Practical Biomarkers for Female Genital Tract Lesions
Introduction
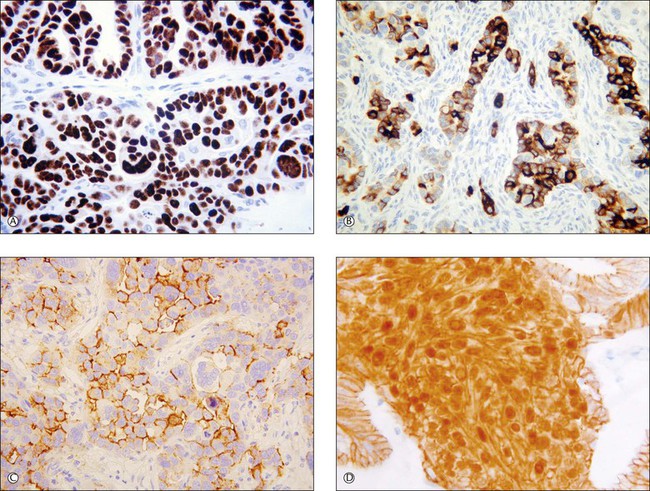
Recent years have witnessed a marked expansion in the use of immunohistochemical markers in gynecologic pathology.1,2 Most relate to the use of antibodies in the diagnosis of gynecologic neoplasms but some markers have prognostic or predictive value. In general when immunohistochemistry is used diagnostically, panels of markers provide better information than reliance on a single antibody. As anticipated historically, most antibodies, although initially thought specific for a given tumor, later have proven to have a broader range of reactivity than is initially suspected, with reactivity in a more diverse set of tumor types. This chapter provides an overview of the antibodies commonly used in the diagnosis of gynecologic lesions grouped as to function or type. The value of markers as prognostic or predictive factors is discussed where appropriate, understanding only a handful are sufficiently informative to be used in routine practice. Different markers result in different staining patterns, for example nuclear, membranous, cytoplasmic, or a combination (Figure 36.1), and knowledge of the expected staining patterns is essential when interpreting immunohistochemical slides.
Broad Spectrum Differentiation Markers
Epithelial Markers
Cytokeratins
Cytokeratins (CKs) belong to the group of intermediate filament proteins that are intermediate between microfilaments and microtubules. They constitute the cytoskeletal structure of virtually all epithelial cells, both benign and malignant. Some nonepithelial cell types and tumors derived from these may also express CKs. The cytokeratin family of proteins, which are coded by different genes, has been numbered (numbers 1–20).3 The expression of the various CKs in cells and tumors depends on their embryonic origin and also the degree of cellular differentiation.3 One broad group of CKs, type I (CK9–20), has an acidic isoelectric point. The other group, type II (CK1–8), has a basic neutral isoelectric point. Antibodies against CKs help confirm the epithelial lineage of a neoplasm. In this regard, monoclonal antibodies, such as AE1/3 and CAM 5.2, are available that recognize multiple members of the CK family. AE1/3 reacts against almost all of the CK family of proteins (AE1 recognizes most of the type 1 CKs whereas AE3 reacts against most of the type II CKs) while CAM 5.2 reacts against CK8 and CK18. Additionally, antibodies are available that react against specific CKs, for example, CK7, CK20, or CK5/6. The following sections detail the use of various anti-CK antibodies in the diagnosis of female genital tract lesions.
Broad Spectrum Cytokeratins
Broad spectrum anti-CK antibodies, such as AE1/3, often prove of value in confirming the epithelial lineage of a neoplasm. For example, in distinguishing a poorly differentiated carcinoma from sarcoma, melanoma, or lymphoma, reactivity with AE1/3, especially if widespread, favors a diagnosis of carcinoma. However, anti-CK antibodies, such as AE1/3, occasionally react with tumors of melanocytic, mesenchymal, and lymphoid origin.4 Smooth muscle tumors may also react with anti-CK antibodies.5 This may result in diagnostic difficulties, especially if dealing with an epithelioid smooth muscle neoplasm, and underscores the necessity of using panels of antibodies.
