Paraesophageal Hernia—Open Repair
W. Scott Melvin
Kyle A. Perry
Paraesophageal hiatal hernia is a relatively rare condition that was first identified on postmortem examination in 1903, and by upper gastrointestinal contrast radiography in 1926. Since that time, the importance of these hernias has been recognized due to their propensity to develop potentially life-threatening complications including gastric volvulus with subsequent strangulation and perforation. Management of paraesophageal hernias has changed considerably during the past 20 years, and several areas of controversy remain as techniques continue to evolve. Although laparoscopic paraesophageal hernia repair has gained increased acceptance, circumstances exist when an open abdominal or thoracic approach is necessary, and surgeons should be familiar with these techniques.
Hiatal hernias occur in approximately 10% of the population, with approximately 10% of these being paraesophageal hernias. Although congenital paraesophageal hernias have been reported, the vast majority of these hernias are believed to be acquired. The underlying cause of hiatal enlargement is unknown, but may be related to metabolic defects affecting the extracellular matrix composition with the supporting ligaments of the gastroesophageal junction, increased intra-abdominal pressure, or inherent weakness of the diaphragmatic tissues. Paraesophageal hernias typically present later in life with a two to one female preponderance, and are occasionally seen as a complication of antireflux surgery. There is also a familial occurrence that confers a 20-fold increased risk in younger siblings of children with a hiatal hernia.
Gastric volvulus, first described by Berti in 1896, is defined as the rotation of the stomach greater than 180 degrees around a fixed axis of rotation. Gastric strangulation from acute gastric volvulus is a dreaded complication of paraesophageal hernia and it remains the driving force for recommending elective repair of asymptomatic hernias. Gastric strangulation occurs in up to 28% of cases of acute gastric volvulus, and may progress to gastric necrosis, perforation, and severe sepsis leading to cardiovascular collapse if it is not diagnosed quickly and aggressively managed. The true incidence of gastric volvulus remains unknown, but it affects males and females equally. Approximately 20% of cases occur in infants and young children, with the remainder occurring in adults older than 50 years of age.
The esophagus enters the abdomen via the esophageal hiatus of the diaphragm. In most patients the limbs of the right diaphragmatic crus comprise this opening, although varying degrees of contribution
from the left crus may be present. Although not anatomically correct, most surgical descriptions of hiatal dissection, including those presented here, refer to these limbs as the right and left diaphragmatic crura. The phrenoesophageal membrane anchors the intra-abdominal esophagus to the diaphragm and tethers the squamocolumnar junction within or just below the diaphragmatic hiatus, preventing displacement of the stomach above the diaphragm. Derangements of this normal esophagogastric anatomy produce herniation of the stomach thorough the esophageal hiatus into the thoracic cavity. Hiatal hernias are classified as types I to IV, with types II to IV representing forms of paraesophageal hernia (Fig. 1).
from the left crus may be present. Although not anatomically correct, most surgical descriptions of hiatal dissection, including those presented here, refer to these limbs as the right and left diaphragmatic crura. The phrenoesophageal membrane anchors the intra-abdominal esophagus to the diaphragm and tethers the squamocolumnar junction within or just below the diaphragmatic hiatus, preventing displacement of the stomach above the diaphragm. Derangements of this normal esophagogastric anatomy produce herniation of the stomach thorough the esophageal hiatus into the thoracic cavity. Hiatal hernias are classified as types I to IV, with types II to IV representing forms of paraesophageal hernia (Fig. 1).
Ninety percent of hiatal hernias are type I (Fig. 1A), or sliding, hiatal hernias in which the gastric cardia herniates upward with proximal migration of the lower esophageal sphincter (LES) into the thorax. This produces attenuation of the phrenoesophageal membrane, but it remains intact. The term sliding hiatal hernia applies here because the gastric wall comprises a portion of the hernia sac, analogous to retroperitoneal structures in sliding groin hernias.
