The periosteum is the layer of tissue that envelopes the outer surface of bone, demarcating bone from soft tissue.
It is a complex structure that provides a niche for pluripotent cells, and is a repository for tissue molecular factors that can modulate the local cellular environment (1).
The periosteum covers the majority of bony structures, with the exception of sesamoid bones and the intra-articular portion of bone (2). A curious and important exception to the lack of periosteum in the intra-articular ends of bones is the hip, where the periosteum is continuous with the hip’s fibrous capsule and reflects backward, an anatomical feature which helps to explain mineralizing tissue sometimes observed at that site.
It is a bilayered membrane consisting of an outer fibrous layer and an inner “cambium” layer. The outer layer consists mostly of collagens and elastin and serves mostly a mechanical or structural role (2). The innermost layer, closest to the bone, is a cellular layer rich in progenitor cells that build and repair bone throughout life. It is well known that periosteal stripping decreases cortical bone perfusion and impairs fracture healing (3). Although the periosteum is now well recognized as a source of pluripotent cells, studies with periosteal grafts have shown variation in osteogenic potential with calvarial periosteum less osteogenic than that of the tibia (4). Attempts to exploit the osteogenic potential of the periosteum have included imaginative approaches such as extracorporeal shock wave treatment (5).
The outer fibrous layer can be subdivided into a superficial portion, which is the most vascularized substratum of the periosteum and a significant contributor to the blood supply of bone and even muscle. This layer is rich in neural tissue, which penetrates to the bone surface. The deeper portion of the outer fibrous layer is rich in elastin fibers, which provide elasticity.
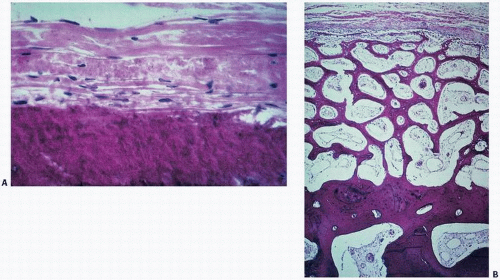
The inner cambium layer, named by Duhamel in 1739 for its resemblance to the ring pattern seen in cut logs, is thickest in the fetus and then thins with aging. It is rich in mesenchymal progenitor cells, differentiated osteogenic progenitor cells, osteoblasts, and fibroblasts (2). Osteoblasts are in contact with the bone (Fig. 7.1).
Osteoclasts in the periosteum most likely originate by migration from the marrow through cortical bone.
Only bones with periosteum can demonstrate a periosteal reaction, and thus, periosteal reactions are not noted in the carpal and tarsal bones. Because the periosteum usually ends at the perichondral ring from which it originally arises, periosteal reactions typically fall several millimeters short of the growth plate. Causes of periosteal reaction include trauma, tumor, infection, and infarction. A periosteal reaction in the first 6 months of life has been considered physiologically normal.
Periosteum, especially in the growing skeleton, has enormous bone-forming potential. In children, periosteum is a complex, thick layer loosely attached to cortical bone and thus more easily biologically active. In adults, it is thinner and more tightly adherent to bone. Periosteal new bone formation is most evident in childhood following fracture or infection. In fact, periostitis characterizes infection in congenital syphilis. In the growing skeleton, the metabolic activity of the periosteum appears more obvious than in adults, where it appears inactive in the absence of trauma or other stimuli. Nonetheless, certain conditions are associated with, if not characterized by, periosteal reactions. Hypertrophic pulmonary osteoarthropathy (HPOA) is a syndrome with periosteal new bone formation in association with pulmonary disease and pulmonary tumors and has been described in association with liver pathology as well. The etiology is poorly understood. Conversely, in Camurati-Engelmann disease, the endocortical surface seems primarily affected. In addition to bone-forming potential, the periosteum has been shown in vitro and in vivo to have a chondrogenic potential that permits its use for cartilage regeneration (6). In rabbits, chondrogenic potential of the periosteum varies from best at the ilium, followed by the scapula and tibia (1). Interestingly, within the tibia, the upper tibia was more chondrogenic than the lower tibia. Chondrogenic potential of the periosteum was related to cellularity of the cambium layer.
In metabolic bone disease, the periosteal envelope is of import. Both hyperparathyroidism and bone aging have been characterized by thinning and widening, which has been measured in the skull, femur, metacarpal, and other bones (7) and may be the result of the lifelong periosteal bone apposition being slower than endosteal (endocortical) bone turnover, including a prevailing osteoclast bone resorption. Periosteal bone formation appears to follow the well-established coupling mechanisms of bone remodeling with osteoclast resorption linked to formation. However, this occurs slower than the rest of bone (with a net increase) and is probably discontinuous with long periods of interruption (7). It appears less affected by biomechanical (modeling) factors. Although periosteal remodeling appears qualitatively similar to remodeling in cortical, endocortical, and trabecular bone, it appears to be quantitatively different (7).