Endometrial stromal neoplasms may also be CK positive.6 Broad spectrum anti-CK antibodies are reactive with trophoblastic cells and may be useful in distinguishing intermediate trophoblast from decidua, thus confirming the presence of a placental site.
CK7 and 20
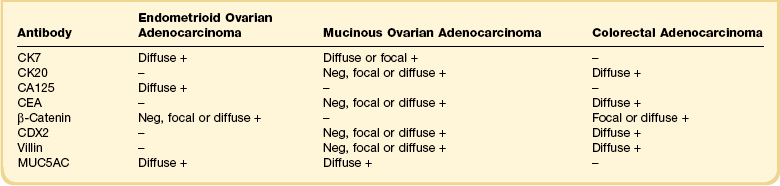
A combination of antibodies against CK7 and 20 (differential CK staining) has been widely used in ovarian and peritoneal pathology to distinguish between a primary ovarian or peritoneal adenocarcinoma and a metastatic adenocarcinoma, especially of colorectal origin.1,2,7–9 In general, primary ovarian carcinomas of serous, endometrioid, and clear cell type exhibit diffuse CK7 reactivity and are negative with CK20. Primary ovarian mucinous neoplasms exhibit a more variable immunophenotype. In general, they are diffusely reactive with CK7 and nonreactive or focally reactive with CK20. However, there are exceptions with occasional primary ovarian mucinous neoplasms, especially those of intestinal type, being diffusely CK20 positive. In the distinction between a primary ovarian endometrioid adenocarcinoma and a metastatic colorectal adenocarcinoma with an endometrioid appearance, differential CK staining is very useful alone or as part of a larger panel (Table 36.1). Endometrioid adenocarcinoma is usually diffusely CK7 reactive and CK20 negative while colonic carcinoma generally exhibits the opposite immunophenotype. In the case of an ovarian mucinous neoplasm, differential CK staining is not uncommonly difficult to interpret since many primary ovarian mucinous neoplasms may be CK20 reactive and mucinous colorectal adenocarcinoma may be focally CK7 positive. Rectal adenocarcinomas may also be CK7 positive. Additionally mucinous tumors arising in a teratoma often exhibit a large intestinal immunophenotype with diffuse CK20 immunoreactivity. In this regard, other antibodies (discussed in the following sections) are sometimes of value.
Differential CK staining is of limited value in distinguishing between a primary ovarian carcinoma and a metastatic adenocarcinoma from other organs, since many of these tumors exhibit a CK7-positive/CK20-negative or focally positive immunophenotype (Table 36.2). However, dual CK7 and CK20 reactivity raises the possibility of a primary neoplasm in the stomach, pancreas, biliary tree, or urinary bladder.1,2,7–9 Breast, pulmonary, endometrial, and endocervical adenocarcinomas are most commonly CK7 positive and CK20 negative.
Table 36.2
Typical Differential Cytokeratin Reaction Patterns in Tumors
| CK7 | CK20 | |
| Mucinous ovarian adenocarcinoma | + | − or + |
| Non-mucinous ovarian adenocarcinoma | + | − |
| Colorectal adenocarcinoma | − | + |
| Cervical adenocarcinoma | + | − |
| Endometrial adenocarcinoma | + | − |
| Pancreatic/biliary adenocarcinoma | + | + or − |
| Gastric adenocarcinoma | + | + or − |
| Renal cell carcinoma | − | − |
| Bladder adenocarcinoma | + | + or − |
| Breast adenocarcinoma | + | − |
| Pulmonary adenocarcinoma | + | − |
| Mesothelioma | + | − |
CK7 and CK20 staining also helps to confirm that most cases of pseudomyxoma peritonei in women are of appendiceal (or more rarely colorectal) origin rather than originating from a ruptured ovarian mucinous neoplasm.10 In cases of pseudomyxoma peritonei with coexistent appendiceal and ovarian mucinous neoplasms, the epithelial elements in all locations, i.e., the appendix, ovary, and peritoneum, are usually diffusely CK20 positive and negative or focally positive with CK7, in keeping with an intestinal origin.