Type II, III, and IV hiatal hernias represent forms of paraesophageal herniation. True paraesophageal (type II) hernias are uncommon, constituting about 3% of all hiatal hernias (Fig. 1B). In this case, the gastroesophageal junction remains fixed in its normal anatomic location and the gastric fundus herniates through an enlarged hiatus. “Parahiatal” hernias may occur in a position adjacent to, but distinct from, the anatomically intact esophageal hiatus; however, these have been reported to comprise only 0.2% of cases in large series of hiatal hernia repairs. These hernias typically occur on the left side and contain the fundus of the stomach producing a clinical picture and radiographic findings indistinguishable from type II paraesophageal hernias. Type III hiatal hernias involve elements of both type I and II hernias and represent the majority of paraesophageal hernias presenting for surgical repair (Fig. 1C). Most often, enlargement of a type I hernia defect allows cephalad migration of the stomach in response to the transdiaphragmatic pressure gradient. A true hernia sac is present with fundic herniation and proximal migration of the gastroesophageal junction into the thorax. This type of hernia is associated with laxity of the elements that retain normal gastric position, and the natural history is to progress to complete gastric herniation with the appearance of an upside-down intrathoracic stomach on contrast radiography (Fig. 2). Large hernia defects that contain other viscera or abdominal organs are referred to as type IV hiatal hernias, but these hernias are best thought of as a subgroup of type III.
This classification system can lead to confusion as some hernias may appear to be either a sliding or paraesophageal hiatal hernia depending on patient position. Thus, the term “giant paraesophageal hernia” has been used to describe the large hernias typically classified as type III and IV hiatal hernia. This term refers to hernias in which at least half of the stomach is located within the thorax on contrast radiography, the hernia measures at least 6 cm in length on preoperative endoscopy, or a distance between the crura of at least 5 cm is noted on intraoperative inspection. Giant hiatal hernias are repaired using the same principles required for all paraesophageal hernias, but the large hernia sac and propensity for esophageal shortening make these cases especially challenging.
The anatomic classification of gastric volvulus is based on the axis of rotation (Fig. 3). Organoaxial volvulus is the most common type, and it accounts for almost all cases of acute gastric volvulus. This involves rotation of the stomach around the anatomic (longitudinal) axis, represented as a line drawn from the cardia to the pylorus, frequently resulting in gastric strangulation. In mesoentericoaxial volvulus, the antrum of the stomach rotates anteriorly and superiorly around a transverse axis that extends from the mid-lesser curvature to the mid-greater curvature. The rotation is typically incomplete and results in intermittent gastric obstruction, rather than acute strangulation.
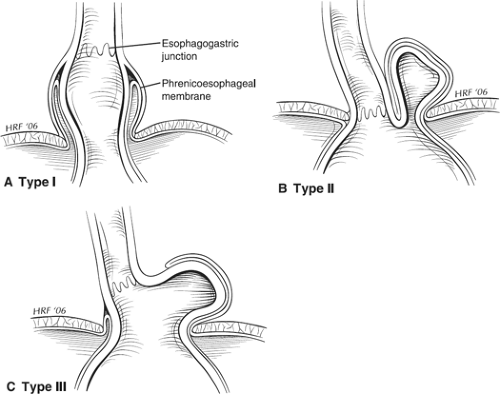 Fig. 1. Classification of hiatal hernia A: Type I, sliding B: Type II, pure paraesophageal C: Type III, mixed hernia. |
Approximately half of all paraesophageal hernias are clinically silent and become apparent on imaging studies obtained for another reason. Symptoms are caused either by obstruction of the stomach or distal esophagus or by gastroesophageal reflux related to LES incompetence. Paraesophageal hernia (PEH) most commonly present with symptoms of gastric obstruction including epigastric or chest pain, dysphagia, emesis, and postprandial fullness. Displacement of the LES into the thorax and loss of the angle of His may produce symptoms commonly associated with sliding hiatal hernias such as heartburn, chronic cough, regurgitation, and aspiration. Many of the signs and symptoms of PEH are nonspecific and may mimic those of acute myocardial infarction, gastric ulcer, or pneumonia. One-third of patients present with iron deficiency anemia secondary to chronic blood loss from erosions of the gastric mucosa caused
by repeated movement across the hiatus, a phenomenon originally described by Collis in 1957, or from an ulcer at the level of the diaphragm described by Cameron.
by repeated movement across the hiatus, a phenomenon originally described by Collis in 1957, or from an ulcer at the level of the diaphragm described by Cameron.
