pain, IV opioid use plus oral gabapentin or carbamazepine provides superior pain relief in mechanically ventilated patients compared to IV opioid use alone.90,91 A lack of direct comparisons between opioids and nonopioids hinders conclusions regarding the effect of non-opioid analgesics, particularly in ICU patients.
Question: What mode of analgesic delivery (i.e., either neuraxial or parenteral) is recommended for pain relief in critically ill adults who have undergone either thoracic or abdominal surgery or who have traumatic rib fractures (including both mechanically ventilated and nonmechanically ventilated ICU patients)? (actionable)
Answer: We recommend that thoracic epidural anesthesia/analgesia be considered for postoperative analgesia in patients undergoing abdominal aortic surgery (+1B). We provide no recommendation for using a lumbar epidural over parenteral opioids for postoperative analgesia in patients undergoing abdominal aortic aneurysm surgery, due to a lack of benefit when these routes of administration are compared in this patient population (0,A). We provide no recommendation for the use of thoracic epidural analgesia in patients undergoing either intrathoracic or nonvascular abdominal surgical procedures, because of insufficient and conflicting evidence for this mode of analgesic delivery in these patients (0,B). We suggest that thoracic epidural analgesia be considered for patients with traumatic rib fractures (+2B). We provide no recommendation for neuraxial/regional analgesia over systemic analgesia in medical ICU patients, due to lack of evidence in this patient population (0, No Evidence).
Rationale: High-quality evidence suggests that thoracic epidural anesthesia/analgesia in patients undergoing abdominal aortic surgery when the epidural catheter is placed preoperatively provides superior pain relief to parenteral opioids alone; rare complications of thoracic epidurals in these patients include postoperative heart failure, infections, and respiratory failure.138,139 High-quality evidence demonstrates no benefit with lumbar epidural compared with parenteral opioids in these patients.139–141 Several shortcomings in research design make it difficult to recommend the use of thoracic epidural analgesia in patients undergoing either intrathoracic or nonvascular abdominal surgical procedures.142–149 Epidural analgesia administered to patients with rib fractures improved pain control, especially during coughing or deep breathing, lowered the incidence of pneumonia, but increased the risk of hypotension.150,151 No evidence supports using neuraxial/regional analgesia in medical ICU patients.
Agitation and Sedation. Indications for sedation. Agitation and anxiety occur frequently in critically ill patients and are associated with adverse clinical outcomes.152–156 Sedatives are commonly administered to ICU patients to treat agitation and its negative consequences.157 Prompt identification and treatment of possible underlying causes of agitation, such as pain, delirium, hypoxemia, hypoglycemia, hypotension, or withdrawal from alcohol and other drugs, are important. Efforts to reduce anxiety and agitation, including maintenance of patient comfort, provision of adequate analgesia, frequent reorientation, and optimization of the environment to maintain normal sleep patterns, should be attempted before administering sedatives.
Sedatives can be titrated to maintain either light (i.e., patient is arousable and able to purposefully follow simple commands) or deep sedation (i.e., patient is unresponsive to painful stimuli). Multiple studies have demonstrated the negative consequences of prolonged, deep sedation, and the benefits of maintaining lighter sedation levels in adult ICU patients.10,14,15,20,158 The use of sedation scales, sedation protocols designed to minimize sedative use, and the use of nonbenzodiazepine medications are associated with improved ICU patient outcomes, including a shortened duration of mechanical ventilation, ICU and hospital LOS, and decreased incidences of delirium and long-term cognitive dysfunction.7–10,12,13,18,19,159–162
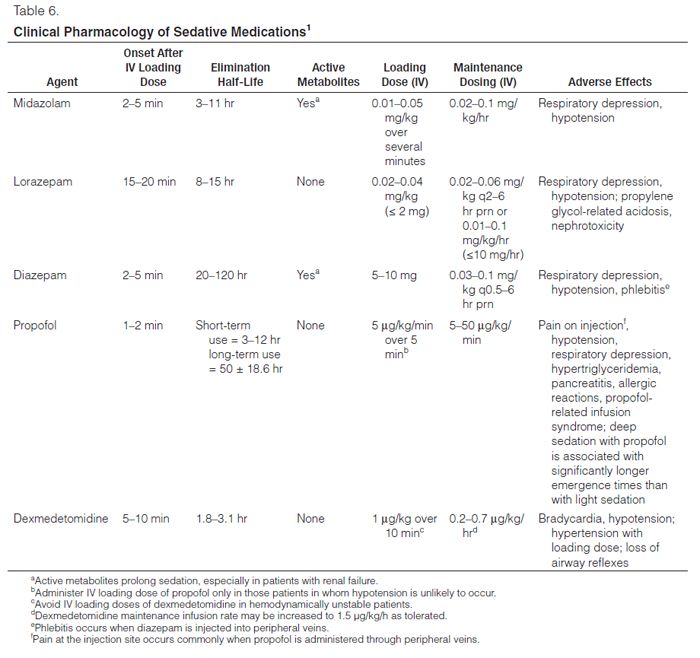
Clinical pharmacology of sedatives. Historically, benzodiazepines (i.e., midazolam and lorazepam) and propofol have commonly been used to sedate ICU patients. The 2002 guidelines recommended midazolam only for short-term sedation, lorazepam for long-term sedation, and propofol for patients requiring intermittent awakenings.1 Recent surveys assessing sedation practices demonstrate that midazolam and propofol remain the dominant medications used for ICU sedation, with decreasing lorazepam use, and rare use of barbiturates, diazepam, and ketamine in the ICU.62,163–166 Dexmedetomidine, approved in the United States shortly before completion of the 2002 guidelines, is now more commonly administered for ICU sedation.166–168 The clinical pharmacology of sedatives prescribed for ICU patients is summarized in Table 6.
