

INTRODUCTION TO PELVIS AND PERINEUM
PELVIC GIRDLE
Bones and Features of Pelvic Girdle
Orientation of Pelvic Girdle
Joints and Ligaments of Pelvic Girdle
TABLE 3.1. Comparison of Male and Female Bony Pelves
BLUE BOX: Pelvic Girdle. Variations in Male and Female Pelves; Pelvic Diameters (Conjugates); Pelvic Fractures; Relaxation of Pelvic Ligaments and Increased Joint Mobility in Late Pregnancy; Spondylolysis and Spondylolisthesis
PELVIC CAVITY
Walls and Floor of Pelvic Cavity
TABLE 3.2. Muscles of Pelvic Walls and Floor
Peritoneum and Peritoneal Cavity of Pelvis
TABLE 3.3. Peritoneal Reflections in Pelvis
Pelvic Fascia
BLUE BOX: Pelvic Cavity. Injury to Pelvic Floor; Prenatal “Relaxation” Training for Participatory Childbirth
NEUROVASCULAR STRUCTURES OF PELVIS
Pelvic Arteries
TABLE 3.4. Arteries of Pelvis
Pelvic Veins
Lymph Nodes of Pelvis
Pelvic Nerves
TABLE 3.5. Somatic Nerves of Pelvis
BLUE BOX: Neurovascular Structures of Pelvis. Iatrogenic Injury of Ureters; Injury During Ligation of Uterine Artery; Injury During Ligation of Ovarian Artery; Ligation of Internal Iliac Artery and Collateral Circulation in Pelvis; Injury to Pelvic Nerves
PELVIC VISCERA
Urinary Organs
Rectum
TABLE 3.6. Parts of Male Urethra
BLUE BOX: Urinary Organs and Rectum. Iatrogenic Compromise of Ureteric Blood Supply; Ureteric Calculi; Cystocele—Hernia of Bladder; Suprapubic Cystotomy; Rupture of Bladder; Cystoscopy; Clinically Significant Differences Between Male and Female Urethrae; Rectal Examination; Resection of Rectum
Male Internal Genital Organs
BLUE BOX: Male Internal Genital Organs. Male Sterilization; Abscesses in Seminal Glands; Hypertrophy of Prostate
Female Internal Genital Organs
BLUE BOX: Female Internal Genital Organs. Infections of Female Genital Tract; Patency of Uterine Tubes; Hysterosalpingography; Endoscopy; Ligation of Uterine Tubes; Ectopic Tubal Pregnancy; Remnants of Embryonic Ducts; Bicornate Uterus; Disposition of Uterus and Uterine Prolapse; Manual Examination of Uterus; Lifetime Changes in Anatomy of Uterus; Cervical Cancer, Cervical Examination and Pap Smear; Hysterectomy; Distension of Vagina; Digital Pelvic Examination; Vaginal Fistulae; Culdoscopy and Culdocentesis; Laparoscopic Examination of Pelvic Viscera; Anesthesia for Childbirth
Lymphatic Drainage of Pelvic Viscera
TABLE 3.7. Lymphatic Drainage of Structures of Pelvis and Perineum
PERINEUM
Fasciae and Pouches of Urogenital Triangle
Features of Anal Triangle
TABLE 3.8. Arteries of Perineum
BLUE BOX: Perineum. Disruption of Perineal Body; Episiotomy; Rupture of Urethra in Males and Extravasation of Urine; Starvation and Rectal Prolapse; Pectinate Line—A Clinically Important Landmark; Anal Fissures and Perianal Abscesses; Hemorrhoids; Anorectal Incontinence
Male Urogenital Triangle
TABLE 3.9. Muscles of Perineum
BLUE BOX: Male Urogenital Triangle. Urethral Catheterization; Distension of Scrotum; Palpation of Testes; Hypospadias; Phimosis, Paraphimosis, and Circumcision; Impotence and Erectile Dysfunction
Female Urogenital Triangle
TABLE 3.10. Nerves of Perineum
BLUE BOX: Female Urogenital Triangle. Female Circumcision; Vulvar Trauma; Infection of Greater Vestibular Glands; Pudendal and Ilio-inguinal Nerve Blocks; Exercises for Increased Development of Female Perineal Muscles; Vaginismus
SECTIONAL MEDICAL IMAGING OF PELVIS AND PERINEUM
Magnetic Resonance Imaging
INTRODUCTION TO PELVIS AND PERINEUM
In common usage, the pelvis (L. basin) is the part of the trunk that is inferoposterior to the abdomen, and is the area of transition between the trunk and the lower limbs. The pelvic cavity is the inferiormost part of the abdominopelvic cavity. Anatomically, the pelvis is the part of the body surrounded by the pelvic girdle (bony pelvis), part of the appendicular skeleton of the lower limb (Fig. 3.1).