Acute gastric volvulus typically presents with a history of dysphagia and high gastric obstruction. In 1904, Borchardt described the classic symptom triad of severe epigastric pain, retching and inability to vomit, and inability to pass an nasogastric (NGT). Patients may also present with severe chest pain and minimal abdominal findings as the incarcerated segment is often located within the chest. Many patients present with intermittent acute symptoms, and a history of multiple emergency room visits for cardiac events is common. In patients with mesenteroaxial gastric volvulus, diaphragmatic defects are not as common, and ligamentous laxity, aerophagia, or postsurgical changes predominate.
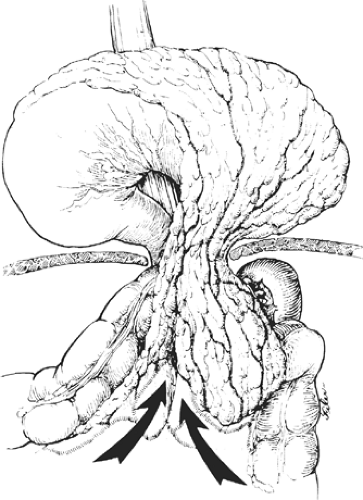 Fig. 2. Large type III paraesophageal hernia with a large hernia sac and an upside-down intrathoracic stomach. |
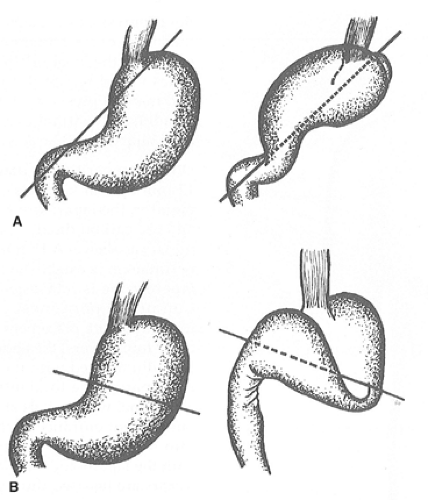 Fig. 3. Types of gastric volvulus associated with paraesophageal hernia A: Organoaxial volvulus B: Mesentericoaxial volvulus. Line indicates axis of volvulus. |
In the acute setting of foregut obstruction, chest X-ray typically demonstrates a retrocardiac air-fluid level and often a second one below the diaphragm. Pleural effusion, pneumothorax, and pneumoperitoneum are ominous findings that mandate exploration as they are often associated with ischemia and perforation. A barium study will reveal obstruction at the level of the volvulus and can be used as a confirmatory study in this setting if the diagnosis remains uncertain. In the setting of ischemia, the presentation is one of septic shock, with epigastric pain and resultant multiorgan system dysfunction. It should be emphasized that the catastrophic presentations of PEH are quite uncommon.
Several tests may be used to classify the hernia, degree of gastroesophageal reflux, and esophageal motility prior to elective repair. Barium esophagram may suggest the presence of a shortened esophagus and classify the hernia to aid in decision making, especially in frail patients with asymptomatic hernias. In some patients, an upper gastrointestinal series will show complete gastric obstruction due to gastric volvulus, which indicates a need for urgent surgical repair. Upper endoscopy is required to inspect for gastric ischemia, ulceration, erosion, or cancer. A paraesophageal hernia is identified on retroversion of the scope by noting a separate orifice adjacent to the gastroesophageal junction into which gastric rugal folds ascend. If a gastric ulcer is present, elective surgery should be delayed until after the ulcer is healed, or at least 6 weeks of proton pump inhibitor treatment have been completed. Esophageal
manometry can be useful in identifying esophageal motility disorders, which may preclude the use of full fundoplication, but may not be technically possible due to difficulties positioning the catheter beyond the LES. Ambulatory pH testing is rarely useful in evaluation of PEH because the goals of treatment typically involve addressing symptoms related to mechanical obstruction rather than the control of gastroesophageal reflux.