Benzodiazepines. Benzodiazepines activate γ-aminobutyric acid A (GABAA) neuronal receptors in the brain. They have anxiolytic, amnestic, sedating, hypnotic, and anticonvulsant effects, but no analgesic activity.169,170 Their amnestic effects extend beyond their sedative effects.171 Lorazepam is more potent than midazolam, which is more potent than diazepam. Midazolam and diazepam are more lipid soluble than lorazepam, resulting in a quicker onset of sedation and a larger volume of distribution than for lorazepam. Elderly patients are significantly more sensitive to the sedative effects of benzodiazepines.171 Benzodiazepines can cause respiratory depression and systemic hypotension, especially when administered in conjunction with other cardiopulmonary depressants, particularly opioids.172 Benzodiazepine-induced cardiopulmonary instability is more likely to occur in critically ill patients with baseline respiratory insufficiency and/or cardiovascular instability.172 Tolerance to benzodiazepines develops with long-term administration.
All benzodiazepines are metabolized by the liver. Benzodiazepine clearance is reduced in patients with hepatic dysfunction and other disease states, in elderly patients, and when administered with other medications that inhibit cytochrome P450 enzyme systems and/or glucuronide conjugation in the liver.173–175 The elimination half-life and duration of clinical effect of lorazepam are also increased in patients with renal failure.176,177 The active metabolites of midazolam and diazepam may accumulate with prolonged administration, especially in patients with renal dysfunction.178 Benzodiazepine clearance decreases with age.175,179,180
Delayed emergence from sedation with benzodiazepines can result from prolonged administration of benzodiazepines (due to saturation of peripheral tissues), advanced age, hepatic dysfunction, or renal insufficiency.171,175,181 Because of the greater potency and slower clearance of lorazepam, emergence from short-term sedation (1–2 days) with lorazepam may be longer than with midazolam. However, comparative studies on the prolonged use of these drugs in ICU patients suggest greater variability and longer time to awakening with midazolam than with lorazepam.171,175,182–184 Diazepam has a prolonged duration of action due to saturation of peripheral tissues and active metabolites that can accumulate in patients with renal insufficiency.185
Parenteral formulations of lorazepam contain propylene glycol as a diluent, which can cause toxicity in ICU patients.186–190 Propylene glycol toxicity manifests as metabolic acidosis and acute kidney injury. Because these conditions occur frequently in critically ill patients, their possible association with lorazepam administration may be overlooked. Although initially thought to accumulate only in patients receiving very high lorazepam doses via continuous infusion (i.e., 15–25 mg/hr), current evidence suggests that total daily IV doses as low as 1 mg/kg can cause propylene glycol toxicity.191 The serum osmol gap has been used as a reliable screening and surveillance tool; an osmol gap greater than 10–12 mOsm/L may help identify patients receiving lorazepam who have significant propylene glycol accumulation.187,191
Propofol. Propofol is an IV sedative that binds to multiple receptors in the central nervous system to interrupt neural transmission, including GABAA, glycine, nicotinic, and M1 muscarinic receptors.192–194 Propofol has sedative, hypnotic, anxiolytic, amnestic, antiemetic, and anticonvulsant properties, but no analgesic effects.195,196 In ICU patients, propofol’s amnestic effects at light sedation levels are less than that of benzodiazepines.197 Propofol is highly lipid soluble and quickly crosses the blood-brain barrier, resulting in the rapid onset of sedation. Because of its high lipid solubility, propofol also rapidly redistributes into peripheral tissues. This rapid redistribution, combined with high hepatic and extrahepatic clearance, results in a rapid offset of effect following short-term propofol administration. Because of its short duration of sedative effect, propofol may be useful in patients requiring frequent awakenings for neurologic assessments and it may facilitate daily sedation interruption protocols.183,198,199 However, long-term propofol administration can lead to the saturation of peripheral tissues and prolonged emergence.198
Propofol causes dose-dependent respiratory depression and hypotension due to systemic vasodilation. These effects may be more pronounced when propofol is administered with other sedative and opioid medications. Cardiopulmonary instability with propofol administration is more likely to occur in patients with baseline respiratory insufficiency and/or cardiovascular instability. Other side effects include hypertriglyceridemia, acute pancreatitis, and myoclonus.200–204 Propofol is dissolved in a 10% lipid emulsion containing egg lecithin and soybean oil, which can precipitate allergic reactions in patients with either egg or soybean allergies. Some generic formulations of propofol contain sulfite preservatives, which may also cause allergic reactions.196
Propofol administration is rarely associated with developing propofol infusion syndrome (PRIS). The signs and symptoms of PRIS vary but may include worsening metabolic acidosis, hypertriglyceridemia, hypotension with increasing vasopressor requirements, and arrhythmias. Acute kidney injury, hyperkalemia, rhabdomyolysis, and liver dysfunction have also occasionally been reported with PRIS.205,206 Possible PRIS mechanisms include mitochondrial dysfunction, impaired fatty acid oxidation, diversion of carbohydrate metabolism to fat substrates, and propofol metabolite accumulation.207 PRIS is usually associated with prolonged administration of high propofol doses (> 70 μg/kg/min), but it may also occur with low-dose infusions.208,209 The incidence of PRIS with propofol infusions is approximately 1%.210 Mortality from PRIS is high (up to 33%) and may occur even after discontinuing the infusion.202 The variable presentation, lack of diagnostic specificity, and infrequent occurrence of PRIS make detection of this potentially life-threatening condition difficult. Early recognition and discontinuation of propofol in patients with suspected PRIS are critically important. Management of patients with PRIS is otherwise supportive.