CK7 may be of value in the vulva in confirming a diagnosis of Paget disease and excluding mimics such as malignant melanoma and mycosis fungoides. The cells of primary vulvar Paget disease are usually intensely CK7 positive,11,12 a feature that may assist in assessment of margins. Strong CK20 reactivity should result in consideration of secondary Paget disease, from either the colorectum or urinary tract.11,12
Ck5/6
CK5/6 is often reactive in mesothelial cells (benign or malignant) and is helpful to distinguish a mesothelial from a serous epithelial proliferation (benign, borderline, or malignant); the latter is usually negative.13 In this regard, CK5/6 should be used as part of a panel that may include Ber-EP4 (an epithelial marker reactive in most epithelial lesions and generally negative in mesothelial lesions). Other antibodies generally reactive in mesothelial lesions are calretinin, HBME1, thrombomodulin, D2-40, and CD44H (generally negative in epithelial lesions).13,14 CK5/6 is more likely to be positive in squamous than glandular neoplasms and this may be useful in diagnosis.
Other Cytokeratins
Although the remaining specific CKs have found little place in diagnostic gynecologic pathology, there are a few exceptions. Staining with the high molecular weight CK34β E12 may assist in highlighting the basal cell layer in ectopic prostatic tissue within the cervix.15 CK18 is especially likely to be positive in undifferentiated endometrial carcinoma and this marker may be useful in distinguishing undifferentiated endometrial carcinoma from undifferentiated sarcoma.16
Epithelial Membrane Antigen and Ber-EP4
Epithelial membrane antigen (EMA), a glycoprotein found in human milk fat globule membranes, and Ber-EP4, an epithelial-specific antigen to a membrane-bound glycoprotein, help to confirm that a neoplasm has an epithelial lineage. Trophoblast and trophoblastic neoplasms are also reactive. Both markers are commonly used in panels to distinguish an ovarian adenocarcinoma (reactive) from a sex cord–stromal tumor (negative).1,2,17 Ber-EP4 is useful in distinguishing a serous proliferation of the ovary or peritoneum (reactive) from mesothelial derived lesions (negative). Although EMA reactivity is rare in ovarian sex cord–stromal tumors, focal immunoreactivity has been found in 50% of a small series of juvenile granulosa cell tumors.18 EMA is generally negative in female adnexal tumor of wolffian origin (FATWO). This is diagnostically useful since FATWO may be confused with an epithelial neoplasm, which is usually EMA reactive. EMA is often positive in undifferentiated endometrial carcinoma and may be useful in distinguishing this from undifferentiated sarcoma.16
Mesenchymal Cell Markers
Vimentin
In the cervix, vimentin may be used as an aid to distinguish between tuboendometrial metaplasia and endometriosis (usually vimentin reactive) and adenocarcinoma in situ (AIS) (usually vimentin negative).19 Vimentin may also be useful in differentiating between an endometrial adenocarcinoma of endometrioid type and an endocervical adenocarcinoma of usual type.20 The former usually exhibits diffuse vimentin reactivity whereas endocervical adenocarcinomas are generally negative.
Vimentin may help distinguish between a microglandular variant of endometrioid or mucinous adenocarcinoma of the endometrium (usually vimentin reactive) and cervical microglandular hyperplasia (vimentin negative).21
Smooth Muscle Markers
The three most common smooth muscle markers are alpha smooth muscle actin (α-SMA), desmin, and h-caldesmon. These are helpful in several diagnostic scenarios, especially in confirming smooth muscle differentiation within a neoplasm within the female genital tract. Some smooth muscle neoplasms, especially malignant and epithelioid variants, are negative or only focally reactive.22 h-Caldesmon is the most specific, but is less sensitive than desmin. However, it should be kept in mind that some tumors that may mimic smooth muscle neoplasms, such as gastrointestinal stromal tumor (GIST), may be h-caldesmon positive.23 Desmin is not a specific smooth muscle marker, as it also stains skeletal muscle.