FIGURE 7.1. (A) Normal periosteum and (B) periosteal new bone formation. The normal periosteum consists of an outer sparsely cellular fibrous layer and a more cellular inner cambium layer, from which arise bone-forming cells, as evidenced in the marked new bone formed in (B).
In reviewing periosteal lesions, Kenan et al. (8) have differentiated surface bone activity into three compartments: (a) juxtacortical, a broad term for lesions arising outside the cortical bone; (b) cortical, lesions of cortical bone that extend into the adjacent periosteum and soft tissue; and (c) truly periosteal lesions.
They further subdivided periosteal lesions into those confined to the subperiosteum, the potential zone between bone and periosteum, as seen involved in infection and subperiosteal hemorrhage, and intraperiosteal lesions. Intraperiosteal lesions are usually tumors expressing the pluripotentiality of the periosteum. A modified classification of surface periosteal lesions is presented in Table 7.1 (8,9), many of which arise in or significantly involve the periosteum.
Hypertrophic (Pulmonary) Osteoarthropathy
In 1889, Bamberger described a syndrome, later reported by Marie, characterized by clubbing of the fingers with associated bone and joint changes (Fig. 7.2). This condition has come to be known as HPOA, and it refers to a clinical syndrome that includes clubbing of the fingers and toes; periostitis of the tubular bones of the extremities, especially distal to the elbows and knees; and arthritis. Although originally described in association with pulmonary lesions, the Marie-Bamberger syndrome has been seen in a wide range of disorders (10) (Table 7.2). Its most common setting is that of pulmonary tumors, where it is seen in approximately 10 percent of cases, but it has been increasingly recognized as a complication of other pulmonary disorders (5), including infections and bronchiectasis, cyanotic congenital heart disease, gastrointestinal problems such as ulcerative colitis, liver disease (11), and even tumors of the gastrointestinal and lymph systems. Hereditary forms have been described. In the primary form, the condition may appear after puberty. Hereditary forms appear to have a dominant trait with incomplete penetrance.
The clinical picture is either that of a symptomless individual or that of one who may be experiencing arthralgias, arthritis, or even bone pain. In HPOA, there may be thickening of the skin with deepened creases, often with pronounced facial prominence, suggesting acromegaly.
The pathologic changes usually develop at the distal ends of the metacarpal, metatarsal, and long bones of the forearms and legs. Common sites are the distal tibia, fibula, radius, and ulna. In advanced cases, dramatic changes of the metacarpal and metatarsal bones may be seen. The axial bones and skull are usually spared. Other involved bones in severe cases may be the ribs, clavicles, scapula, and pelvis.
The clinical manifestation may mimic rheumatoid arthritis, and both morning stiffness and increased sedimentation rates have been described.
Histopathologically, the early changes are that of edema and sparse mononuclear cell infiltration in the periosteum, synovium, and associated para-articular tissues. Eventually, the periosteum forms osteoid, which, with subsequent mineralization, gives rise to the classic x-ray picture of periosteal new bone formation (Fig. 7.3). It is thought that this intramembranous periosteal new bone formation is at the expense of accelerated endosteal resorption, leading to a thin and weakened bone. Synovial biopsies may also show nonspecific changes, including edema and mononuclear cell infiltration. The changes appreciated histopathologically are often mild and nonspecific.
TABLE 7.1 Classification of Lesions Arising from and/or Involving Periosteum
1. Tumor-like conditions
Periosteal reaction in metabolic/hormonal/systemic disorders (e.g., hypertrophic pulmonary osteoarthropathy)
Posttraumatic reparative processes
Subperiosteal hematoma
Florid reactive periostitis
Periostitis ossificans
Myositis ossificans
Osteochondromatous proliferation Subungual
Bizarre parosteal (Nora lesion)
Stress fractures
Infant periostitis
Periosteal amyloid
2. True neoplasms
Bone-forming
Periosteal osteoid osteoma/osteoblastoma
Parosteal osteoma
Parosteal osteosarcoma
Periosteal osteosarcoma
High-grade surface osteosarcoma
Dedifferentiated parosteal osteosarcoma
Cartilage
Osteochondroma
Periosteal chondroma
Periosteal chondromyxoid fibroma
Periosteal fibromyoma
Periosteal chondrosarcoma
Subperiosteal mesenchymal chondrosarcoma
Fibrous
Cortical irregularity syndrome
Periosteal fibromatosis
Periosteal fibrosarcoma
Periosteal malignant fibrous histiocytoma
Round cell
Periosteal Ewing sarcoma
Vascular
Periosteal hemangioma
Neurogenic
Periosteal neurofibromatosis
3. Miscellaneous
Periosteal leiomyoma
Parosteal lipoma
Periosteal ganglion
Juxtacortical adamantinoma
Periosteal myxoma
Periosteal giant-cell tumor
Periosteal giant-cell reparative granuloma
Modified after Kenan S, Abdelwahab IF, Klein MJ, et al. Lesions of juxtacortical origin (surface lesions of bone) [Review]. Skeletal Radiol. 1993;22:337-357; Sugiura I. Tibial periosteal hemangioma. Clin Orthop. 1975;106:242-244.