Dexmedetomidine. Dexmedetomidine is a selective a2-receptor agonist with sedative, analgesic/opioid sparing, and sympatholytic properties, but with no anticonvulsant properties.211,212 Dexmedetomidine produces a pattern of sedation that differs considerably from other sedative agents. Patients sedated with dexmedetomidine are more easily arousable and interactive, with minimal respiratory depression.213,214 The onset of sedation occurs within 15 mins and peak sedation occurs within 1 hr of starting an IV infusion of dexmedetomidine.167,215 Sedation onset may be hastened by administering an initial IV loading dose of dexmedetomidine, but this is more likely to cause hemodynamic instability in critically ill patients.216 Dexmedetomidine is rapidly redistributed into peripheral tissues and is metabolized by the liver.217 In patients with normal liver function, the elimination half-life is approximately 3 hrs.215 Patients with severe hepatic dysfunction have impaired dexmedetomidine clearance, can experience prolonged emergence, and may require lower dexmedetomidine doses.218 Although dexmedetomidine has only been approved in the United States for short-term sedation of ICU patients (< 24 hrs) at a maximal dose of 0.7 μg/kg/hr (up to 1.0 μg/kg/h for procedural sedation), several studies demonstrate the safety and efficacy of dexmedetomidine infusions administered for greater than 24 hrs (up to 28 days) and at higher doses (up to 1.5 μg/kg/hr).216,219–222
The most common side effects of dexmedetomidine are hypotension and bradycardia.223 IV loading doses can cause either hypotension or hypertension.215,224 Because dexmedetomidine does not significantly affect respiratory drive, it is the only sedative approved in the United States for administration in nonintubated ICU patients, and infusions can be continued as needed following extubation.225–227 However, dexmedetomidine can cause a loss of oropharyngeal muscle tone which can lead to airway obstruction in nonintubated patients, so continuous respiratory monitoring for both hypoventilation and hypoxemia in these patients is indicated.225 Dexmedetomidine’s opioid-sparing effect may reduce opioid requirements in critically ill patients.219,220,224,228 The mechanism of action for the analgesic properties of dexmedetomidine remains controversial.229 Although a2 receptors are located in the dorsal region of the spinal cord and in supraspinal sites, dexmedetomidine’s nonspinal analgesic effects have been documented.230 One recent study suggests that ICU patients receiving dexmedetomidine may have a lower prevalence of delirium than patients sedated with midazolam.220
Agitation and Sedation: Questions, Statements, and Recommendations.
1. Depth of Sedation and Clinical Outcomes
Question: Should adult ICU patients be maintained at a light level of sedation? (actionable)
Answer: Maintaining light levels of sedation in adult ICU patients is associated with improved clinical outcomes (e.g., shorter duration of mechanical ventilation and a shorter ICU LOS) (B). Maintaining light levels of sedation increases the physiologic stress response, but is not associated with an increased incidence of myocardial ischemia (B). The association between depth of sedation and psychological stress in these patients remains unclear (C). We recommend that sedative medications be titrated to maintain a light rather than deep level of sedation in adult ICU patients, unless clinically contraindicated (+1B).
Rationale: Thirteen studies examined the direct relationship between sedative depth and clinical outcomes in ICU patients, including duration of mechanical ventilation, ICU LOS, measures of physiologic stress, and assessments of post-ICU psychological stress.10,14,15,20,158,231–238 Five studies demonstrated that deeper sedation levels are associated with longer durations of mechanical ventilation and ICU LOS.10,14,15,20,158 Three studies demonstrated evidence of increased physiologic stress in terms of elevated catecholamine concentrations and/or increased oxygen consumption at lighter sedation levels,232,235,236 whereas one study did not.233 The clinical significance of this is unclear, because no clear relationship was observed between elevated markers of physiologic stress and clinical outcomes, such as myocardial ischemia, in these patients.232–234
Four studies examined the relationship between depth of sedation and post-ICU psychological stress.20,231,237,238 One showed that a protocol of daily sedation interruption did not cause adverse psychological outcomes,231 whereas another found a low incidence of such events in patients who were lightly sedated.20 A third study showed that deeper sedation levels were associated with a lower incidence of recall, but that delusional memories did not correlate with lighter levels of sedation.238 However, in the fourth study, periods of wakefulness were associated with recall of stressful ICU memories.237 The overall quality of evidence evaluating the relationship between depth of ICU sedation and post-ICU psychological stress is low, and these study results are conflicting. Thus, the overall benefits of maintaining a light sedation level in ICU patients appear to outweigh the risks.
2. Monitoring Depth of Sedation and Brain Function
a.Sedation scales
Question: Which subjective sedation scales are the most valid and reliable in the assessment of depth and quality of sedation in mechanically ventilated adult ICU patients? (descriptive)
Answer: The Richmond Agitation-Sedation Scale (RASS) and Sedation-Agitation Scale (SAS) are the most valid and reliable sedation assessment tools for measuring quality and depth of sedation in adult ICU patients (B).
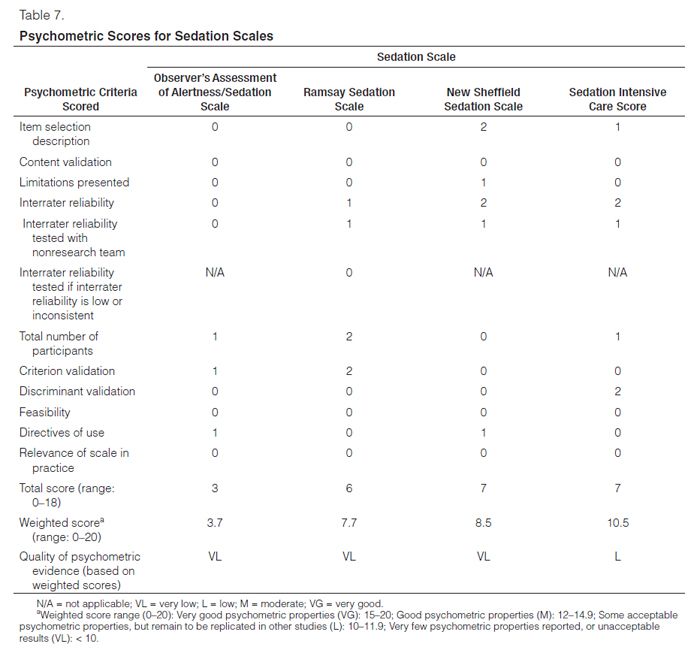
Rationale: Several subjective sedation scales exist for monitoring depth of sedation and agitation in adult ICU patients, and their psychometric properties are well described. But the cumulative degree of psychometric properties tested and the quality of evidence vary widely among scales. We reviewed the psychometric properties of ten subjective sedation scales, each developed for evaluating the depth and quality of sedation in adult ICU patients: 1) Observer’s Assessment of Alertness/Sedation Scale (OAA/S); 2) Ramsay Sedation Scale (Ramsay); 3) New Sheffield Sedation Scale (Sheffield); 4) Sedation Intensive Care Score (SEDIC); 5) Motor Activity Assessment Scale (MAAS); 6) Adaptation to the Intensive Care Environment (ATICE); 7) Minnesota Sedation Assessment Tool (MSAT); 8) Vancouver Interaction and Calmness Scale (VICS); 9) SAS; and 10) RASS. We reviewed 27 studies including 2,805 patients2,239–264: 26 were observational studies and one used a blinded and randomized format to evaluate videos of previously scored patient sedation levels.253 Table 7 summarizes the psychometric scores for all ten sedation scales.