In the uterus, the main value of smooth muscle markers is in establishing a diagnosis of a smooth muscle neoplasm, either benign or malignant. An antibody panel composed of desmin, h-caldesmon, and CD10 (discussed later) helps distinguish cellular and other morphologically problematic leiomyomatous neoplasms from endometrial stromal neoplasms24,25 (Table 36.3). In general, leiomyomatous neoplasms are diffusely reactive with desmin and h-caldesmon. CD10 is usually negative or focally reactive, although some cellular leiomyomatous neoplasms and leiomyosarcomas may be diffusely reactive. Endometrial stromal neoplasms are usually diffusely CD10 reactive and desmin and h-caldesmon usually negative. Sometimes, desmin and h-caldesmon, are focally positive, although occasional examples are diffusely positive, especially with desmin. α-SMA is of limited value since many endometrial stromal neoplasms are diffusely reactive. Uterine tumor resembling ovarian sex cord tumor, sex cord-like areas within endometrial stromal neoplasms, and uterine perivascular epithelioid cell tumor (PEComa) are also variably reactive with smooth muscle markers.26
Table 36.3
Typical Reaction Patterns in Endometrial Stromal and Smooth Muscle Neoplasm
| Antibody | Smooth Muscle Neoplasm | Endometrial Stromal Neoplasm |
| Desmin | Diffuse + | − or focal + |
| α-SMA | Diffuse + | Neg, focal or diffuse + |
| h-Caldesmon | Diffuse + | − |
| CD10 | Neg, focal or diffuse + | Diffuse + |
| Oxytocin receptor | Diffuse + | − |
In the cervix, α-SMA may be useful in distinguishing normal endocervical glands or non-neoplastic endocervical glandular lesions from the well-differentiated glands of adenoma malignum. The presence of many α-SMA reactive stromal cells suggests a desmoplastic response to tumor.27
In the vulvovaginal region, many of the wide range of relatively site-specific mesenchymal neoplasms such as angiomyofibroblastoma, aggressive angiomyxoma, and superficial myofibroblastoma of the lower female genital tract react with smooth muscle markers, especially desmin.28 Thus, none of these markers are of value in confirming that a mesenchymal lesion represents a leiomyomatous neoplasm. However, negative staining with smooth muscle markers is of value in diagnosing cellular angiofibroma which, in contrast to most other neoplasms in the differential diagnosis, does not usually react.28
Another tumor that commonly shows reactivity with desmin is intra-abdominal desmoplastic small round cell tumor (IADSRCT; in females this may clinically mimic a primary ovarian neoplasm), usually with paranuclear dot-like immunoreactivity.29 This is useful in diagnosis, especially in differentiating this neoplasm from the wide range of ‘small blue cell tumors’ that may involve the ovary and peritoneum. Desmin sometimes assists in the distinction between benign and malignant mesothelial proliferations. Benign mesothelial cells are usually desmin reactive while the cells of malignant mesothelioma are generally negative, although there is significant overlap.
Skeletal Muscle Markers
A variety of skeletal muscle markers are available, including myoglobin, myogenin, myoD1, and sarcomeric actin. These assist in confirming rhabdomyosarcomatous differentiation within a neoplasm such as carcinosarcoma. Embryonal rhabdomyosarcomas are rare in general in the female genital tract and are most common in the vagina where the differential diagnosis usually includes the ‘small blue cell tumors of childhood.’ Rhabdomyosarcomas of embryonal, alveolar, and pleomorphic types rarely arise in the cervix, uterine corpus, or ovary. Myogenin and myoD1 are markers which have been generated against intranuclear transcription factors.30 They are relatively specific nuclear markers of skeletal muscle and are the antibodies of choice in demonstrating skeletal muscle differentiation within a neoplasm, having superseded myoglobin and sarcomeric actin.
