Patient Story
A young man presented with painful blisters on his face and mouth (Figure 185-1). The patient was referred to dermatology that day. The dermatologist recognized likely pemphigus vulgaris (PV) and did shave biopsies for histopathology and direct immunofluorescence of facial vesicles/bullae to confirm the presumed diagnosis. The patient was started on 60 mg of prednisone daily until the pathology confirmed PV. Steroid-sparing therapy was then discussed and started in 2 weeks from presentation.

Introduction
Pemphigus is a rare group of autoimmune bullous diseases of skin and mucous membranes characterized by flaccid bulla and erosions. The three main types of pemphigus are PV (with the pemphigus vegetans variant), pemphigus foliaceous (with the pemphigus erythematosus variant), and paraneoplastic pemphigus. All types of pemphigus cause significant morbidity and mortality. Although pemphigus is not curable, it can be controlled with systemic steroids and immunosuppressive medications. These medications can be lifesaving, but also place pemphigus patients at risk for a number of complications. The word pemphigus is derived from the Greek word pemphix, which means bubble or blister.
Epidemiology
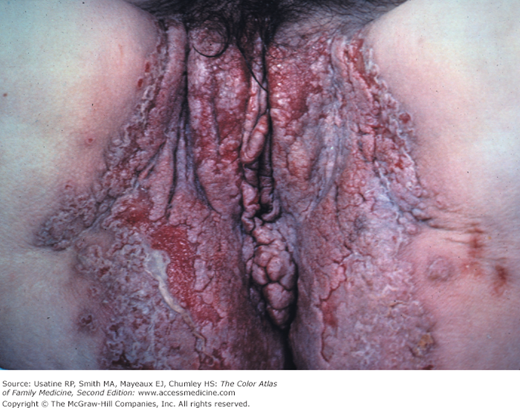
- PV (Figures 185-1, 185-2, 185-3, and 185-4):
- Most common form of pemphigus in the United States.
- Annual incidence is 0.75 to 5 cases per 1 million population.1
- Usually occurs between 30 and 50 years of age.2
- Increased incidence in Ashkenazi Jews and persons of Mediterranean origin.2
- Pemphigus vegetans is a variant form of PV (Figures 185-5 and 185-6).
- Most common form of pemphigus in the United States.
- Pemphigus foliaceus (PF) (Figures 185-7, 185-8, 185-9, and 185-10): Superficial form of pemphigus.
- More prevalent in Africa (Figures 185-11 and 185-12).1
- Variant forms include pemphigus erythematosus (resembles the malar rash of lupus erythematosus) and fogo selvagem.
- Fogo selvagem is an endemic form of PF seen in Brazil and affects teenagers and individuals in their twenties.1
- More prevalent in Africa (Figures 185-11 and 185-12).1
- Paraneoplastic pemphigus (PNP)
- Onset at age 60 years and older.
- Associated with occult neoplasms commonly lymphoreticular.
- Malignancies like non-Hodgkin lymphoma and chronic lymphocytic leukemia.
- Also associated with benign neoplasms such as thymoma and Castleman disease (angiofollicular lymph node hyperplasia).2
- Onset at age 60 years and older.










Etiology and Pathophysiology
- The basic abnormality in all three types of pemphigus is acantholysis, a process of separating keratinocytes from one another. This occurs as a result of autoantibody formation against desmoglein (the adhesive molecule that holds epidermal cells together). Separation of epidermal cells leads to formation of intraepidermal clefts, which enlarge to form bullae.1
- The mechanism that induces the production of these autoantibodies in most individuals is unknown. Yet PF may be triggered by drugs, most commonly thiol compounds like penicillamine, captopril, piroxicam, and others, like penicillin and imiquimod.3 An environmental trigger in the presence of susceptible human leukocyte antigen (HLA) gene is suggested to induce autoantibodies in fogo selvagum.1
- The autoantibodies in pemphigus are usually directed against desmoglein 1 and 3 molecules (Dsg1 and Dsg3). Dsg1 is present predominantly in the superficial layers of the epidermis, whereas Dsg3 is expressed in deeper epidermal layers and in mucous membranes. As a result, clinical presentation depends on the antibody profile. In PV, a limited mucosal disease occurs when only anti-Dsg3 antibody is present, but extensive mucosal and cutaneous disease occurs when both anti-Dsg1 and Dsg3 antibodies are present. In PF, mucosal lesions are absent and the cutaneous lesions are superficial because of isolated anti-Dsg1 antibody.
- Patients with PNP demonstrate both anti-Dsg1 and Dsg3 antibodies. However, unlike PV, autoantibodies against plakin proteins (another adhesive molecule) are also observed in patients with PNP and these autoantibodies form a reliable marker for this type of pemphigus.
Diagnosis
- Pemphigus vulgaris (Figures 185-1, 185-2, 185-3, and 185-4)—Classical lesions are flaccid bullae that rupture easily, creating erosions. Since bullae are short-lived, erosions are the more common presenting physical finding (Figure 185-13). Lesions are typically tender and heal with postinflammatory hyperpigmentation that resolves without scarring. A positive Asboe-Hansen or Nikolsky sign may be present, but neither sign is diagnostic. A positive Asboe-Hansen sign occurs when a bulla extends to surrounding skin while pressure is applied directly to the bulla. The Nikolsky sign is positive when skin shears off while lateral pressure is applied to unblistered skin during active disease. Sometimes the Asboe-Hansen sign is also attributed to Nikolsky and called a Nikolsky sign, too.
- Pemphigus vegetans is a variant of PV where healing is associated with vegetating proliferation of the epidermis (Figures 185-5 and 185-6

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