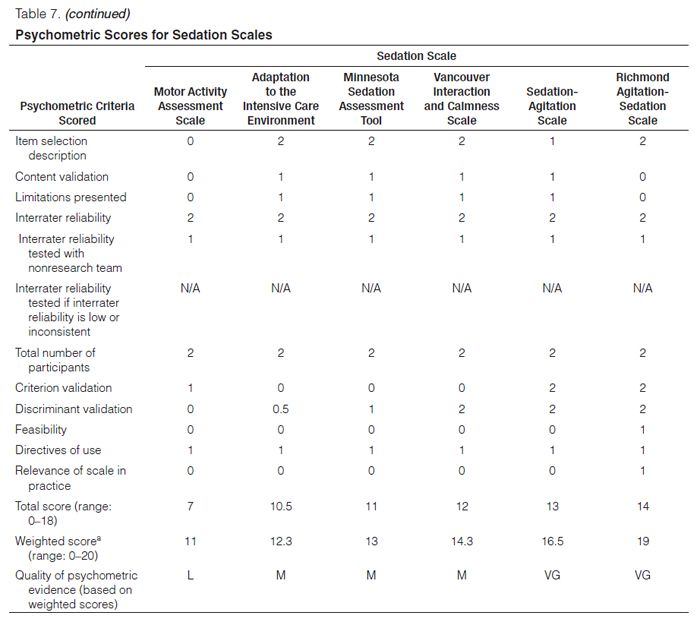
The RASS and SAS yielded the highest psychometric scores (i.e., inter-rater reliability, convergent or discriminant validation) and had a robust number of study participants. Both scales demonstrated a high degree of inter-rater reliability, which included ICU clinicians.240,262,263 Both scales were able to discriminate different sedation levels in various clinical situations.246,250,258,261 Moderate to high correlations were found between the sedation scores of these scales and either electroencephalogram (EEG) or bispectral index (BIS) values.244,246,258 In addition, the RASS consistently provided a consensus target for goal-directed delivery of sedative agents, demonstrating feasibility of its usage.2,246,254
We found that the ATICE, MSAT, and VICS had good quality of psychometric evidence, but some psychometric properties (e.g., convergent or discriminant validation) have not been tested.242,243,249,259,260 The MAAS, SEDIC, Sheffield, Ramsay, and OAA/S scales had a lower quality of evidence; replication studies and psychometric testing of reliability and validity for determining the depth and quality of sedation in ICU patients are needed.239,241,242,245,247–249,251–253,255,261,262,264
In summary, our comparative assessment of the psychometric properties of sedation scales revealed RASS and SAS to be the most valid and reliable for use in critically ill patients, whereas ATICE, MSAT, and VICS are moderately valid and reliable. Additional testing of the remaining scales is needed to better assess their reliability and validity in determining depth of sedation in critically ill patients.
b. Neurologic monitoring
i.Question: Should objective measures of brain function (e.g., auditory evoked potentials [AEPs], bispectral index [BIS], Narcotrend Index [NI], Patient State Index [PSI], or state entropy [SE]) be used to assess depth of sedation in noncomatose, adult ICU patients who are not receiving neuromuscular blocking agents? (actionable)
Answer: We do not recommend that objective measures of brain function (e.g., AEPs, BIS, NI, PSI, or SE) be used as the primary method to monitor depth of sedation in noncomatose, nonparalyzed critically ill adult patients, as these monitors are inadequate substitutes for subjective sedation scoring systems (–1B).
ii.Question: Should objective measures of brain function (e.g., AEPs, BIS, NI, PSI, or SE) be used to measure depth of sedation in adult ICU patients who are receiving neuromuscular blocking agents? (actionable)
Answer: We suggest that objective measures of brain function (e.g., AEPs, BIS, NI, PSI, or SE) be used as an adjunct to subjective sedation assessments in adult ICU patients who are receiving neuromuscular blocking agents, as subjective sedation assessments may be unobtainable in these patients (+2B).
iii.Question: Should EEG monitoring be used to detect nonconvulsive seizure activity and to titrate electrosuppressive medication to obtain burst suppression in adult ICU patients with either known or suspected seizures? (actionable)
Answer: We recommend that EEG monitoring be used to monitor nonconvulsive seizure activity in adult ICU patients with either known or suspected seizures, or to titrate electrosuppressive medication to achieve burst suppression in adult ICU patients with elevated intracranial pressure (+1A).