Endometrial Stromal Markers
CD10
CD10 is useful in diagnosing an endometrial stromal neoplasm, since most endometrial stromal nodules and endometrial stromal sarcomas (low-grade endometrial stromal sarcomas) exhibit diffuse intense reactivity, although fibrous variants may be negative.24,25 In the distinction between an endometrial stromal and a smooth muscle neoplasm, CD10 should be used as part of a panel (Table 36.3), since conventional uterine smooth muscle tumors may be focally reactive and it is not uncommon for cellular and highly cellular leiomyomas (which are not infrequently mistaken for endometrial stromal neoplasms) and leiomyosarcomas to be diffusely reactive.
CD10 is also characteristically reactive in mesonephric glandular lesions within the female genital tract. Mesonephric remnants throughout the female genital tract usually exhibit luminal CD10 reactivity.31,32 CD10 reactivity in a benign cervical glandular lesion is good evidence of a mesonephric origin,31 although so-called ectopic prostatic tissue may also be reactive.15 However, CD10 is of limited value in confirming a mesonephric origin for an adenocarcinoma since many cervical and endometrial adenocarcinomas are also reactive.31 FATWO may be CD10 reactive.33
Other uses of CD10 staining in gynecologic pathology include the distinction between a metastatic renal clear cell carcinoma involving the ovary (CD10 reactive)34 and a primary ovarian clear cell carcinoma (usually CD10 negative). In addition, most trophoblastic cell populations and trophoblastic neoplasms are reactive.32 A wide range of other gynecologic neoplasms may be CD10 reactive, including leiomyosarcoma, carcinosarcoma, undifferentiated uterine sarcoma, ovarian sex cord–stromal tumors, uterine tumors resembling ovarian sex cord tumor, and mixed tumor of the vagina.35 However, CD10 immunoreactivity in these neoplasms is inconsistent and unlikely to be of diagnostic value. In summary, CD10 is expressed in a much wider range of gynecologic neoplasms than was originally appreciated and, when used as an aid to diagnosis, should always be part of a panel, which will depend on the differential diagnoses under consideration.
Mesothelial Markers
Calretinin
Calretinin is a 29 kDa calcium-binding protein, best known for its role in the diagnosis of mesothelioma. In the distinction between a mesothelioma and an adenocarcinoma, calretinin should be used as part of a panel. Calretinin and Ber-EP4 are the two most useful antibodies to distinguish between a serous epithelial and a mesothelial proliferation.14 Most serous proliferations are Ber-EP4 reactive and calretinin negative; the converse is the rule for mesothelial lesions. Nuclear reactivity with calretinin is more specific than cytoplasmic staining for mesothelial cells.14
Calretinin is also expressed in most ovarian sex cord–stromal tumors, being more sensitive but less specific than inhibin.36,37 Calretinin is more likely to be reactive in an ovarian fibroma than inhibin.
In general, neoplasms reactive for inhibin also show reactivity with calretinin. Other gynecologic neoplasms that may show calretinin reactivity include FATWO, uterine tumor resembling ovarian sex cord tumor, sex cord-like areas within endometrial stromal neoplasms, and adenomatoid tumor. Mesonephric lesions, both benign and malignant, within the cervix and elsewhere in the female genital tract may show reactivity.31
Blood Vessel Markers
CD34
CD34, a single chain transmembrane glycoprotein, leukocyte differentiation antigen, is expressed by hematopoietic progenitor cells, endothelial cells, and connective tissue cells, such as skin fibroblasts. CD34 is variably expressed in several vulvovaginal mesenchymal lesions, including aggressive angiomyxoma, cellular angiofibroma, and superficial myofibroblastoma of the lower female genital tract.28 Solitary fibrous tumors rarely occur at various sites within the female genital tract and are CD34 reactive. Endometrial stromal neoplasms are usually CD34 negative, which may be of use in differential diagnosis in that many mimics are reactive.38 Metastatic GIST in the ovary is usually CD34 positive,23 as are rare primary GISTs arising in the rectovaginal septum or elsewhere in the female genital tract.39
Narrow Spectrum Differentiation Markers
Trophoblastic Markers
β-hCG
β-hCG reacts against syncytiotrophoblast but not cytotrophoblast. Choriocarcinoma shows the strongest and most diffuse reactivity. Placental site trophoblastic tumor (PSTT) and epithelioid trophoblastic tumor are less reactive. Trophoblastic elements in mixed germ cell tumors show reactivity, as do isolated syncytiotrophoblast cells in neoplasms such as dysgerminoma and endometrial carcinoma. β-hCG may be reactive on occasions in a variety of nontrophoblastic neoplasms, such as cervical squamous carcinoma.40
