Overview
Although many conditions that affect adults also affect children, pediatric pathology includes many conditions found only in patients younger than 18 years of age. This chapter will address many of these conditions.
One group of conditions involving the infant population is congenital anomalies. Several terms are important to remember when discussing congenital anomalies. A malformation is a congenital anomaly due to an intrinsic defect in development. A disruption occurs when a normally developing organ is secondarily damaged by another process. For example, in amniotic band syndrome, a fragment of the amniotic membrane wraps around a portion of the body and damages or amputates it. A deformation is an abnormal development of an organ due to an extrinsic process. A sequence is a collection of several anomalies, all of which are due to one malformation, disruption, or deformation. For example, Potter sequence is due to oligohydramnios and includes flat facies, small chest, hypoplastic lungs, club foot (talipes equinovarus), and nodules in the amniotic sac. Finally, a syndrome is a group of related anomalies. Common congenital anomalies include clubfoot, patent ductus arteriosus, ventricular septal defect, and cleft lip or cleft palate. Although most congenital anomalies are diagnosed during infancy, they are present and can cause complications into adulthood.
This chapter will discuss causes of congenital anomalies and major congenital anomalies by organ system. Also discussed are conditions diagnosed in the pediatric population such as prematurity, perinatal infections, hydrops fetalis, sudden infant death syndrome (SIDS), and select pediatric tumors, including neuroblastoma and Wilms tumor.
Causes of Congenital Anomalies
Overview: The causes of congenital anomalies are genetic, environmental, and multifactorial; however, the etiology of many congenital anomalies is unknown. Two common environmental causes of congenital anomalies are nicotine and maternal diabetes mellitus.
- Nicotine: Use of nicotine when pregnant predisposes the mother to a high risk for spontaneous abortion, placental abruption, premature labor, or placental abnormalities.
- Maternal diabetes mellitus: Predisposes to a large-for-gestational-age fetus, neural tube defects, and neonatal hypoglycemia. The most common associated anomalies are cardiac. The most severe associated disorder is caudal regression syndrome (also referred to as “mermaid syndrome”), which causes fused, malformed lower extremities and sacral agenesis.
Major Congenital Anomalies by Organ System
Ventricular septal defect, atrial septal defect, patent ductus arteriosus, and tetralogy of Fallot are only a few of many cardiac congenital anomalies (see Chapter 10).
Central nervous system anomalies: Anencephaly and holoprosencephaly are only two of many congenital anomalies of the central nervous system (see Chapter 11).
Respiratory system congenital anomalies: Although there are other congenital anomalies of the respiratory system, only pulmonary sequestration and foregut cysts will be discussed below.
- Basic description: Discrete region of lung tissue that has no connection to the airway.
- Forms
- Extralobar sequestration: Discrete mass of lung tissue occurring outside the lungs. Infants can present with a mass lesion.
- Intralobar sequestration: Discrete mass of lung tissue occurring within one of the lung lobes, yet has no connection to the airway. Patients can present with symptoms of bronchopneumonia or bronchiectasis.
- Extralobar sequestration: Discrete mass of lung tissue occurring outside the lungs. Infants can present with a mass lesion.
- Basic description: Cyst derived from an abnormally detached portion of the foregut that can arise within the mediastinum or pulmonary hilum.
- Clinical presentation: Can be asymptomatic or present because of mass effects or because it has become infected.
Gastrointestinal tract and pancreatic congenital anomalies: Although there are many congenital anomalies of the gastrointestinal tract and pancreas, four of the more common anomalies are tracheo-esophageal fistula, omphalocele, gastroschisis, and pancreas divisum, which are discussed below.
- Basic description: Condition associated with an atretic esophagus with a fistulous connection to the trachea. The most common variant is a blind-ended proximal esophagus with a distal esophagus that connects to the trachea.
- Clinical presentation: Aspiration of food with potential for suffocation or development of pneumonia.
Omphalocele: Infants have herniated abdominal organs in a membranous sac composed of amnion and peritoneum. The condition is due to failure of formation of the abdominal wall musculature. The umbilical cord arises from the dome of the membranous sac.
Gastroschisis: Infants have failure of formation of the abdominal wall with the resultant evisceration of abdominal organs. The abdominal organs are present outside the peritoneal cavity, just to the right of the umbilical cord, and are not covered by a membranous sac (Figure 7-1).
Figure 7-1.