Rationale: We reviewed 18 studies comparing objective monitors of sedation to sedation scoring systems in adult ICU patients.244,248,258,265–279 Objective monitors included both raw and processed EEG and AEP monitors. Processed EEG monitors (i.e., conversion of a raw EEG signal to an index by an algorithm) included the Bispectral Index (BIS) and Bispectral Index XP (BIS-XP SE), NI, and the PSI. The overall evidence is conflicting. Fifteen studies of moderate quality found that objective sedation monitors based on either AEP or processed EEG signals, including BIS, NI, SE, and PSI, may be useful adjuncts to subjective sedation assessments in critically ill patients.244,248,258,266,267,271–273,276,278–283 However, most of these studies reported that electromyographic signals negatively affected the correlation between the objective measure in question and sedation scores. Five additional studies of moderate quality found no benefit in using objective monitors over subjective scoring systems to assess depth of sedation.268–270,277,284 In most studies, objective monitors distinguished only between deep and light levels of sedation, but their values correlated poorly with specific sedation scores and were negatively influenced by electromyographic signal artifact. Several studies demonstrated that continuous EEG monitoring is useful for detecting nonconvulsive seizure activity in ICU patients either with known seizure activity or who are at risk for seizures (e.g., traumatic brain injury, intracerebral hemorrhage, cerebral vascular accidents, patients with an unexplained depressed level of consciousness).275,281 Continuous EEG monitoring may also be useful in titrating electrosuppressive medications to achieve burst suppression in critically ill patients with increased intracranial pressure.275,281
3. Choice of Sedative
Question: Should nonbenzodiazepine-based sedation, instead of sedation with benzodiazepines, be used in mechanically ventilated adult ICU patients? (actionable)
Answer: We suggest that sedation strategies using nonbenzodiazepine sedatives (either propofol or dexmedetomidine) may be preferred over sedation with benzodiazepines (either midazolam or lorazepam) to improve clinical outcomes in mechanically ventilated adult ICU patients (+2B).
Rationale: In general, the choice of sedative agent used in ICU patients should be driven by: 1) specific indications and sedation goals for each patient; 2) the clinical pharmacology of the drug in a particular patient, including its onset and offset of effect and its side effect profile; and 3) the overall costs associated with using a particular sedative. Outcomes studies of the effects of sedative agents in ICU patients typically compare a benzodiazepine (either midazolam or lorazepam) to a nonbenzodiazepine (either propofol or dexmedetomidine) for sedation. At the time of our literature review, only two low-quality studies had been published comparing clinical outcomes in ICU patients receiving propofol vs. dexmedetomidine for sedation.285,286 No studies have compared clinical outcomes in ICU patients sedated with either ketamine or other sedative agents. Several studies we reviewed suggested that the sustained use of benzodiazepine-based sedative regimens is associated with adverse clinical outcomes, such as prolonged dependence on mechanical ventilation, increased ICU LOS, and the development of delirium.29,183,220,286–293 These findings had not been consistently reported, however.197,222,285,294–297
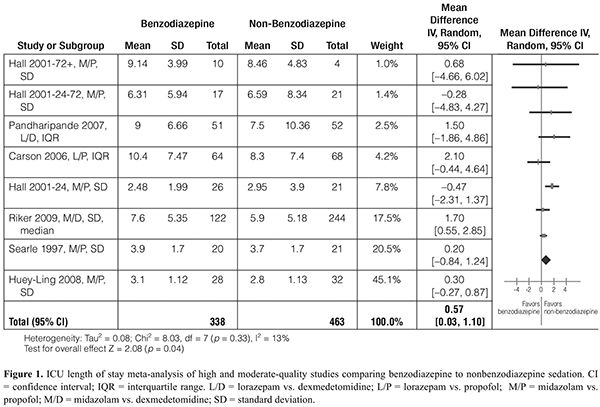
We reviewed 13 studies of 1,551 ICU patients comparing clinical outcomes in patients sedated with either benzodiazepines (midazolam or lorazepam) or nonbenzodiazepines (propofol or dexmedetomidine) and found no consistent differences in ICU LOS.183,197,220,222,285,286,292–298 However, our meta-analysis of six trials ranked as moderate to high quality suggested that sedation with benzodiazepines may increase ICU LOS by approximately 0.5 days compared with nonbenzodiazepine sedation (p = 0.04) (Fig. 1).183,197,220,222,292,295–297 Limited data suggested that mechanical ventilation is prolonged with benzodiazepine-based sedation.183,220,292,298 There was no apparent difference in mortality with benzodiazepine vs. nonbenzodiazepine sedation.220,222,285,295 Six trials evaluated the influence of benzodiazepine-based sedation on the cost of ICU care;194,222,286,294,299,300 only one study found that benzodiazepine-based sedation (i.e., midazolam infusion) was associated with higher ICU costs than sedation with dexmedetomidine.300
When we compared outcome studies in ICU patients sedated with propofol vs. either midazolam or lorazepam, we found several studies demonstrating that propofol use may be associated with a shorter duration of mechanical ventilation, but this effect varied across patient populations,183,197,291,292,294–297 and did not necessarily translate into a shorter ICU LOS. There was no apparent difference in the incidence of self-extubation with propofol vs. benzodiazepine sedation.183 A separate systematic review evaluated 16 randomized, controlled trials comparing clinical outcomes in ICU patients receiving either propofol or another sedative agent.291 When this meta-analysis was restricted to a comparison of propofol and midazolam, there was no difference in mortality, a slight reduction in the duration of mechanical ventilation with propofol, but no difference in ICU LOS. The relationship between using either propofol or benzodiazepines for sedation and the development of delirium is unclear. Only two relevant studies have been published comparing the incidence of delirium in ICU patients receiving propofol vs. benzodiazepines for sedation.285, 286 In both studies, patients were randomized to receive propofol, midazolam, or dexmedetomidine for sedation, and the incidence of delirium was similar in patients receiving either propofol or midazolam, but the quality of evidence was low.