FIGURE 3.1. Pelvis and perineum. A and B. The pelvis (green) is the space within the pelvic girdle, overlapped externally by the abdominal and gluteal regions, perineum, and lower back. Thus the pelvis has no external surface area. The greater pelvis (light green) is pelvic by virtue of its bony boundaries, but is abdominal in terms of its contents. The lesser pelvis (dark green) provides the bony framework (skeleton) for the pelvic cavity and deep perineum.
The pelvis is subdivided into greater and lesser pelves. The greater pelvis is surrounded by the superior pelvic girdle. The greater pelvis is occupied by inferior abdominal viscera, affording them protection similar to the way the superior abdominal viscera are protected by the inferior thoracic cage. The lesser pelvis is surrounded by the inferior pelvic girdle, which provides the skeletal framework for both the pelvic cavity and the perineum—compartments of the trunk separated by the musculofascial pelvic diaphragm. Externally, the pelvis is covered or overlapped by the inferior anterolateral abdominal wall anteriorly, the gluteal region of the lower limb posterolaterally, and the perineum inferiorly.
The term perineum1 refers both to the area of the surface of the trunk between the thighs and the buttocks, extending from the coccyx to the pubis, and to the shallow compartment lying deep (superior) to this area but inferior to the pelvic diaphragm. The perineum includes the anus and external genitalia: the penis and scrotum of the male and the vulva of the female.
PELVIC GIRDLE
The pelvic girdle is a basin-shaped ring of bones that connects the vertebral column to the two femurs. The primary functions of the pelvic girdle are to:
• Bear the weight of the upper body when sitting and standing.
• Transfer that weight from the axial to the lower appendicular skeleton for standing and walking.
• Provide attachment for the powerful muscles of locomotion and posture and those of the abdominal wall, withstanding the forces generated by their actions.
Consequently, the pelvic girdle is strong and rigid, especially compared to the pectoral (shoulder) girdle. Other functions of the pelvic girdle are to:
• Contain and protect the pelvic viscera (inferior parts of the urinary tracts and the internal reproductive organs) and the inferior abdominal viscera (intestines), while permitting passage of their terminal parts (and, in females, a full-term fetus) via the perineum.
• Provide support for the abdominopelvic viscera and gravid (pregnant) uterus.
• Provide attachment for the erectile bodies of the external genitalia.
• Provide attachment for the muscles and membranes that assist the functions listed above by forming the pelvic floor and filling gaps that exist in or around it.
Bones and Features of Pelvic Girdle
In the mature individual, the pelvic girdle is formed by three bones (Fig. 3.2A):
• Right and left hip bones (coxal or pelvic bones): large, irregularly shaped bones, each of which develops from the fusion of three bones, the ilium, ischium, and pubis.
• Sacrum: formed by the fusion of five, originally separate, sacral vertebrae.

FIGURE 3.2. Pelvic girdle. A and B. Features of the pelvic girdle demonstrated anatomically (A) and radiographically (B). The pelvic girdle is formed by the two hip bones (of the inferior axial skeleton) anteriorly and laterally and the sacrum (of the axial skeleton) posteriorly. C. The hip bone is in the anatomical position when the anterior superior iliac spine (ASIS) and the anterior aspect of the pubis lie in the same vertical plane. The preadolescent hip bone is composed of three bones—ilium, ischium, and pubis—that meet in the cup-shaped acetabulum. Prior to their fusion, the bones are united by a triradiate cartilage along a Y-shaped line (blue). D. An adult’s right hip bone in the anatomical position shows the bones when fused. (B courtesy of Dr. E. L. Lansdown, Professor of Medical Imaging, University of Toronto, Toronto, ON, Canada.)
The internal (medial or pelvic) aspects of the hip bones bound the pelvis, forming its lateral walls; these aspects of the bones are emphasized here. Their external aspects, primarily involved in providing attachment for the lower limb muscles, are discussed in Chapter 5. As they are part of the vertebral column, the sacrum and coccyx are discussed in detail in Chapter 4.
In infants and children, the hip bones consist of three separate bones that are united by a triradiate cartilage at the acetabulum (Fig. 3.2B), the cup-like depression in the lateral surface of the hip bone, which articulates with the head of the femur. After puberty, the ilium, ischium, and pubis fuse to form the hip bone. The two hip bones are joined anteriorly at the pubic symphysis, a secondary cartilaginous joint. The hip bones articulate posteriorly with the sacrum at the sacro-iliac joints to form the pelvic girdle.
The ilium is the superior, fan-shaped part of the hip bone (Fig. 3.2B & C). The ala (wing) of the ilium represents the spread of the fan, and the body of the ilium, the handle of the fan. On its external aspect, the body participates in formation of the acetabulum. The iliac crest, the rim of the fan, has a curve that follows the contour of the ala between the anterior and posterior superior iliac spines. The anteromedial concave surface of the ala forms the iliac fossa. Posteriorly, the sacropelvic surface of the ilium features an auricular surface and an iliac tuberosity, for synovial and syndesmotic articulation with the sacrum, respectively.
The ischium has a body and ramus (L. branch). The body of the ischium helps form the acetabulum and the ramus of the ischium forms part of the obturator foramen. The large postero-inferior protuberance of the ischium is the ischial tuberosity. The small pointed posteromedial projection near the junction of the ramus and body is the ischial spine. The concavity between the ischial spine and the ischial tuberosity is the lesser sciatic notch. The larger concavity, the greater sciatic notch, is superior to the ischial spine and is formed in part by the ilium.
The pubis is an angulated bone with a superior ramus, which helps form the acetabulum, and an inferior ramus, which helps form the obturator foramen. A thickening on the anterior part of the body of the pubis is the pubic crest, which ends laterally as a prominent swelling, the pubic tubercle. The lateral part of the superior pubic ramus has an oblique ridge, the pecten pubis (pectineal line of pubis).
The pelvis is divided into greater (false) and lesser (true) pelves by the oblique plane of the pelvic inlet (superior pelvic aperture) (Figs. 3.1A and 3.2A). The bony edge (rim) surrounding and defining the pelvic inlet is the pelvic brim, formed by the:
• Promontory and ala of the sacrum (superior surface of its lateral part, adjacent to the body of the sacrum).
• A right and left linea terminalis (terminal line) together form a continuous oblique ridge consisting of the:
• Arcuate line on the inner surface of the ilium.
• Pecten pubis (pectineal line) and pubic crest, forming the superior border of the superior ramus and body of the pubis.
The pubic arch is formed by the ischiopubic rami (conjoined inferior rami of the pubis and ischium) of the two sides (Fig. 3.2A & C). These rami meet at the pubic symphysis, their inferior borders defining the subpubic angle (Fig. 3.3). The width of the subpubic angle is determined by the distance between the right and the left ischial tuberosities, which can be measured with the gloved fingers in the vagina during a pelvic examination.
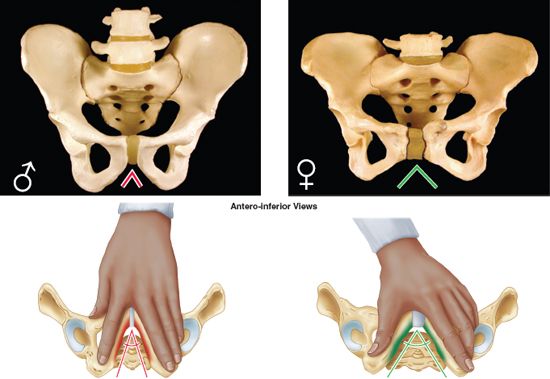
FIGURE 3.3. Pelvic girdles of male and female. Pubic arches, or subpubic angles typical for each gender (male = red; female = green) can be approximated by spreading index and middle finger (demonstrating narrow subpubic angle of male pelvis) or thumb and index finger (demonstrating wider subpubic angle of female pelvis).
The pelvic outlet (inferior pelvic aperture) is bounded by the (Figs. 3.1A and 3.2A):
• Pubic arch anteriorly.
• Ischial tuberosities laterally.
• Inferior margin of the sacrotuberous ligament (running between the coccyx and the ischial tuberosity) posterolaterally.
• Tip of the coccyx posteriorly.
The greater pelvis (false pelvis) is the part of the pelvis (Fig. 3.1):
• Superior to the pelvic inlet.
• Bounded by the iliac alae posterolaterally and the anterosuperior aspect of the S1 vertebra posteriorly.
• Occupied by abdominal viscera (e.g., the ileum and sigmoid colon).
The lesser pelvis (true pelvis) is the part of the pelvis:
• Between the pelvic inlet and the pelvic outlet.
• Bounded by the pelvic surfaces of the hip bones, sacrum, and coccyx.
• That includes the true pelvic cavity and the deep parts of the perineum (perineal compartment), specifically the ischio-anal fossae (Fig. 3.1B).
• That is of major obstetrical and gynecological significance.
The concave superior surface of the musculofascial pelvic diaphragm forms the floor of the true pelvic cavity, which is thus deepest centrally. The convex inferior surface of the pelvic diaphragm forms the roof of the perineum, which is therefore shallow centrally and deep peripherally. Its lateral parts (ischio-anal fossae) extending well up into the lesser pelvis. The terms pelvis, lesser pelvis, and pelvic cavity are commonly used incorrectly, as if they were synonymous terms.
Orientation of Pelvic Girdle
When a person is in the anatomical position, the right and left anterior superior iliac spines (ASISs) and the anterior aspect of the pubic symphysis lie in the same vertical plane (Fig. 3.2B & C). When a pelvic girdle in this position is viewed anteriorly (Fig. 3.2A), the tip of the coccyx appears close to the center of the pelvic inlet, and the pubic bones and pubic symphysis constitute more of a weight-bearing floor than an anterior wall. In the median view (Fig. 3.1A), the sacral promontory is located directly superior to the center of the pelvic outlet (site of the perineal body). Consequently, the curved axis of the pelvis intersects the axis of the abdominal cavity at an oblique angle.
The pelvic girdles of males and females differ in several respects (Fig. 3.3; Table 3.1). These sexual differences are related mainly to the heavier build and larger muscles of most men and to the adaptation of the pelvis (particularly the lesser pelvis) in women for parturition (childbearing). See the blue box “Variations in Male and Female Pelves,” on p. 334.
TABLE 3.1. COMPARISON OF MALE AND FEMALE BONY PELVES

