Clinical Photograph of Poroma Clinical photograph shows a traumatized poroma on the lower back of an adult male, which presented as an irritated polypoid lesion.
Poroma With Squamoid Features Low magnification of a poroma with squamoid features shows a basaloid to squamoid-appearing neoplasm with multiple anastomosing connections between thickened cords of tumor cells and to epidermis. Note the ectatic ductal space on the left .
Poroma With Clear Cell Features Scanning magnification of a poroma with clear cell features shows a basaloid to clear cell neoplasm with multiple anastomosing connections between thickened cords of tumor cells and to epidermis .
Higher Magnification of Clear Cell Poroma Higher magnification of a clear cell area of poroma shows a proliferation of small cells with abundant pale to clear-staining cytoplasm and small nuclei lacking atypia.
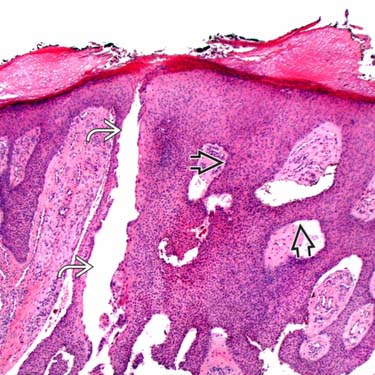
 between thickened cords of tumor cells and to epidermis. Note the ectatic ductal space on the left
between thickened cords of tumor cells and to epidermis. Note the ectatic ductal space on the left  .
.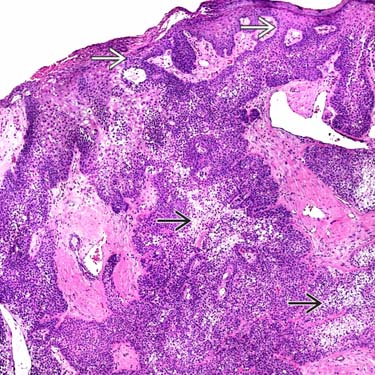
 neoplasm with multiple anastomosing connections between thickened cords of tumor cells and to epidermis
neoplasm with multiple anastomosing connections between thickened cords of tumor cells and to epidermis  .
.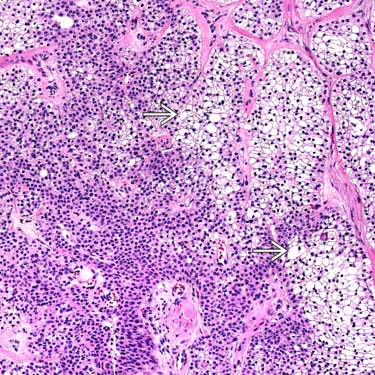
 and small nuclei lacking atypia.
and small nuclei lacking atypia.














