Infantile Hypertrophic Pyloric Stenosis
Definition
This is a condition characterized by hypertrophy of the circular muscle of the gastric pylorus that obstructs gastric outflow.
Aetiology
The aetiology is unknown but it affects 1 in 450 children; 85% male, often firstborn; 20% have family history.
Clinical Features
- Non-bile-stained, projectile vomiting (after feeds) beginning at 2–6 weeks. May be bloodstained.
- Baby is hungry, constipated and dehydrated. Loss of H+ and Cl− from stomach and K+ from kidney causes hypochloraemic, hypokalaemic metabolic alkalosis.
- Palpable pyloric ‘tumour’ during a test feed or after vomiting.
- Gastric peristalsis may be seen. Ultrasound confirms the diagnosis.
Management
- Correct dehydration and electrolyte imbalance with 0.9% NaCl with added K+ (20 mmol/L) (contains 170 mmol Cl−/L) or 0.45% NaCl in dextrose 5% with added K+ (20 mmol/L)(contains 95 mmol Cl−/L). May take 24–48 hours to become normal.
- Ramstedt’s pyloromyotomy via transverse RUQ or per umbilical incision or laparoscopically. Normal feeding can commence within 24 hours.
Malrotation of the Gut
Definition and Aetiology
‘Malrotation’ is often used to describe a number of conditions (1 in 500 live births) that are caused by failure of the intestine to rotate into the correct anatomical position during embryological development. Most common types are incomplete rotation and non-rotation.
Complications that can result include:
- Volvulus (leading to risk of bowel necrosis); usually small bowel ± caecum/proximal colon.
- Internal herniation (via abnormally large paraduodenal recesses and paracolic spaces).
- Duodenal obstruction (usually incomplete and intermittent); often said to be due to Ladd’s bands (peritoneal tissue related to incomplete rotation) but probably due to rotation of a narrow small bowel mesenteric origin.
Clinical Features
Bile-stained vomiting in the newborn period is the most common presentation but older children may present with recurrent abdominal pain, abdominal distension and vomiting.
Management
- If diagnosed prior to acute presentation: surgery to ‘complete’ the non-rotation; placing the colon in the left abdomen and small bowel to the right (widening the mesenertic attachment with fixation).
- Acute presentations: release the obstructions, resect non-viable bowel ± fixation of the bowel in normal anatomical position.
Meckel’s Diverticulum
Definition
Meckel’s diverticulum is the remnant of the vitello-intestinal duct forming a blind-ending pouch on the antimesenteric border of the terminal ileum and is present in 2% of the population.
Clinical Features
Most are asymptomatic.
May present with:
- Rectal bleeding (often due to ulceration of the normal ileal mucosa opposite the diverticulum due to acid secreting (gastric antral type) epithelium within the diverticulum – detectable by technetium pertechnate scan in 70% of cases.
- ‘Appendicitis’ (Meckel’s diverticulitis).
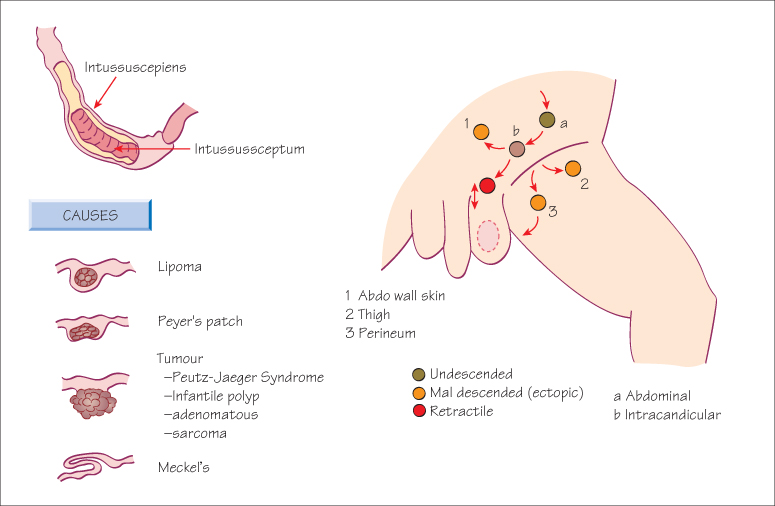
- Acute ileoileal intussusception.
- Volvulus (due to intestine-vitelline band/duct with small bowel rotation around it).
Management
Surgical excision, even if found incidentally.
Paediatric ‘General’ Surgery/2
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


