Plasmacytoma
Pei Lin, MD
Key Facts
Terminology
Plasmacytoma is a neoplasm composed of monoclonal plasma cells that involves tissues
No evidence of bone marrow involvement
No clinical or laboratory evidence of myeloma
2 general types of plasmacytoma
EP: Neoplasm composed of plasma cells, which arises in tissues other than bone
SPB: Localized (single) bone tumor composed of plasma cells
Clinical Issues
Small M-component in ˜ 50% of SPB, < 25% of EP
No anemia or elevated creatinine
Microscopic Pathology
Plasma cells show a spectrum of maturation
Ancillary Tests
CD138(+), CD38(+), MUM1/IRF-4(+), and cytoplasmic light chain restriction
Usually pax-5(−), CD20(−)
Top Differential Diagnoses
MALT lymphoma with marked plasmacytic differentiation
Castleman disease, plasma cell variant
Plasmablastic lymphoma
ALK(+) diffuse large B-cell lymphoma
Diagnostic Checklist
SPB has high risk of progression to myeloma; much less for EP
Persistent paraprotein signifies higher risk of progression
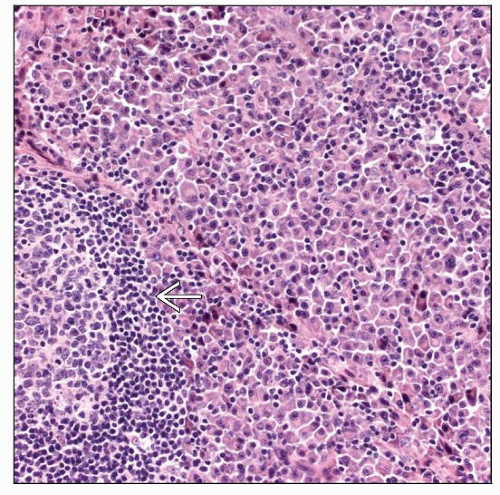 Plasmacytoma involving lymph node. The neoplasm has a parafollicular pattern and is composed of mature plasma cells. Note the presence of a lymphoid follicle with a hyperplastic germinal center  . . |
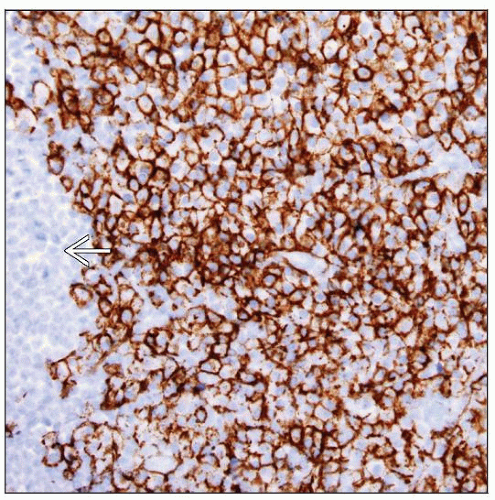 Plasmacytoma involving lymph node. The neoplasm is strongly CD138(+). A hyperplastic lymphoid follicle that is CD138(−) is at the left of the field  . . |
TERMINOLOGY
Abbreviations
Extramedullary plasmacytoma (EP)
Solitary plasmacytoma of bone (SPB)
Synonyms
Extraosseous or osseous plasmacytoma
Definitions
Neoplasm composed of monoclonal plasma cells that involves tissues
No evidence of bone marrow involvement
No clinical features of plasma cell myeloma
Small or absent M-component in urine or serum
ETIOLOGY/PATHOGENESIS
Immune Dysfunction
T- or B-cell deficiency or autoimmune disorders may play a role in some cases
CLINICAL ISSUES
Epidemiology
Incidence
Rare
< 5% of all plasma cell malignancies
SPB is more frequent than EP
Age
Median age ˜ 55 years
IgA(+) extramedullary plasmacytomas occur at a younger age
Gender
Male:female: ˜ 2-3:1
Presentation
Extramedullary plasmacytoma
Head and neck is most common site of disease (90%)
Upper respiratory tract: Nasopharynx, sinuses, and tonsils
˜ 4% of all nonepithelial tumors of this area
Nasal obstruction, epistaxis, mass
May spread to cervical lymph nodes in ˜ 15% of cases
Gastrointestinal (GI) tract is 2nd most common site
Other rare sites of disease
Lymph node, bladder, breast, thyroid, testis, brain, skin
Solitary plasmacytoma of bone
Bone pain, severe back pain, spinal cord compression, pathological fracture
Thoracic vertebrae are most common site of disease
Lumbar or cervical vertebrae are 2nd most common locations
Involvement of distal extremities, below knees or elbow, is rare
Laboratory Tests
Small M-component in up to 50% of SPB and in < 25% of EP cases
˜ 20% of EP cases have paraprotein of IgA type
Levels of uninvolved Ig are usually normal
No anemia or elevated creatinine
Serum free light chain ratio may be abnormal
Treatment
Radiation
Surgery
Prognosis
Prognosis of EP is significantly better than that of SPB
˜ 2/3 are alive for > 10 years
Only 15% of EP progress to plasma cell myeloma
Survival of SPB is better than that of myeloma patients
50% of SPB patients are alive at 10 years
25-40% are disease free at 10 years
50% of SPB progress to plasma cell myeloma
Progression usually occurs within 3-4 years of diagnosis; risk is higher in patients with
Large mass (> 5 cm)
Persistent M-protein
Rising free Ig light chain ratio
Recurrences are frequent in SPB and EP
IMAGE FINDINGS
General Features
Extramedullary plasmacytoma
No evidence of bone involvement
Solitary plasmacytoma of bone
Single lytic bone lesion
No additional lesions by MRI
MICROSCOPIC PATHOLOGY
Histologic Features
Diffuse infiltrate of plasma cells
EP of head and neck and GI tract more often show mature cytology
Plasma cells may show spectrum of maturation from well to poorly differentiated
Mature plasma cells
Round eccentric nuclei, clumped peripheral nuclear chromatin, and cytoplasmic perinuclear hof
Nucleoli absent or inconspicuous
Immature plasma cells
Pleomorphic nuclei, fine and immature nuclear chromatin
Prominent nucleoli
Plasmablastic or anaplastic morphology
Large nuclei with centrally located nucleoli (immunoblast-like)
Lymph Nodes
Plasma cells present in diffuse sheets
Partially involved cases have parafollicular or paracortical pattern
± residual lymphoid follicles
ANCILLARY TESTS
Immunohistochemistry
Plasmacytoma shows an immunophenotype similar to plasma cell myeloma
CD138(+), CD38(+), MUM1/IRF-4(+), and cytoplasmic light chain restricted
CD79a(+), usually IgG(+) or IgA(+)
CD56 is more frequently positive in SPB (˜ 50%) than in EP (˜ 10%)
Cyclin-D1(+) small subset
Some cases express Cyclin-D1 due to CCND1 gene amplification
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