Joints and Ligaments of Pelvic Girdle
The primary joints of the pelvic girdle are the sacro-iliac joints and the pubic symphysis (Fig. 3.4A). The sacro-iliac joints link the axial skeleton (skeleton of the trunk, composed of the vertebral column at this level) and the inferior appendicular skeleton (skeleton of the lower limb). The lumbosacral and sacrococcygeal joints, although joints of the axial skeleton, are directly related to the pelvic girdle. Strong ligaments support and strengthen these joints.

FIGURE 3.4. Joints of pelvic girdle. A. The sacro-iliac joints unite the axial and inferior appendicular skeletons. The lumbosacral and sacrococcygeal joints are joints of the axial skeleton directly related to the pelvic girdle. B. The auricular surfaces and tuberosities of the ilium and sacrum are demonstrated in an “opened book” view.
SACRO-ILIAC JOINTS
The sacro-iliac joints are strong, weight-bearing compound joints, consisting of an anterior synovial joint (between the ear-shaped auricular surfaces of the sacrum and ilium, covered with articular cartilage) and a posterior syndesmosis (between the tuberosities of these bones) (Fig. 3.4B). The auricular surfaces of this synovial joint have irregular but congruent elevations and depressions that interlock (Figs. 3.5A–C). The sacro-iliac joints differ from most synovial joints in that limited mobility is allowed, a consequence of their role in transmitting the weight of most of the body to the hip bones.

FIGURE 3.5. Sacro-iliac joints and pubic symphysis with associated ligaments. A. The posterior half of a coronally sectioned pelvic girdle and its sacro-iliac joints are shown. The strong interosseous sacro-iliac ligaments lie deep (antero-inferior) to the posterior sacro-iliac ligaments and consist of shorter fibers connecting the tuberosity of the sacrum to the tuberosity of the ilium, suspending the sacrum from the ilia (left and right ilium) like the central portion of a suspension bridge is suspended from the pylons at each end. B. CT scan of the synovial and syndesmotic portions of the sacro-iliac joint. C. Because the articulating surfaces are irregular and slightly oblique, the anterior and posterior parts of the joint appear separately in an AP radiograph. D. The weight of the body is transmitted to the sacrum anterior to the axis of rotation at the sacro-iliac joint. The tendency for increased weight or force to rotate the upper sacrum anteriorly and inferiorly is resisted by the strong sacrotuberous and sacrospinous ligaments anchoring the inferior sacrum and coccyx to the ischium.
Weight is transferred from the axial skeleton to the ilia via the sacro-iliac ligaments (Fig. 3.4A), and then to the femurs during standing, and to the ischial tuberosities during sitting. As long as tight apposition is maintained between the articular surfaces, the sacro-iliac joints remain stable. Unlike a keystone at the top of an arch, the sacrum is actually suspended between the iliac bones and is firmly attached to them by posterior and interosseous sacro-iliac ligaments (Fig. 3.5A).
The thin anterior sacro-iliac ligaments are merely the anterior part of the fibrous capsule of the synovial part of the joint (Figs. 3.5A and 3.6). The abundant interosseous sacroiliac ligaments (lying deep between the tuberosities of the sacrum and ilium and occupying an area of approximately 10 cm2) are the primary structures involved in transferring the weight of the upper body from the axial skeleton to the two ilia of the appendicular skeleton (Fig. 3.5A).