The x-rays are characteristic, with symmetric periostitis along the shafts of the bone, often confined to the diaphysis, but progressing proximally. They characteristically do not involve the joint. Bone scans characteristically show diffuse increased uptake along the periosteum or cortical margins of long bones, giving a parallel or double-stripe sign with sparing of the epiphysis (12). There may be, on routine roentgenographic studies, an opaque line of new bone separated from the underlying dense cortex by a narrow radiolucent band, or indeed an onion skinning effect suggestive of a small-cell tumor. Actual ossification at the insertion of ligaments and tendons as seen in fluoride osteopathy may be noted.
The periostitis has been described as regular and undulating in HPOA, and shaggy and florid in a rare primary type called pachydermoperiostosis, an autosomal dominant disease characterized by pachydermia, periostitis, and cutis verticis gyrata (12).
The laboratory is routinely normal in hypertrophic osteoarthropathy, although cases with elevated alkaline phosphatase have been noted, suggesting a role for osteoblast activity.
Etiologic considerations have included vascular, hormonal, and neurogenic etiology. Support for a vascular abnormality has been suggested based on the occasional relief noted after vagotomy (10). In one study of hypertrophic hepatic osteoarthropathy, the presence of mild arterial hypoxemia, increased cardiac output, and evidence of right to left shunting further suggested a vascular etiology. However, these changes were not statistically significant from those of controls. Hormonal etiologies are suggested, based in part on the acromegaly-like clinical symptoms and facial appearances seen in some patients. However, hormonal or hormonal-like substances related to the more well-defined syndromes of acromegaly have not yet been discerned in this condition. In fact, hormonal-like substances capable of stimulating periosteal new growth have been suggested to be inactivated in the pulmonary circulation, a mechanism bypassed in disorders creating right to left shunting. In this regard, the rarity of the condition in cyanotic congenital heart disease is of note.
The neurogenic theory has been based on anatomical study, suggesting that hepatic branches of the vagus nerve may carry afferent impulses to the central nervous system that subsequently may mediate the vascular changes noted in hypertrophic osteoarthropathy (11).
There has been evidence of hypertrophic osteoarthropathy in human skeletal remains as early as the pre-Hispanic Mesoamerica period (13). Martinez-Lavin et al. (13) have estimated, through preserved Mexican bones of this period, that the bone changes of HPOA were present in Mexico near the time of the original description of clubbing by Hippocrates (approximately 2,500 years ago).
Periostitis
The differential diagnosis of inflammation of the periosteum, “periostitis,” is large and includes infection, arthritides, trauma, metabolic and congenital causes, and vascular and genetic causes. Drug-related periostitis is seen in fluorosis, hypervitaminosis A, prostaglandins, retinoids, and the antifungal agent voriconazole (14).
The differential diagnosis of periostitis in infancy is broad (15). Periostitis in congenital syphilis is diffuse, symmetric, and usually identified in the first few months of life. Associated osteomyelitis destroys the bones, especially the long tubular bones. Excess vitamin A or insufficient vitamin C (scurvy) results in periosteal reactions. In hypervitaminosis A, there is extensive diaphyseal involvement (see Fig. 4.63). Usually seen after 1 year of age, the ulna, clavicle, and metatarsal bones are primarily involved. Hard tender forearm nodules are common. Scurvy is characterized by subperiosteal hemorrhage (see Fig. 4.62). Metaphyses are primarily involved, often with irregular enlarged zones of provisional calcification. Metaphyseal defects, including transverse metaphyseal lucencies, are characteristic. Most cases are diagnosed between 8 and 14 months with evidence of bleeding in mucosal surfaces, skin, urine, or bowel. Tender soft tissue masses, fever, and irritability in association with diaphyseal periostitis of the mandible, ulnae, ribs, and clavicles in a symmetric fashion characterize Caffey disease (infantile cortical hyperostosis). Other periostitis syndromes of infancy include osseous changes of leukemia, trauma, including battered child syndrome, osteomyelitis, and hypertrophic osteoarthropathy associated with cyanotic congenital heart disease.
Only gold members can continue reading. Log In or Register to continue