Mel-CAM (CD146)
Mel-CAM is expressed in implantation site intermediate trophoblastic cells.41 Chorion-type intermediate trophoblastic cells are usually negative or focally reactive. Placental site trophoblastic tumor and exaggerated placental site, lesions of implantation site intermediate trophoblast, express Mel-CAM, whereas placental site nodule and epithelioid trophoblastic tumor, lesions of chorion-type intermediate trophoblast, are usually negative. In distinguishing placental site trophoblastic tumor from exaggerated placental site, double immunohistochemical staining with Mel-CAM and MIB1 is of value.41 In exaggerated placental site, the MIB1 index in intermediate trophoblastic cells is close to zero whereas it is significantly elevated (14 ± 6.9%) in placental site trophoblastic tumor.41
HLA-G
HLA-G is expressed in all known trophoblastic tumors, including choriocarcinoma, placental site trophoblastic tumor, and epithelioid trophoblastic tumor, as well as in benign trophoblastic lesions, such as placental site nodule and exaggerated placental site.42 HLA-G is generally negative in nontrophoblastic uterine neoplasms.64 HLA-G reactivity has been demonstrated in some ovarian carcinomas.43
Melanocytic Markers
HMB45
HMB45 is probably the most specific marker of malignant melanoma, and it is melanosome associated. HMB45 reactivity is useful to confirm the diagnosis of malignant melanoma at any site within the female genital tract, most commonly in the vulva or vagina. Metastatic melanoma in the ovary can assume an unusual array of morphologic appearances and easily fool the pathologist if there is no history of melanoma. HMB45 may assist in this regard. However, occasional ovarian steroid cell tumors, which may mimic melanoma, are HMB45 reactive.44 Another neoplasm characteristically reactive with HMB45 is PEComa.26 This is an uncommon neoplasm, which in the female genital tract most often involves the myometrium.41 Uterine epithelioid leiomyosarcomas with a clear cell appearance may also express HMB45.45
Melan-A (MART-1)
Melan-A, also known as MART-1, is another melanocytic marker of value in the diagnosis of malignant melanoma. Ovarian sex cord–stromal tumors are also commonly reactive.46
Neuroendocrine Markers
There are various neuroendocrine markers in widespread use, including chromogranin, CD56, synaptophysin, and PGP9.5. These vary in their specificity and sensitivity. For example, chromogranin is a highly specific but poorly sensitive marker while CD56 is sensitive but lacks specificity. Reactivity with neuroendocrine markers is not necessary to establish a diagnosis of a small cell neuroendocrine carcinoma since many of these are sparsely granulated and negative with neuroendocrine markers. In contrast, reactivity with neuroendocrine markers is a prerequisite for a diagnosis of large cell neuroendocrine carcinoma. Rarely paraganglioma and typical and atypical carcinoid occur within the female genital tract and are reactive. A high percentage of ovarian sex cord–stromal tumors are CD56 positive.47 Undifferentiated uterine carcinomas may be focally positive with neuroendocrine markers.16
Lymphoid Markers
Several markers may assist in the diagnosis of a low-grade endometritis, which usually depends on the morphologic identification of plasma cells that may be difficult to visualize with H&E when few in number. In the normal endometrium, most lymphoid cells are of T-cell or natural killer (NK) cell lineage. B-lymphocytes account for less than 1% of endometrial leukocytes, and are mainly located in lymphoid aggregates. In endometritis, the number of T-lymphocytes and NK cells does not differ from controls. However, the use of B-lymphoid markers, such as CD20 and CD79a, reveals substantially increased numbers of B-cells in unusual locations such as beneath the surface epithelium and intraepithelially.48 Markers against plasma cells, such as syndecan and VS38, may also assist in diagnosing endometritis.49
Markers of Altered Function in Disease States
Tumor Markers
Carcinoembryonic Antigen
Monoclonal CEA helps distinguish non-mucinous ovarian adenocarcinomas (usually negative) from colorectal adenocarcinoma (usually reactive), when used as part of a panel.1,2 Primary ovarian mucinous neoplasms are often reactive. Adenocarcinomas from other organs, such as pancreas and stomach, are variably reactive.