FIGURE 3.6. Ligaments of pelvic girdle. The ligaments of hip joint (shown but not labeled) are identified in Chapter 5 (Lower Limb).
The posterior sacro-iliac ligaments are the posterior external continuation of the same mass of fibrous tissue (Figs. 3.5A and 3.6). Because the fibers of the interosseous and posterior sacro-iliac ligaments run obliquely upward and outward from the sacrum, the axial weight pushing down on the sacrum actually pulls the ilia inward (medially) so that they compress the sacrum between them, locking the irregular but congruent surfaces of the sacro-iliac joints together. The iliolumbar ligaments are accessory ligaments to this mechanism (Fig. 3.6).
Inferiorly, the posterior sacro-iliac ligaments are joined by fibers extending from the posterior margin of the ilium (between the posterior superior and posterior inferior iliac spines) and the base of the coccyx to form the massive sacrotuberous ligament (Fig. 3.6). This ligament passes from the posterior ilium and lateral sacrum and coccyx to the ischial tuberosity, transforming the sciatic notch of the hip bone into a large sciatic foramen. The sacrospinous ligament, passing from lateral sacrum and coccyx to the ischial spine, further subdivides this foramen into greater and lesser sciatic foramina.
Most of the time, movement at the sacro-iliac joint is limited by interlocking of the articulating bones and the sacro-iliac ligaments to slight gliding and rotary movements (Fig. 3.5D). When landing after a high jump or when weightlifting in the standing position, exceptional force is transmitted through the bodies of the lumbar vertebrae to the superior end of the sacrum. Because this transfer of weight occurs anterior to the axis of the sacro-iliac joints, the superior end of the sacrum is pushed inferiorly and anteriorly. However, rotation of the superior sacrum is counterbalanced by the strong sacrotuberous and sacrospinous ligaments that anchor the inferior end of the sacrum to the ischium, preventing its superior and posterior rotation (Figs. 3.5D and 3.6). By allowing only slight upward movement of the inferior end of the sacrum relative to the hip bones, resilience is provided to the sacro-iliac region when the vertebral column sustains sudden increases in force or weight.
PUBIC SYMPHYSIS
The pubic symphysis consists of a fibrocartilaginous interpubic disc and surrounding ligaments uniting the bodies of the pubic bones in the median plane (Fig. 3.7). The interpubic disc is generally wider in women. The ligaments joining the bones are thickened at the superior and inferior margins of the symphysis, forming superior and inferior pubic ligaments. The superior pubic ligament connects the superior aspects of the pubic bodies and interpubic disc, extending as far laterally as the pubic tubercles. The inferior (arcuate) pubic ligament is a thick arch of fibers that connects the inferior aspects of the joint components, rounding off the subpubic angle as it forms the apex of the pubic arch (Fig. 3.3). The decussating, fibers of the tendinous attachments of the rectus abdominis and external oblique muscles also strengthen the pubic symphysis anteriorly (see Chapter 2).

FIGURE 3.7. Pubic symphysis. A. The pubic symphysis is a secondary cartilaginous joint between the bodies of the pubic bones. B. Radiographic appearance of the pubic symphysis in the anatomical position. In this position, the bodies of the pubic bones are nearly horizontal, and the joint appears foreshortened.
LUMBOSACRAL JOINTS
L5 and S1 vertebrae articulate at the anterior intervertebral (IV) joint formed by the L5/S1 IV disc between their bodies (Fig. 3.4A) and at two posterior zygapophysial joints (facet joints) between the articular processes of these vertebrae (Fig. 3.1). The facets on the S1 vertebra face posteromedially, interlocking with the anterolaterally facing inferior articular facets of the L5 vertebra, preventing the lumbar vertebra from sliding anteriorly down the incline of the sacrum. These joints are further strengthened by fan-like iliolumbar ligaments radiating from the transverse processes of the L5 vertebra to the ilia (Fig. 3.6).
SACROCOCCYGEAL JOINT
The sacrococcygeal joint is a secondary cartilaginous joint (Fig. 3.4A) with an IV disc. Fibrocartilage and ligaments join the apex of the sacrum to the base of the coccyx. The anterior and posterior sacrococcygeal ligaments are long strands that reinforce the joint (Fig. 3.6).
PELVIC GIRDLE
Variations in Male and Female Pelves
 Although anatomical differences between male and female pelves are usually clear cut, the pelvis of any person may have some features of the opposite sex. The pelvic types shown in Figure B3.1A and C are most common in males, B and A in white females, and B and C in black females, whereas D is uncommon in both sexes. The gynecoid pelvis is the normal female type (Fig. B3.1B); its pelvic inlet typically has a rounded oval shape and a wide transverse diameter. An platypelloid or markedly android (masculine or funnel-shaped) pelvis in a woman may present hazards to successful vaginal delivery of a fetus (Fig. B3.1A).
Although anatomical differences between male and female pelves are usually clear cut, the pelvis of any person may have some features of the opposite sex. The pelvic types shown in Figure B3.1A and C are most common in males, B and A in white females, and B and C in black females, whereas D is uncommon in both sexes. The gynecoid pelvis is the normal female type (Fig. B3.1B); its pelvic inlet typically has a rounded oval shape and a wide transverse diameter. An platypelloid or markedly android (masculine or funnel-shaped) pelvis in a woman may present hazards to successful vaginal delivery of a fetus (Fig. B3.1A).

