Pigmented Spindle Cell Nevus (Reed Nevus)
David Cassarino, MD, PhD
Key Facts
Terminology
Pigmented spindle cell nevus (PSCN)
Pigmented spindle cell nevus of Reed
Melanocytic proliferation that is typically predominantly junctional and composed of a population of spindle-shaped cells with heavy cytoplasmic pigmentation
Clinical Issues
Typically young adults (usually < 35 years old)
More common in females
Most often presents on extremities, especially leg
Microscopic Pathology
Compound, predominantly junctional (in most cases) melanocytic proliferation
Composed of spindle-shaped melanocytes with “streaming together” appearance
Pagetoid upward scatter may be seen
Dermis shows numerous melanophages in most cases
Cells are moderately enlarged, spindle-shaped melanocytes
Typically show hyperchromatic-staining nuclei with small nucleoli
Cytoplasm with prominent melanin pigmentation
Atypical Reed nevus
Often larger, more cellular lesions
Increased mitotic activity, especially in junctional component
Top Differential Diagnoses
Spitz nevus
Melanoma
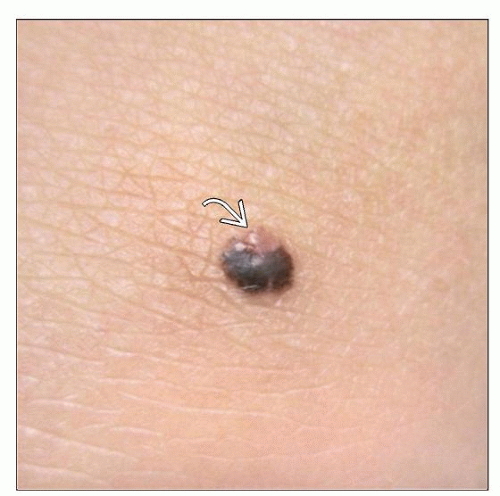 Clinical photograph shows a pigmented spindle cell nevus on the knee of a young adult patient. This case shows dark pigmentation, except 1 area at the top of the lesion with depigmentation  . (Courtesy P. Hsu, MD.) . (Courtesy P. Hsu, MD.) |
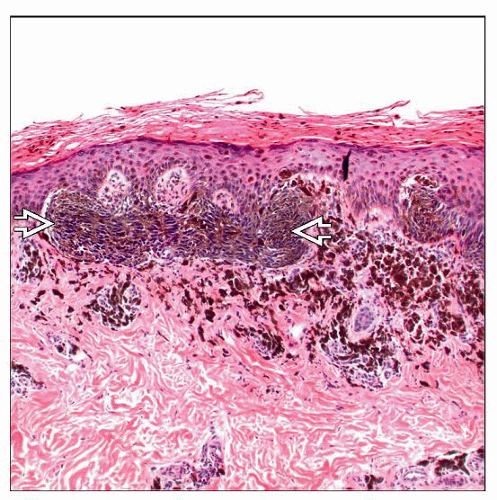 Histologic examination of a Reed nevus shows fusion of rete ridges by a proliferation of junctional pigmented spindle cells, which show a characteristic “streaming together”  pattern. pattern. |
TERMINOLOGY
Abbreviations
Pigmented spindle cell nevus (PSCN)
Synonyms
Pigmented spindle cell nevus of Reed
Definitions
Melanocytic proliferation that is typically predominantly junctional and composed of a population of spindle-shaped cells with heavy cytoplasmic melanin pigmentation
Controversial, but often considered a variant of Spitz nevus, which occurs more frequently in adults
ETIOLOGY/PATHOGENESIS
Unknown
May be related to solar exposure in some cases
CLINICAL ISSUES
Epidemiology
Incidence
Relatively uncommon tumors
Age
Typically young adults (usually < 35 years old)
Gender
More common in females
Ethnicity
Caucasian patients in most cases
Site
Most often presents on extremities, especially leg
Classic presentation is on thigh of a young woman
Presentation
Pigmented lesion
Usually papular, but can be nodular
Treatment
Surgical approaches
Complete excision is curative
Typically recommended in partially sampled lesions
To allow for complete evaluation to exclude more atypical areas
To prevent recurrence
Prognosis
Excellent; may recur if incompletely excised, but very low risk of developing melanoma
MACROSCOPIC FEATURES
Size
Usually small (< 1 cm)
MICROSCOPIC PATHOLOGY
Histologic Features
Compound, predominantly junctional (in most cases) melanocytic proliferation
Symmetric, well-circumscribed lesion
Junctional nests often large and show bridging across several rete ridges
Composed of spindle-shaped melanocytes with “streaming together” appearance
Overlapping features with junctional Spitz nevi, but conventional Spitz nevi not as heavily pigmented
Pagetoid upward scatter may be seen, similar to Spitz nevi
Dermal component is usually small and superficial and composed of a few single cells &/or small nests in papillary dermis
Overlying hyperkeratosis and pigmented parakeratosis are usually present
Often associated with dermal inflammation
Dermis shows numerous melanophages in most cases
Atypical Reed nevus
Pigmented spindle cell nevus with atypical features
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


