Patient Story
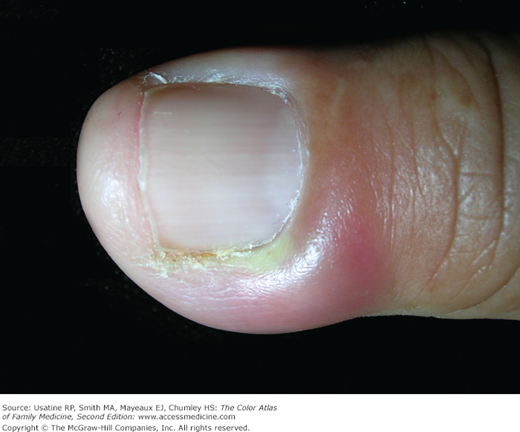
A 41-year-old woman presented with a 3-day history of localized pain, redness, and tenderness of the lateral nailfold of the index finger. A small abscess had developed in the last 24 hours at the nail margin (Figure 194-1). After informed consent was given, a digital block was performed. This acute paronychia was treated with incision and drainage using a #11 scalpel (Figure 194-2). A significant amount of pus was drained. She soaked her finger four times daily as directed. Two days later the patient’s finger was much better and the culture grew out Staphylococcus aureus. Draining the abscess was sufficient treatment.

Introduction
Paronychia is a localized, superficial infection or abscess of the nailfolds. It is one of the most common infections of the hand. Paronychia can be acute or chronic. Acute paronychia usually presents as an acutely painful abscess in the nailfold. Chronic paronychia is defined as being present for longer than 6 weeks’ duration. It is a generalized red, tender, swelling of the proximal or lateral nailfolds. It is usually nonsuppurative and is more difficult to treat.
Epidemiology
Paronychia is the most common infection of the hand, representing 35% of all hand infections in the United States.1
Etiology and Pathophysiology
- Paronychial infections develop when a disruption occurs between the seal of the nailfold and the nail plate or the skin of a nailfold is disrupted and allows a portal of entry for invading organisms.2
- Acute paronychia is most commonly caused by S. aureus, followed by streptococci and Pseudomonas (Figures 194-1, 194-2, 194-3, 194-4, and 194-5).1
- Chronic paronychia more likely results from chronic Candida albicans (95%) (Figures 194-6 and 194-7). Other rare causes include atypical Mycobacteria and Gram-negative rods. There is some evidence that chronic paronychia is at least partially an eczematous process and that Candida infection is a secondary phenomenon.3
- Untreated persistent chronic paronychia may cause horizontal ridging, undulations, and other changes to the nail plate (Figures 194-6 and 194-7).







