• Treatment: Wide surgical excision with negative margins
• Local recurrence in up to 40%
• Low metastatic potential (6%)
Macroscopic
• Multinodular, poorly delineated, tan-white
• Usually < 3 cm (range: 0.3-8.5 cm)
Microscopic
• Poorly circumscribed with infiltrative growth pattern
• Morphologically subdivided into 3 types (fibroblastic, histiocytic, mixed)
• Fascicles of spindled fibroblastic cells
• Nodules or aggregates of epithelioid histiocytoid cells
Osteoclast-like giant cells common
• Multinodular and plexiform growth
• Low mitotic rate; usually no cellular pleomorphism
Ancillary Tests
• (Myo)fibroblasts SMA(+); histiocytes CD68(+) and CD163(+)
• Negative for S100, CD34, desmin, keratin, MITF
Top Differential Diagnoses
• Cellular neurothekeoma
• Giant cell tumor of soft tissue
• Fibromatosis
• Low-grade myofibroblastic sarcoma
Plexiform Fibrohistiocytic Tumor Plexiform fibrohistiocytic tumor (PFHT) is an unusual, infiltrative mesenchymal neoplasm that typically arises near the dermal-subcutaneous junction, as depicted. Tumors are characterized by fascicles or sheets of spindled fibroblasts &/or nests of histiocytoid cells in a nodular and plexiform growth pattern.
Infiltrative Growth in Plexiform Fibrohistiocytic Tumor Most cases of PFHT are infiltrative and characteristically show extensions or projections of tumor into the subcutaneous adipose tissue.
Mixed-Type Plexiform Fibrohistiocytic Tumor The mixed subtype of PFHT shows a complex mixture of nests of histiocytoid cells with short fascicles of bland spindled cells .
Histiocytoid Nests in Plexiform Fibrohistiocytic Tumor The characteristic nests and aggregates of PFHT, when present, contain plump to epithelioid mononuclear histiocytoid cells. Multinucleated giant cells may or may not be present.
TERMINOLOGY
Abbreviations
• Plexiform fibrohistiocytic tumor (PFHT)
Synonyms
• Plexiform fibrous histiocytoma
Definitions
• Rarely metastasizing dermal-subcutaneous mesenchymal neoplasm composed of variable mixture of fibroblasts and histiocyte-like cells
CLINICAL ISSUES
Epidemiology
• Incidence
Rare
• Age
Most common in children and young adults
– Overall wide range: 1-77 years
• Sex
Male = female
– Female predilection in some series
Site
• Upper extremity (particularly forearm and hand)
• Also lower extremity, trunk, head and neck
• Most arise at dermal-subcutaneous interface
May also be purely dermal or subcutaneous
– Subcutaneous tumors may involve skeletal muscle
Presentation
• Painless, slow-growing mass or plaque
Treatment
• Wide surgical excision or reexcision with negative margins
• Examination of regional lymph nodes may be warranted
• Indefinite clinical follow-up recommended
Prognosis
• Local recurrence in up to 40%
• Low metastatic potential (6%)
Regional lymph nodes
Only gold members can continue reading. Log In or Register to continue

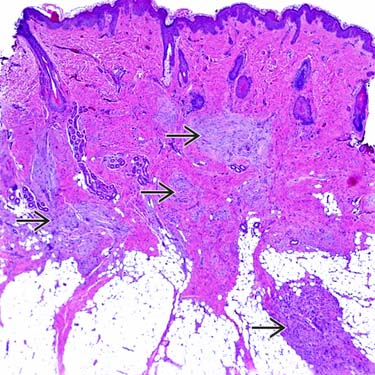
 that typically arises near the dermal-subcutaneous junction, as depicted. Tumors are characterized by fascicles or sheets of spindled fibroblasts &/or nests of histiocytoid cells in a nodular and plexiform growth pattern.
that typically arises near the dermal-subcutaneous junction, as depicted. Tumors are characterized by fascicles or sheets of spindled fibroblasts &/or nests of histiocytoid cells in a nodular and plexiform growth pattern.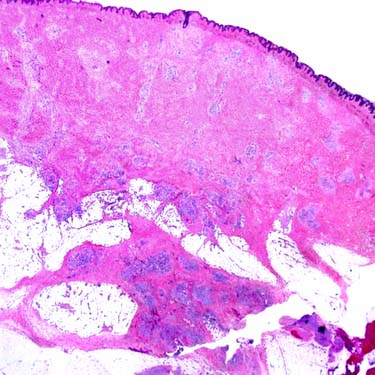
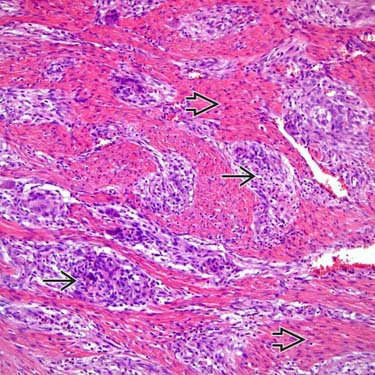
 of histiocytoid cells with short fascicles of bland spindled cells
of histiocytoid cells with short fascicles of bland spindled cells  .
.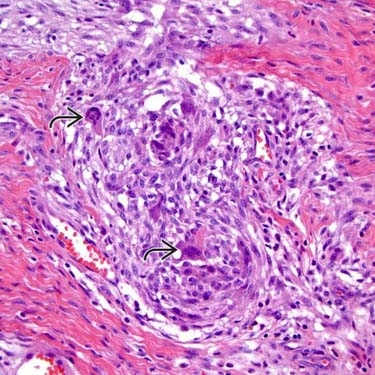
 may or may not be present.
may or may not be present.