FIGURE B3.1.
In forensic medicine (the application of medical and anatomical knowledge for the purposes of law), identification of human skeletal remains usually involves the diagnosis of sex. A prime focus of attention is the pelvic girdle because sexual differences usually are clearly visible. Even fragments of the pelvic girdle are useful in determining sex.
Pelvic Diameters (Conjugates)
 The size of the lesser pelvis is particularly important in obstetrics because it is the bony canal through which the fetus passes during normal child birth. To determine the capacity of the female pelvis for childbearing, the diameters of the lesser pelvis are noted radiographically or manually during a pelvic examination. The minimum anteroposterior (AP) diameter of the lesser pelvis, the true (obstetrical) conjugate from the middle of the sacral promontory to the posterosuperior margin (closest point) of the pubic symphysis (Fig. B3.2A & B), is the narrowest fixed distance through which the baby’s head must pass in a vaginal delivery. This distance, however, cannot be measured directly during a pelvic examination because of the presence of the bladder. Consequently, the diagonal conjugate (Fig. B3.2B) is measured by palpating the sacral promontory with the tip of the middle finger, using the other hand to mark the level of the inferior margin of the pubic symphysis on the examining hand (Fig. B3.2C). After the examining hand is withdrawn, the distance between the tip of the index finger (1.5 cm shorter than the middle finger) and the marked level of the pubic symphysis is measured to estimate the true conjugate, which should be 11.0 cm or greater.
The size of the lesser pelvis is particularly important in obstetrics because it is the bony canal through which the fetus passes during normal child birth. To determine the capacity of the female pelvis for childbearing, the diameters of the lesser pelvis are noted radiographically or manually during a pelvic examination. The minimum anteroposterior (AP) diameter of the lesser pelvis, the true (obstetrical) conjugate from the middle of the sacral promontory to the posterosuperior margin (closest point) of the pubic symphysis (Fig. B3.2A & B), is the narrowest fixed distance through which the baby’s head must pass in a vaginal delivery. This distance, however, cannot be measured directly during a pelvic examination because of the presence of the bladder. Consequently, the diagonal conjugate (Fig. B3.2B) is measured by palpating the sacral promontory with the tip of the middle finger, using the other hand to mark the level of the inferior margin of the pubic symphysis on the examining hand (Fig. B3.2C). After the examining hand is withdrawn, the distance between the tip of the index finger (1.5 cm shorter than the middle finger) and the marked level of the pubic symphysis is measured to estimate the true conjugate, which should be 11.0 cm or greater.

FIGURE B3.2.
In all pelvic girdles, the ischial spines extend toward each other, and the interspinous distance between them is normally the narrowest part of the pelvic canal (the passageway through the pelvic inlet, lesser pelvis, and pelvic outlet) through which a baby’s head must pass at birth (Fig. B3.2B), but it is not a fixed distance (see the blue box “Relaxation of Pelvic Ligaments and Increased Joint Mobility During Pregnancy,” p. 336). During a pelvic examination, if the ischial tuberosities are far enough apart to permit three fingers to enter the vagina side by side, the subpubic angle is considered sufficiently wide to permit passage of an average fetal head at full term.
Pelvic Fractures
 Anteroposterior compression of the pelvis occurs during crush accidents (as when a heavy object falls on the pelvis, Fig. B3.3A). This type of trauma commonly produces fractures of the pubic rami. When the pelvis is compressed laterally, the acetabula and ilia are squeezed toward each other and may be broken.
Anteroposterior compression of the pelvis occurs during crush accidents (as when a heavy object falls on the pelvis, Fig. B3.3A). This type of trauma commonly produces fractures of the pubic rami. When the pelvis is compressed laterally, the acetabula and ilia are squeezed toward each other and may be broken.