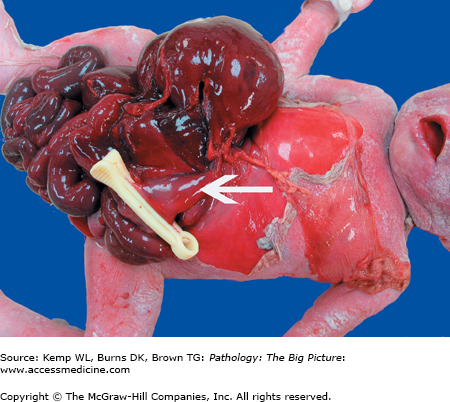
Gastroschisis. This infant had extrusion of the liver, small intestine, and large intestine through a defect in the abdominal wall. Note that the extruded abdominal contents are not covered by a thin membranous sac, and that they exit the abdominal wall to the right of the umbilicus (arrow).
Pancreas divisum: Pancreas divisum is due to failure of the dorsal and ventral pancreatic ducts to fuse, resulting in drainage of most of the organ through the dorsal pancreatic duct (Santorini) and smaller minor papilla. This congenital anomaly can lead to stenosis of the duct and resultant chronic pancreatitis.
Renal congenital anomalies: Although there are many congenital anomalies involving the kidneys, only agenesis of the kidney, ectopic kidney, and horseshoe kidney will be discussed below.
Agenesis of the kidney: Bilateral renal agenesis (i.e., failure of formation of both kidneys) will cause the death of an infant; unilateral agenesis is compatible with life.
Ectopic kidney: The kidney is abnormally located near the pelvic brim or within the pelvis. Abnormal location can lead to kinking of the urethra and predispose to pyelonephritis.
Horseshoe kidney: While commonly associated with Turner syndrome, horseshoe kidneys (usually with fusion of the lower poles of both kidneys) are a relatively common sporadic renal congenital anomaly.
Hypospadias and epispadias: In hypospadias, the urethral opening is abnormally located on the ventral surface of the penis; in epispadias, the urethral opening is located on the dorsal surface of the penis. The anomaly can be associated with other anomalies of the genitourinary tract, and can predispose to sterility and to urinary tract infections.
Prematurity and Its Complications
Basic description of prematurity: Age at delivery is less than 37 weeks’ gestation (for singleton pregnancy).
Risk factors for prematurity: Premature rupture of membranes, infections such as chorioamnionitis, maternal genitourinary abnormalities, twin or multiple gestation pregnancies, and preeclampsia.
Causes of prematurity: The causes of prematurity can be grouped into fetal, placental, and maternal categories.
Fetal causes of prematurity
- Specific fetal cause of prematurity: Chorioamnionitis.
- Result of fetal cause of prematurity: Small-for-gestational-age infant with symmetric growth retardation (also called proportionate fetal growth restriction because the entire body is small).
- Specific fetal cause of prematurity: Chorioamnionitis.
Placental causes of prematurity
- Specific placental causes of prematurity: Uteroplacental insufficiency, such as occurs with a single umbilical artery, placental infarction, and placenta previa.
- Result of placental cause of prematurity: Small-for-gestational-age infant with asymmetric growth retardation (also called disproportionate growth restriction). The head is normal size and the body is small; the head receives a disproportionate amount of oxygen and nutrients to preserve its development.
- Specific placental causes of prematurity: Uteroplacental insufficiency, such as occurs with a single umbilical artery, placental infarction, and placenta previa.
Maternal causes of prematurity
- Specific maternal causes of prematurity: Preeclampsia, maternal hypertension, alcohol and nicotine use, and maternal malnutrition.
- Result of maternal cause of prematurity: Small-for-gestational-age infant.
- Specific maternal causes of prematurity: Preeclampsia, maternal hypertension, alcohol and nicotine use, and maternal malnutrition.
Complications of prematurity: The three main complications of prematurity are hyaline membrane disease, necrotizing enterocolitis, and germinal matrix hemorrhage.
Basic description: Condition due to deficiency of pulmonary surfactant, which occurs because fetal lungs are not fully developed.
Pathogenesis: Decreased surfactant leads to atelectasis, which causes hypoxemia and carbon dioxide retention. Hypoxemia and carbon dioxide retention lead to acidosis, which contributes to hypoperfusion of the pulmonary parenchyma and eventually to endothelial and epithelial damage.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