We reviewed five studies comparing outcomes in ICU patients receiving either dexmedetomidine or a benzodiazepine (either midazolam or lorazepam) for sedation.220,222,285,286,293 Three of the four studies evaluating duration of mechanical ventilation showed no difference between these groups.222,285,286 However, the largest study did demonstrate a significant reduction in the time to liberation from mechanical ventilation with dexmedetomidine (3.7 days) compared with midazolam (5.6 days).220 Dexmedetomidine was not associated with a lower incidence of self-extubation compared with benzodiazepines.222 Four of the five studies showed no difference in ICU LOS.220,222,285,286 Five studies, including a subgroup analysis from the Maximizing Efficacy of Targeted Sedation and Reducing Neurological Dysfunction trial, evaluated the development of delirium in patients receiving either dexmedetomidine or a benzodiazepine for sedation.220,222,285,286,298 Delirium was reported in terms of frequency of occurrence, prevalence, and delirium-free days. Three studies favored dexmedetomidine,286,288,300 although only one was of high quality.220 The subgroup analysis trial favored dexmedetomidine over lorazepam in septic patients only.298 One trial showed no relationship between benzodiazepine use and delirium.222 One very low-quality trial suggested a higher rate of delirium with dexmedetomidine, but suffered from serious methodological flaws including imprecision in the measurement of delirium.285
The results of two high-quality, randomized, double-blind, comparative trials of dexmedetomidine vs. either midazolam or propofol for ICU sedation were published after the guideline task force had completed its voting and developed its recommendations.301 The relevant outcomes in both studies included duration of mechanical ventilation, and ICU and hospital LOS. Except for a longer duration of mechanical ventilation with midazolam use, no differences between groups were seen. These results are consistent with both our analysis of previously published data and subsequent recommendation for benzodiazepine-based vs. nonbenzodiazepine-based sedation.
In summary, the current literature supports modest differences in outcomes with benzodiazepine-based vs. nonbenzodiazepine-based sedation. Our meta-analysis of moderate to high-quality trials indicates that benzodiazepine sedation is associated with an increased ICU LOS. Moderate to high-quality data favor using propofol over lorazepam183 and dexmedetomidine over midazolam220 to limit the duration of mechanical ventilation. The clinical significance of the comparative deliriogenic effects of benzodiazepines remains uncertain, with one high-quality trial indicating benzodiazepines pose higher risks than dexmedetomidine.220 Additional recommendations to prevent or treat delirium can be found in the Delirium section of these guidelines. Dexmedetomidine may offer an advantage in ICU resource consumption compared to midazolam infusions in health care institutions that are efficient in transferring patients out of the ICU.300 Despite the apparent advantages in using either propofol or dexmedetomidine over benzodiazepines for ICU sedation, benzodiazepines remain important for managing agitation in ICU patients, especially for treating anxiety, seizures, and alcohol or benzodiazepine withdrawal. Benzodiazepines are also important when deep sedation, amnesia, or combination therapy to reduce the use of other sedative agents is required.166,302
Delirium
Epidemiology of Delirium in ICU Patients. Delirium is a syndrome characterized by the acute onset of cerebral dysfunction with a change or fluctuation in baseline mental status, inattention, and either disorganized thinking or an altered level of consciousness.303–309 The cardinal features of delirium are: 1) a disturbed level of consciousness (i.e., a reduced clarity of awareness of the environment), with a reduced ability to focus, sustain, or shift attention; and 2) either a change in cognition (i.e., memory deficit, disorientation, language disturbance), or the development of a perceptual disturbance (i.e., hallucinations, delusions).310 A common misconception is that delirious patients are either hallucinating or delusional, but neither of these symptoms is required to make the diagnosis. Other symptoms commonly associated with delirium include sleep disturbances, abnormal psychomotor activity, and emotional disturbances (i.e., fear, anxiety, anger, depression, apathy, euphoria). Patients with delirium may be agitated (hyperactive delirium), calm or lethargic (hypoactive delirium), or may fluctuate between the two subtypes. Hyperactive delirium is more often associated with hallucinations and delusions, while hypoactive delirium is more often characterized by confusion and sedation, and is often misdiagnosed in ICU patients.
Delirium in critically ill patients is now recognized as a major public health problem, affecting up to 80% of mechanically ventilated adult ICU patients, and costing $4 to $16 billion annually in the United States alone.311–314 Over the past decade, the study of delirium in ICU patients has expanded significantly.315–319 But the underlying pathophysiology of delirium in critically ill patients remains poorly understood.320–322
Impact of Delirium on ICU Patient Outcomes. Delirium, as a manifestation of acute brain dysfunction, is an important independent predictor of negative clinical outcomes in ICU patients, including increased mortality, hospital LOS, cost of care, and long-term cognitive impairment consistent with a dementia-like state.313,320–324 ICU team practices affect the incidence of delirium and its consequences.220,222,325–329 Critical care professionals strive to understand which aspects of delirium are predictable, preventable, detectable, and treatable.
Preventing, Detecting, and Treating Delirium in ICU Patients. Delirium may be a disease-induced syndrome (e.g., organ dysfunction in severe sepsis), for which timely management of the cause or causes is essential in order to reduce the incidence, severity, and duration of delirium. Iatrogenic (e.g., exposure to sedative and opioid medications) or environmental (e.g., prolonged physical restraints or immobilization) factors may also contribute to delirium in ICU patients. ICU patients should be evaluated for identifiable and avoidable risk factors, and therapeutic interventions should be assessed in terms of their likelihood of either causing or exacerbating delirium in individual patients. Delirium prevention strategies can be categorized as nonpharmacologic (e.g., early mobilization), pharmacologic, and combined pharmacologic/nonpharmacologic approaches. Monitoring critically ill patients for delirium with valid and reliable delirium assessment tools enables clinicians to potentially detect and treat delirium sooner, and possibly improve outcomes.