FIGURE B3.3.
Fractures of the bony pelvic ring are almost always multiple fractures or a fracture combined with a joint dislocation. To illustrate this, try breaking a pretzel ring at just one point. Some pelvic fractures result from the tearing away of bone by the strong ligaments associated with the sacro-iliac joints. (These ligaments are shown in Figs 3.3 and 3.4A.)
Pelvic fractures can result from direct trauma to the pelvic bones, such as occurs during an automobile accident (Fig. B3.3A), or be caused by forces transmitted to these bones from the lower limbs during falls on the feet (Fig. B3.3B). Weak areas of the pelvis, where fractures often occur, are the pubic rami, the acetabula (or the area immediately surrounding them), the region of the sacro-iliac joints, and the alae of the ilium.
Pelvic fractures may cause injury to pelvic soft tissues, blood vessels, nerves, and organs. Fractures in the pubo-obturator area are relatively common and are often complicated because of their relationship to the urinary bladder and urethra, which may be ruptured or torn.
Falls on the feet or buttocks from a high ladder may drive the head of the femur through the acetabulum into the pelvic cavity, injuring pelvic viscera, nerves, and vessels. In individuals younger than 17 years of age, the acetabulum may fracture through the triradiate cartilage into its three developmental parts (Fig. 3.2C) or the bony acetabular margins may be torn away.
Relaxation of Pelvic Ligaments and Increased Joint Mobility in Late Pregnancy
 The larger cavity of the interpubic disc in females (Fig. 3.3) increases in size during pregnancy. This change increases the circumference of the lesser pelvis and contributes to increased flexibility of the pubic symphysis. Increased levels of sex hormones and the presence of the hormone relaxin cause the pelvic ligaments to relax during the latter half of pregnancy, allowing increased movement at the pelvic joints. Relaxation of the sacro-iliac joints and pubic symphysis permits as much as a 10–15% increase in diameters (mostly transverse, including the interspinous distance—Fig. B3.2A), facilitating passage of the fetus through the pelvic canal. The coccyx is also able to move posteriorly.
The larger cavity of the interpubic disc in females (Fig. 3.3) increases in size during pregnancy. This change increases the circumference of the lesser pelvis and contributes to increased flexibility of the pubic symphysis. Increased levels of sex hormones and the presence of the hormone relaxin cause the pelvic ligaments to relax during the latter half of pregnancy, allowing increased movement at the pelvic joints. Relaxation of the sacro-iliac joints and pubic symphysis permits as much as a 10–15% increase in diameters (mostly transverse, including the interspinous distance—Fig. B3.2A), facilitating passage of the fetus through the pelvic canal. The coccyx is also able to move posteriorly.
The one diameter that remains unaffected is the true (obstetrical) diameter between the sacral promontory and the posterosuperior aspect of the pubic symphysis (Fig. B3.2A & B). Relaxation of sacro-iliac ligaments causes the interlocking mechanism of the sacro-iliac joint to become less effective, permitting greater rotation of the pelvis and contributing to the lordotic (“swayback”) posture often assumed during pregnancy with the change in the center of gravity. Relaxation of ligaments is not limited to the pelvis, and the possibility of joint dislocation increases during late pregnancy.
Spondylolysis and Spondylolisthesis
 Spondylolysis is a defect allowing part of a vertebral arch (the posterior projection from the vertebral body that surrounds the spinal canal and bears the articular, transverse, and spinal processes) to be separated from its body. Spondylolysis of vertebra L5 results in the separation of the vertebral body from the part of its vertebral arch bearing the inferior articular processes (Fig. B3.4A). The inferior articular processes of L5 normally interlock with the articular processes of the sacrum. When the defect is bilateral, the body of the L5 vertebrae may slide anteriorly on the sacrum (spondylolisthesis) so that it overlaps the sacral promontory (Fig. B3.4B–C). The intrusion of the L5 body into the pelvic inlet reduces the AP diameter of the pelvic inlet, which may interfere with parturition (child-birth). It may also compress spinal nerves, causing low back or lower limb pain.
Spondylolysis is a defect allowing part of a vertebral arch (the posterior projection from the vertebral body that surrounds the spinal canal and bears the articular, transverse, and spinal processes) to be separated from its body. Spondylolysis of vertebra L5 results in the separation of the vertebral body from the part of its vertebral arch bearing the inferior articular processes (Fig. B3.4A). The inferior articular processes of L5 normally interlock with the articular processes of the sacrum. When the defect is bilateral, the body of the L5 vertebrae may slide anteriorly on the sacrum (spondylolisthesis) so that it overlaps the sacral promontory (Fig. B3.4B–C). The intrusion of the L5 body into the pelvic inlet reduces the AP diameter of the pelvic inlet, which may interfere with parturition (child-birth). It may also compress spinal nerves, causing low back or lower limb pain.

FIGURE B3.4. A. Comparison of a normal L5 vertebra with intact articular processes that prevent spondylolisthesis and an L5 vertebra with spondylolysis (A) resulting in spondylolisthesis (B). B. Interpretive figure of radiograph (C) demonstrating spondylolysis and spondylolisthesis.
Obstetricians test for spondylolisthesis by running their fingers along the lumbar spinous processes. An abnormally prominent L5 process indicates that the anterior part of L5 vertebra and the vertebral column superior to it may have moved anteriorly relative to the sacrum and the vertebral arch of L5. Medical images, such as sagittal magnetic resonance imaging (MRI), are taken to confirm the diagnosis, and to measure the AP diameter of the pelvic inlet.
The Bottom Line
PELVIS AND PELVIC GIRDLE
Pelvis: The pelvis is the space enclosed by the pelvic girdle, which is subdivided into the greater pelvis (the inferior part of the abdominal cavity, which receives the protection of the alae of the ilia) and the lesser pelvis (the space inside the bony ring of pelvis inferior to the pelvic brim). ♦ The lesser pelvis provides the skeletal framework for both the pelvic cavity and the perineum, which are separated by the musculofascial pelvic diaphragm. ♦ The term perineum refers both to the region that includes the anus and external genitalia and to a shallow compartment deep to that area. ♦ The inferior anterolateral abdominal wall, gluteal region, and perineum overlap the pelvis.
Pelvic girdle: The pelvic girdle is an articulated bony ring composed of the sacrum and two hip bones. Whereas the pelvic girdle is part of the appendicular skeleton of the lower limb, the sacrum is also part of the axial skeleton, continuous with the lumbar vertebrae superiorly and coccyx inferiorly. ♦ The hip bones are formed by the fusion of the ilium, ischium, and pubis. ♦ The primary functions of the pelvic girdle are bearing and transfer of weight; secondary functions include protection and support of abdominopelvic viscera and housing and attachment for structures of the genital and urinary systems. ♦ The pelvic girdle is in the anatomical position when its three anteriormost points (right and left ASISs and anterior aspect of pubic symphysis) lie in the same vertical plane. ♦ Male and female pelves are distinct. The characteristic features of the normal (gynecoid) female pelvis reflect the fact that the fetus must traverse the pelvic canal during childbirth. ♦ Because atypical female pelves may not be conducive to a vaginal birth, determination of the pelvic diameters is of clinical importance.
Joints of pelvis: The sacro-iliac joints are specialized compound synovial and syndesmotic joints, the structures of which reflect both the primary (weight-bearing/weight transfer and stability) and the secondary (parturition) functions of the pelvis. ♦ Strong interosseous and posterior sacro-iliac ligaments suspend the sacrum between the ilia, transferring weight and stabilizing the bony ring of the pelvis. ♦ The synovial joints allow slight but significant movement during childbirth, when the pubic symphysis and the ligaments are softened by hormones. ♦ To counterbalance the weight of the upper body and additional forces generated by activities such as jumping and load bearing, which are received by the superior sacrum anterior to the rotatory axis of the sacro-iliac joints, the inferior end of the sacrum is anchored to the ischium by the substantial sacrotuberous and sacrospinous ligaments.
PELVIC CAVITY
The abdominopelvic cavity extends superiorly into the thoracic cage and inferiorly into the pelvis, so that its superior and inferior parts are relatively protected (Fig. 3.8A). Perforating wounds in either the thorax or the pelvis may therefore involve the abdominopelvic cavity and its contents.

