Definitions
A traumatic brain injury (TBI) or head injury is the process whereby trauma to the head results in skull and/or brain inury. Primary brain injury is the damage that occurs to the brain immediately as the result of the trauma. The degree of primary brain injury is directly related to the location of injury, the amount of energy transfered to the head and the rate of energy transfer. Prevention (e.g. helmets, airbags) is the only way to reduce primary injury (deflecting penetration/energy and slowing energy transfer).
Secondary brain injury is the damage that develops later as a result of complications. Secondary damage results from hypoxia and/or hypercarbia (respiratory complications, e.g. airway obstruction), hypovolaemic shock, intracranial bleeding, cerebral oedema, epilepsy, infection and hydrocephalus. Brain death is defined as the absence of brain function.
- Prevention of secondary brain injury caused by hypoxia and hypotension is the most important objective of head injury care.
- A full trauma survey (see Chapter 41) must be carried out on all patients with head injuries.
- Head injury does not cause hypovolaemic shock – look for another cause.
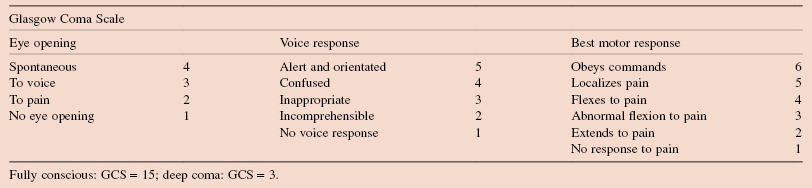
- The GCS provides a simple method of monitoring global CNS function over a period rather than a precise index of brain injury at any one time.
- CT scanning is the investigation of choice to assess the head/brain but transfer to CT scan is complex and requires optimum stabilization of the patient to perform.
- 100% of those with severe head injury and 60% of those with moderate head injury will be permanently disabled.
Epidemiology
Head injury is very common. RTAs, falls, assaults and sports injuries are common causes. A million patients each year present to emergency departments in the UK with head injury and about 5000 patients die each year following head injuries.
Pathophysiology
Closed Head Injury
Direct Blow
May cause damage to the brain at the site of the blow (coup injury) or to the side opposite the blow when the brain moves within the skull and hits the opposite wall (contrecoup injury).
Rotation/Deceleration
Neck flexion, extension or rotation results in the brain striking bony points within the skull (e.g. the wing of the sphenoid bone). Severe rotation also causes shear injuries within the white matter of the brain and brainstem, causing axonal injury and intracerebral petechial haemorrhages.
Crush
The brain is often remarkably spared direct injury unless severe (especially in children with elastic skulls).
Penetrating Head Injury
Missiles tend to cause loss of tissue with injury proportionate. Brain swelling – less of a problem due to the skull disruption automatically decompressing the brain. High velocity injuries (bullets) worse than low velocity due to shock wave disruption of brain tissue.
Clinical Features
- History of direct trauma to head or deceleration.
- Patient must be assessed fully for other injuries.
- Level of consciousness determined by GCS.
- Headache, nausea, vomiting, a falling pulse rate and rising BP indicate cerebral oedema.
- Neurological assessment: motor exam, sensory exam, reflex exam, cranial nerves.
- Brainstem tests: pupillary exam, ocular movements, corneal reflex, gag reflex;
Investigations
- CT/MRI scan: show contusions, haematomas, hydrocephalus, cerebral oedema. CT is the diagnostic study of choice.
- Skull X-ray: no benefit if CT is being performed. If CT unavailable two views should be obtained. Plain radiographs are used to exclude cervical spine injury.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