Patients are frequently given various medications to reduce the severity and duration of delirium once it has occurred. Although no double-blind, randomized, placebo-controlled trials which are adequately powered have established the efficacy or safety of any antipsychotic agent in the management of delirium in ICU patients, administration of antipsychotic medications is endorsed by various international guidelines,330–339 and most critical care specialists use these medications to treat delirious patients.164 In the previous version of these guidelines, the recommended use of haloperidol for the treatment of delirium was a Level C recommendation based only on a case series. These data did not meet the evidence standard for this version of the guidelines. No recent prospective trials have verified the safety and efficacy of haloperidol for the treatment of delirium in adult ICU patients. Data on the use of other antipsychotics in this patient population are similarly sparse. A recent Cochrane Review on using antipsychotics for the treatment of delirium did not address the issue of antipsychotic use in ICU patients.340 Robust data on haloperidol in non-ICU patients that could potentially be applied to the ICU patient population are lacking. Further research is needed to determine the safety and efficacy of using antipsychotics in general, including haloperidol, to treat delirium in ICU patients.
Delirium due to Drug and/or Alcohol Withdrawal. During their ICU stay, critically ill patients may develop a subcategory of delirium related to either drug or alcohol withdrawal, which usually manifests as a hyperactive type of delirium. Withdrawal symptoms may result from abrupt discontinuation of: 1) illicit or prescription drugs that patients were taking chronically; 2) sedatives or opioids administered as part of routine ICU care; or 3) chronic ethanol use. An exhaustive review of the pathophysiology, diagnosis, and treatment of drug and alcohol withdrawal is beyond the scope of these guidelines. Clinicians are referred to other clinical practice guidelines for more detail.341–343
Patients with long-term exposure to high-dose opiates or sedatives may develop physiologic dependence, and abrupt discontinuation may cause drug withdrawal symptoms.344 Signs and symptoms of acute opiate withdrawal include sweating, piloerection, mydriasis, lacrimation, rhinorrhea, vomiting, diarrhea, abdominal cramping, tachycardia, hypertension, fever, tachypnea, yawning, restlessness, irritability, myalgias, increased sensitivity to pain, and anxiety. The onset of symptoms can occur < 12 hrs following discontinuation of opioids, or be precipitated by either the administration of the opioid antagonist, naloxone, or mixed agonist/antagonists such as nalbuphine.345,346 Prolonged benzodiazepine use in ICU patients may lead to withdrawal symptoms when the drug is abruptly discontinued, manifesting as anxiety, agitation, tremors, headaches, sweating, insomnia, nausea, vomiting, myoclonus, muscle cramps, hyperactive delirium, and occasionally seizures.344 Reversing the sedative effects of benzodiazepines following long-term exposure with the benzodiazepine receptor antagonist flumazenil may induce symptoms of benzodiazepine withdrawal.347,348 Adult ICU patients receiving dexmedetomidine infusions for up to 7 days have developed withdrawal symptoms, most commonly nausea, vomiting, and agitation, within 24–48 hrs of discontinuing dexmedetomidine.349 In the largest study to date looking prospectively at the effects of sedation of ICU patients with dexmedetomidine vs. midazolam, the incidence of withdrawal following discontinuation of dexmedetomidine was 4.9% vs. 8.2% in midazolam-treated patients (p = 0.25).220 Signs and symptoms of opioid and sedative withdrawal in critically ill patients may be overlooked or attributed to other causes, such as alcohol or illicit drug withdrawal.
In the past decade, little was published on the pathophysiology and incidence of drug withdrawal from opioids and sedative agents administered to adult ICU patients. Most studies are retrospective and include patients who have received a variety of sedative and analgesic agents, making it difficult to determine specific incidences and risk factors for drug withdrawal in these patients.344,350 One small prospective study assessed adult ICU patients for signs and symptoms of withdrawal following discontinuation of sufentanil infusions used concurrently with either midazolam or propofol infusions.351 Patients in the sufentanil/midazolam group were sedated for 7.7 days vs. 3.5 days for the sufentanil/propofol group. Withdrawal symptoms occurred more frequently in the midazolam group (35% vs. 28% with propofol). Although specific recommendations are lacking for the prophylaxis or treatment of opioid or sedative withdrawal in ICU patients, opioids and/or sedatives administered for prolonged periods (i.e., days) should be weaned over several days in order to reduce the risk of drug withdrawal.
Ethanol (ETOH) dependence is present in 15%–20% of all hospitalized patients.352 Between 8% and 31% of hospitalized patients with ETOH dependence, especially surgical and trauma patients, will go on to develop Alcohol Withdrawal Syndrome (AWS) during their hospital stay, with signs and symptoms of neurologic and autonomic dysfunction.353–355 Symptoms of AWS range from mild to life-threatening.356 Up to 15% of hospitalized patients with AWS experience generalized tonic-clonic seizures, and 5% develop delirium tremens (DTs), a life-threatening combination of central nervous system excitation (agitation, delirium, and seizures) and hyperadrenergic symptoms (hypertension, tachycardia, arrhythmias).357 ICU patients with severe AWS may exhibit prolonged ventilator dependence and extended ICU stays as a result of persistent delirium.353–355
Prior ethanol dependence is often underestimated in ICU patients, making identification of patients at risk for AWS or DTs difficult. Screening tools for AWS or DTs have not been fully validated in the critical care setting. Differentiating between delirium due to alcohol withdrawal vs. other causes may be difficult. Symptom-oriented treatment of AWS symptoms with drug dosing as needed to specifically target agitation, psychosis, and autonomic hyperactivity decreases the severity and duration of AWS, and medication requirements in ICU patients.358 Benzodiazepines are considered the mainstay of alcohol withdrawal treatment, despite uncertainty about their effectiveness and safety.320 To date, no published studies have compared the safety and efficacy of treating symptoms of severe AWS with dexmedetomidine vs. benzodiazepines. Diagnosis and management of delirium due to AWS in ICU patients remains challenging. It is beyond the scope of these guidelines to describe the validity of alcohol withdrawal measurement tools, of alcohol withdrawal prevention, or of its treatment in the critical care setting.