FIGURE 3.8. Thoracic and abdominopelvic cavities. A and C. These sections of the trunk show the relationship of the thoracic and abdominopelvic cavities. Although the greater pelvis and pelvic cavity are actually continuous, they are demarcated by the plane of the pelvic inlet (defined by the pelvic brim). B. The pelvic diaphragm is a dynamic barrier separating the lesser pelvis and the perineum, forming the floor of the former and roof of the latter.
The funnel-shaped pelvic cavity—the space bounded peripherally by the bony, ligamentous, muscular pelvic walls and floor—is the inferoposterior part of the abdominopelvic cavity. The pelvic cavity is continuous with the abdominal cavity at the pelvic inlet but angulated posteriorly from it (Fig. 3.8A & C). Although continuous, the abdominal and pelvic cavities are described separately for descriptive purposes, facilitating the regional approach.
The pelvic cavity contains the terminal parts of the ureters, the urinary bladder, rectum, pelvic genital organs, blood vessels, lymphatics, and nerves. In addition to these distinctly pelvic viscera, it also contains what might be considered an overflow of abdominal viscera: loops of small intestine (mainly ileum) and, frequently, large intestine (appendix and transverse and/or sigmoid colon).
The pelvic cavity is limited inferiorly by the musculofascial pelvic diaphragm, which is suspended above (but descends centrally to the level of) the pelvic outlet, forming a bowl-like pelvic floor. The pelvic cavity is bounded posteriorly by the coccyx and inferiormost sacrum, with the superior part of the sacrum forming a roof over the posterior half of the cavity (Fig. 3.8A & B).
The bodies of the pubic bones, and the pubic symphysis uniting them, form an antero-inferior wall that is much shallower (shorter) than the posterosuperior wall and ceiling formed by sacrum and coccyx. Consequently, the axis of the pelvis (a line in the median plane defined by the center point of the pelvic cavity at every level) is curved, pivoting around the pubic symphysis (Fig. 3.8A). The curving form of the axis and the disparity in depth between the anterior and posterior walls of the cavity are important factors in the mechanism of fetal passage through the pelvic canal.
Walls and Floor of Pelvic Cavity
The pelvic cavity has an antero-inferior wall, two lateral walls, a posterior wall, and a floor (Fig. 3.9A). The muscles forming the walls and floor of the pelvic cavity are demonstrated in Figure 3.10, and the proximal and distal attachments, innervation, and main actions of the muscles are described in Table 3.2.

FIGURE 3.9. Floor and walls of pelvis. A. The floor of the pelvis is formed by the pelvic diaphragm, encircled by and suspended in part from the pubic symphysis and pubic bones anteriorly, the ilia laterally, and the sacrum and coccyx posteriorly. Parts B through D show the staged reconstruction of the parietal structures of the right hemipelvis. B. Posterolaterally, the coccyx and inferior part of the sacrum are attached to the ischial tuberosity by the sacrotuberous ligament and to the ischial spine by the sacrospinous ligament. The obturator membrane, composed of strong interlacing fibers, fills the obturator foramen. C. The muscles of the lesser pelvis are added. The obturator internus pads the lateral wall of the pelvis, its fibers converging to escape posteriorly through the lesser sciatic foramen (see part B). D. The levator ani is added, suspended from a thickening in the obturator fascia (the tendinous arch), which extends from the pubic body to the ischial spine.

FIGURE 3.10. Muscles of pelvic walls and floor. A and B. The obturator internis and piriformis are muscles that act on the lower limb but are also components of the pelvic walls. C. The muscles of the levator ani and the coccygeus comprise the pelvic diaphragm that forms the floor of the pelvic cavity. The fascia covering the inferior surface of the pelvic diaphragm forms the “roof” of the perineum.
TABLE 3.2. MUSCLES OF PELVIC WALLS AND FLOOR

ANTERO-INFERIOR PELVIC WALL
The antero-inferior pelvic wall (more of a weight-bearing floor than an anterior wall in the anatomical position) is formed primarily by the bodies and rami of the pubic bones and the pubic symphysis (Figs. 3.7 and 3.9B–D). It participates in bearing the weight of the urinary bladder.
LATERAL PELVIC WALLS
The lateral pelvic walls are formed by the right and left hip bones, each of which includes an obturator foramen closed by an obturator membrane (Figs. 3.8C & 3.9B). The fleshy attachments of the obturator internus muscles cover and thus pad most of the lateral pelvic walls (Figs. 3.9C and 3.10A). The fleshy fibers of each obturator internus converge posteriorly, become tendinous, and turn sharply laterally to pass from the lesser pelvis through the lesser sciatic foramen to attach to the greater trochanter of the femur. The medial surfaces of these muscles are covered by obturator fascia, thickened centrally as a tendinous arch that provides attachment for the pelvic diaphragm (Fig. 3.9D).
POSTERIOR WALL (POSTEROLATERAL WALL AND ROOF)
In the anatomical position, the posterior pelvic wall consists of a bony wall and roof in the midline (formed by the sacrum and coccyx) and musculoligamentous posterolateral walls, formed by the ligaments associated with the sacro-iliac joints and piriformis muscles (Fig. 3.9A–C). The ligaments include the anterior sacro-iliac, sacrospinous, and sacrotuberous ligaments.
The piriformis muscles arise from the superior sacrum, lateral to its pelvic foramina (Figs. 3.9A and 3.10A). The muscles pass laterally, leaving the lesser pelvis through the greater sciatic foramen to attach to the superior border of the greater trochanter of the femur (Fig. 3.10B). These muscles occupy much of the greater sciatic foramen, forming the posterolateral walls of the pelvic cavity (Fig. 3.9A). Immediately deep (anteromedial) to these muscles (often embedded in the fleshy fibers) are the nerves of the sacral plexus (Fig. 3.9D). A gap at the inferior border of the piriformis allows passage of neurovascular structures between the pelvis and the perineum and lower limb (gluteal region).
PELVIC FLOOR
The pelvic floor is formed by the bowl- or funnel-shaped pelvic diaphragm, which consists of the coccygeus and levator ani muscles and the fascias (L. fasciae) covering the superior and inferior aspects of these muscles (Figs. 3.9A, 3.10C, and 3.11; Table 3.2). The pelvic diaphragm lies within the lesser pelvis, separating the pelvic cavity from the perineum, for which it forms the roof.