CEA is useful as part of a panel to help distinguish endometrioid-type endometrial adenocarcinoma from endocervical adenocarcinoma of usual type.20 Endocervical adenocarcinomas are usually, but not always, diffusely reactive with CEA. Primary endometrioid adenocarcinomas of the corpus are negative or focally reactive, although the associated squamous elements may be diffusely reactive. CEA staining patterns of primary mucinous adenocarcinoma of the endometrium are not well studied, but at least a proportion are reactive. CEA is usually reactive in cervical AIS and negative in benign endocervical glandular lesions.50
CA125 (Oc125)
Immunohistochemical staining with CA125 helps to distinguish between a primary and a metastatic ovarian adenocarcinoma and in the evaluation of a disseminated peritoneal tumor in a female.1,2 In general, primary ovarian (or peritoneal) adenocarcinomas of serous, endometrioid, and clear cell types exhibit diffuse CA125 reactivity. Primary ovarian mucinous carcinomas are usually negative, as are colorectal adenocarcinomas. In distinguishing primary ovarian adenocarcinoma from a metastatic colorectal adenocarcinoma, CA125 should be used in a panel (Table 36.2) that could include CK7, CK20, estrogen receptor (ER), CDX2, and CEA. CA125 reactivity is not specific for an ovarian adenocarcinoma, as primary adenocarcinomas of many other organs, including pancreas, breast, lung, cervix, and uterine corpus exhibit reactivity in a proportion of cases. Mesotheliomas are commonly reactive, as are benign mesothelial cells.51
Inhibin
Inhibin is a dimeric 32 kDa peptide hormone composed of an α- and a β-subunit and produced by ovarian granulosa and theca cells. Individual antibodies are available against each subunit. Most ovarian sex cord–stromal tumors show focal to diffuse cytoplasmic reactivity with inhibin (antibody against α-subunit), although fibroma, poorly differentiated Sertoli–Leydig, and sarcomatoid granulosa cell tumors are sometimes negative.52,53 Since ovarian sex cord–stromal neoplasms may be morphologically confused with a wide range of neoplasms, especially endometrioid carcinomas, immunohistochemical evaluation with inhibin (and other sex cord–stromal markers such as calretinin) may be extremely useful in primary diagnosis and also when confirming a metastatic neoplasm, which may occur years or decades later. In distinguishing between a sex cord–stromal tumor and an endometrioid carcinoma, the former is almost always negative with EMA17 (Table 36.4). Ovarian sex cord–stromal tumors are usually negative with CK7 but may be focally positive with broad spectrum anti-CK antibodies. Most carcinomas are negative with inhibin, although occasional tumors are focally reactive. Activated ovarian stromal cells that occur in association with and at the periphery of any ovarian neoplasm may be reactive with sex cord–stromal markers, so close attention must be paid to the cellular morphology of the particular clusters that are immunohistochemically reactive.
Table 36.4
Antibodies of Value in Distinguishing between Ovarian Endometrioid Adenocarcinoma and Sex Cord–Stromal Tumor
| Antibody | Endometrioid Adenocarcinoma | Sex Cord–Stromal Tumor |
| CK7 | + | − |
| EMA | + | − |
| α-Inhibin | − | + |
| Calretinin | − or + | + |
| Steroidogenic factor 1 | − | + |
| Broad spectrum CKs | Diffuse + | − or focal + |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