Delirium: Questions, Statements, and Recommendations.
1. Outcomes Associated With Delirium in ICU Patients
Question: What outcomes are associated with delirium in adult ICU patients? (descriptive)
Answer: Delirium is associated with increased mortality (A), prolonged ICU and hospital LOS (A), and development of post-ICU cognitive impairment in adult ICU patients (B).
Rationale: Numerous prospective cohort studies have demonstrated that patients who develop delirium are at increased risk for adverse outcomes both in the ICU and after discharge. This risk is independent of preexisting comorbidities, severity of illness, age, and other covariates that might be merely associative. Eleven prospective cohort studies examined the relationship between delirium while in the ICU and mortality at various time points: ICU discharge (n = 5), hospital discharge (n = 4), 30 days (n = 1), 3 months (n = 1), 6 months (n = 3), and 12 months (n = 1).318,319,321,322,359–365 All studies classified delirium as present on one or more ICU days; three studies also examined the relationship between delirium duration and mortality.320,321,366 Delirium was an independent predictor of mortality in 11 of 15 studies, including the three studies with a high quality of evidence.320,321,366 Duration of delirium (after adjusting for coma and in some cases psychoactive medication exposure) was significantly associated with 6- and 12-month mortality rates. In two cohort studies, duration of delirium consistently portended a 10% increased risk of death per day (after adjusting for covariates and appropriately treating delirium as a time-dependent covariate).320,321
Nine prospective cohort studies examined the relationship between one or more days of delirium in the ICU and ICU and/or hospital LOS, as well as duration of mechanical ventilation.318,319,322,323,360,361,363,364,367 Delirium was an independent predictor of duration of mechanical ventilation in four studies360,363,364,367 and of ICU LOS in four studies.318,319,364,367 Both of these outcome variables are particularly at risk for immortal time bias, which is introduced when the exposure to a treatment or independent variable (in this case, delirium) can change daily during the actual outcome measurement (in this case, either duration of mechanical ventilation or ICU LOS).368 It is therefore important that the predictive relationship between delirium and hospital LOS was also strong in seven of nine studies,318,319,322,323,361,364,367 including three high-quality studies that accounted for immortal time bias.318,322,368
Two prospective cohort studies examined the relationship between delirium in the ICU and subsequent cognitive impairment. One study of moderate quality described an association between the presence of delirium on one or more ICU days and a higher incidence of cognitive dysfunction at hospital discharge.322 In a recent prospective cohort study of moderate quality, increasing duration of delirium in ICU patients was associated with significantly greater cognitive impairment in these patients at 3 and 12 months.324
2. Detecting and Monitoring Delirium
a.Question: Should ICU patients be monitored routinely for delirium with an objective bedside delirium instrument? (actionable)
Answer: We recommend routine monitoring for delirium in adult ICU patients (+1B).
Rationale: Delirium is common in both mechanically ventilated14,220,222,308,360,369,370 and nonmechanically ventilated ICU patients.309,359,371–379 ICU personnel often underestimate the presence of delirium in patients because it frequently presents as hypo-active rather than hyperactive delirium.372,380 Delirium can be detected in both intubated and nonintubated ICU patients using valid and reliable tools. In most studies, delirium detection was improved when caregivers used a valid and reliable delirium assessment tool,367 also allowing them to reassure frightened and disoriented patients.381 Delirium monitoring rationale includes: 1) most informed patients at moderate to high risk want to be monitored for delirium; 2) high-quality cohort data relating delirium to critical outcomes shows high delirium “miss rates” in the absence of monitoring; 3) clinicians have successfully implemented ICU delirium monitoring programs on a large-scale, using assessment tools recommended in these guidelines; and 4) policy makers can adopt delirium assessment as part of routine, high-quality care in most ICUs.254,372,374,382,383 Based on moderate evidence, we issue a strong recommendation that ICU patients at moderate to high risk for delirium (e.g., patients: with a baseline history of alcoholism, cognitive impairment, or hypertension; with severe sepsis or shock; on mechanical ventilation; or receiving parenteral sedative and opioid medications) should be routinely monitored, at least once per nursing shift, for the development of delirium using a valid and reliable delirium assessment tool.
b.Question: Which instruments available for delirium monitoring have the strongest evidence for validity and reliability in ventilated and nonventilated medical and surgical ICU patients? (descriptive)
Answer: The Confusion Assessment Method for the ICU (CAM-ICU) and the Intensive Care Delirium Screening Checklist (ICDSC) are the most valid and reliable delirium monitoring tools in adult ICU patients (A).
Rationale: Five delirium monitoring tools were evaluated for use in ICU patients: Cognitive Test for Delirium (CTD), CAM-ICU, Delirium Detection Score (DDS), ICDSC, and Nursing Delirium Screening Scale (Nu-DESC). Table 8 compares their psychometric properties. Both the CAM-ICU308,359,371–374,384–387 and ICDSC309,371 demonstrate very good psychometric properties (i.e., validity and reliability), and are explicitly designed for use in ICU patients both on and off mechanical ventilation. Translated into over 20 languages, these tools are currently in use worldwide.315 The CAM-ICU and ICDSC have shown high inter-rater reliability when tested by ICU nurses and intensivists.308,309,373 They both demonstrated high sensitivity and specificity when tested against the American Psychiatric Association’s criteria for delirium.319,359,379 Predictive validation of the presence of delirium, as detected with the CAM-ICU or ICDSC, was associated with clinical outcomes such as increased ICU and hospital LOS318,319,322,323,360,361,363,364,367 and higher risk of mortality.318,319,321,322,359–365 Based on our review of the literature, both the CAM-ICU and ICDSC are valid, reliable, and feasible tools to detect delirium in ICU patients.254,309 While the CTD388–390 and Nu-DESC379
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