FIGURE 3.11. Pelvic diaphragm and anorectum in situ. A and B. The components of the pelvic diaphragm (levator ani and coccygeus) form the floor of the pelvic cavity and the roof of the perineum. B. The basin-like nature for which the pelvis was named is evident in this coronal section. The fat-filled ischio-anal fossae of the perineum also lie within the bony ring of the lesser pelvis.
The attachment of the diaphragm to the obturator fascia divides the obturator internus into a superior pelvic portion and an inferior perineal portion (Fig. 3.11B). Medial to the pelvic portions of the obturator internus muscles are the obturator nerves and vessels and other branches of the internal iliac vessels.
The coccygeus muscles arise from the lateral aspects of the inferior sacrum and coccyx, their fleshy fibers lying on and attaching to the deep surface of the sacrospinous ligament (Fig. 3.9B & C). The levator ani (a broad muscular sheet) is the larger and more important part of the pelvic floor. It is attached to the bodies of the pubic bones anteriorly, to the ischial spines posteriorly, and to a thickening in the obturator fascia (the tendinous arch of the levator ani) between the two bony sites on each side.
The pelvic diaphragm thus stretches between the anterior, the lateral, and the posterior walls of the lesser pelvis, giving it the appearance of a hammock suspended from these attachments, closing much of the ring of the pelvic girdle. An anterior gap between the medial borders of the levator ani muscles of each side—the urogenital hiatus—gives passage to the urethra and, in females, the vagina (Fig. 3.9A).
The levator ani consists of three parts, often poorly demarcated but designated according to attachments and fiber course (Figs. 3.9A & D, 3.10C, and 3.11):
• Puborectalis: the thicker, narrower, medial part of the levator ani, consisting of muscle fibers that are continuous between the posterior aspects of the bodies of the right and left pubic bones. It forms a U-shaped muscular sling (puborectal sling) that passes posterior to the anorectal junction (Fig. 3.12), bounding the urogenital hiatus. This part plays a major role in maintaining fecal continence.
• Pubococcygeus: the wider but thinner intermediate part of the levator ani, which arises lateral to the puborectalis from the posterior aspect of the body of the pubis and anterior tendinous arch (Figs. 3.9A & D, 3.10C, and 3.11). It passes posteriorly in a nearly horizontal plane; its lateral fibers attach to the coccyx and its medial fibers merge with those of the contralateral muscle to form a fibrous raphe or tendinous plate, part of the anococcygeal body or ligament between the anus and the coccyx (often referred to clinically as the “levator plate”).

FIGURE 3.12. Puborectalis muscle. Most of the left hip bone has been removed to demonstrate that this part of the levator ani is formed by continuous muscle fibers following a U-shaped course around the anorectal junction. The puborectalis thus forms a puborectal sling, the tonus of which is responsible for maintaining the anorectal angle (perineal flexure).
Shorter muscular slips of the pubococcygeus extending medially and blending with the fascia around midline structures are named for the structure near their termination: pubovaginalis (females), puboprostaticus (males), puboperinealis, and pubo-analis.
• Iliococcygeus: the posterolateral part of the levator ani, which arises from the posterior tendinous arch and ischial spine. It is thin and often poorly developed (appearing more aponeurotic than muscular), and also blends with the anococcygeal body posteriorly.
The levator ani forms a dynamic floor for supporting the abdominopelvic viscera. It is tonically contracted most of the time to support the abdominopelvic viscera, and to assist in maintaining urinary and fecal continence. It is actively contracted during activities such as forced expiration, coughing, sneezing, vomiting, and fixation of the trunk during strong movements of the upper limbs (e.g., when lifting heavy objects), primarily to increase support of the viscera during periods of increased intra-abdominal pressure, and perhaps secondarily to contribute to the increased pressure (to aid expulsion).
Penetrated centrally by the anal canal, the levator ani is funnel shaped, with the U-shaped puborectalis looping around the “funnel spout”; its tonic contraction bends the anorectum anteriorly. Active contraction of the (voluntary) puborectalis portion is important in maintaining fecal continence immediately after rectal filling or during peristalsis when the rectum is full and the involuntary sphincter muscle is inhibited (relaxed).
The levator ani must relax to allow urination and defecation. The increased intra-abdominal pressure for defecation is provided by contraction of the (thoracic) diaphragm and muscles of the anterolateral abdominal wall. Acting together, the parts of the levator ani elevate the pelvic floor after their relaxation and the consequent descent of the pelvic diaphragm that occurs during urination and defecation.
Peritoneum and Peritoneal Cavity of Pelvis
The parietal peritoneum lining the abdominal cavity continues inferiorly into the pelvic cavity, but does not reach the pelvic floor. Instead, it reflects onto the pelvic viscera, remaining separated from the pelvic floor by the pelvic viscera and the surrounding pelvic fascia (Table 3.3). Except for the ovaries and uterine tubes, the pelvic viscera are not completely ensheathed by the peritoneum, lying inferior to it for the main part. Only their superior and superolateral surfaces are covered with peritoneum. Only the uterine tubes (except for their ostia, which are open) are intraperitoneal and suspended by a mesentery. The ovaries, although suspended in the peritoneal cavity by a mesentery, are not covered with glistening peritoneum; instead a special, relatively dull epithelium of cuboidal cells (germinal epithelium) covers them.

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