manometry can be useful in identifying esophageal motility disorders, which may preclude the use of full fundoplication, but may not be technically possible due to difficulties positioning the catheter beyond the LES. Ambulatory pH testing is rarely useful in evaluation of PEH because the goals of treatment typically involve addressing symptoms related to mechanical obstruction rather than the control of gastroesophageal reflux.
The repair of paraesophageal hernias may be approached via thoracotomy, laparotomy, or laparoscopy. The principles of proper surgical repair are the same with each approach:
Complete reduction and excision of the hernia sac
Reduction of the herniated stomach and 2 to 3 cm of distal esophagus into the abdominal cavity
Repair of the diaphragmatic hiatus
It has been generally accepted that reasonable surgical candidates should undergo repair regardless of symptoms. This recommendation is based on early series that showed an increased mortality after emergency surgery of 30% compared with 1% in elective cases. In 1967, Skinner and Belsey found that 6 of 21 patients with a known diagnosis of paraesophageal hernia died from complications of their hernia when followed conservatively for 5 years.
Other studies have suggested differences in both the natural history of the disease and operative outcomes. Allen et al. followed 23 patients who refused operative repair of paraesophageal hernias for a median follow-up of 78 months without development of any life-threatening complications. Others have advocated that asymptomatic or minimally symptomatic paraesophageal hernias may be managed by a strategy of “watchful waiting” with emergency surgery required in only 1.2% of cases with an operative mortality of 5.4% in this setting. A recent retrospective review of 127 patients undergoing open transabdominal PEH repair in a single institution, however, found emergent surgical repair carried a mortality rate of 22%, compared with 1% for patients undergoing elective repair. In this series, emergent repair was an independent predictor of in hospital mortality, major complications, readmission to an intensive care unit, and postoperative length of hospital stay.
Our current recommendation is that all type II hernias should be repaired, and consideration should be given to type III hernias regardless of symptoms. However, in the case of an elderly, frail patient with significant comorbidities it may be appropriate to decide on a course of watchful waiting due to increased risks associated with surgical repair in these patients.
Traditionally, transthoracic repair of paraesophageal hernias has been advocated. Approaching these via thoracotomy provides excellent visualization of the hernia sac from within the mediastinum, allows extensive esophageal mobilization under direct vision, and provides the easiest approach for esophageal lengthening procedures. However, this approach has been associated with longer hospital stay, need for tube thoracostomy, and increased pulmonary complication rates and incisional discomfort. Also, blind reduction of the stomach also leaves the potential for recurrence of organoaxial rotation leading to postoperative intra-abdominal gastric volvulus. Given the high morbidity rates and increased length of hospital stay associated with the transthoracic approach, most paraesophageal hernias are now repaired using an open or laparoscopic transabdominal approach.
Laparoscopic paraesophageal hernia repair has gained popularity and has been proven feasible, safe, and effective. Laparoscopy provides an attractive option because it combines some of the advantages of both thoracotomy (access to the hiatus, ability to perform extensive mobilization of the esophagus under direct vision) and laparotomy (lower morbidity, no need for single lung ventilation or postoperative chest tube). However, this is a challenging procedure that requires advanced laparoscopic skills and cannot be safely applied in all situations. Current indications for open transabdominal paraesophageal hernia repair include the following:
Gastric volvulus with acute peritonitis that cannot be relieved with gastric decompression.
Completion of a procedure that has been converted from a laparoscopic approach.
Reoperative surgery after a previous laparoscopic or open gastric surgery.
Patient preference.
Lack of expertise in advanced laparoscopic surgery.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


