Overview of Urinary Bladder Neoplasms
Jesse K. McKenney, MD
Mahesha Vankalakunti, MD
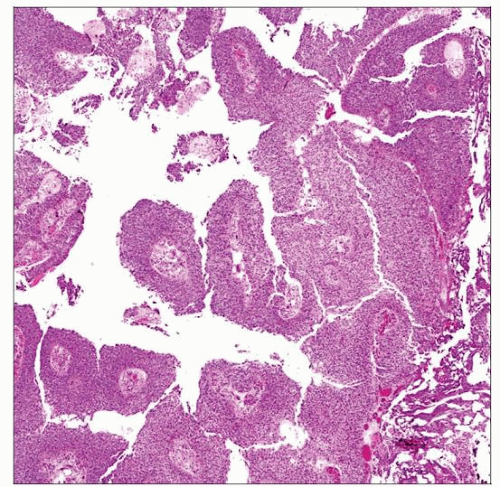 The spectrum of neoplasia in the bladder includes noninvasive papillary urothelial carcinomas. These may progress to invasive urothelial carcinoma; the risk of progression is related to grade. |
 Nonpapillary forms of urothelial carcinoma also occur, as demonstrated by this urothelial carcinoma in situ. Progression to invasion may also arise in these flat urothelial carcinomas. |
EPIDEMIOLOGY
Incidence
7th most common cancer worldwide
260,000 new cases each year in men
76,000 new cases each year in women
In USA, over 90% are urothelial in origin
Pure squamous cell carcinoma and adenocarcinoma represent < 5%
In regions of endemic schistosomiasis, squamous cell carcinoma is most common
Ethnicity Relationship
Highest incidence in Western Europe, North America, and Australia
Incidence in developed countries is 6x higher than nondeveloped countries
2x more common in American white men than African-American men
Gender
Approximately 3x more common in men than women
Natural History
For noninvasive tumors, recurrence and progression rates depend on grade
Urothelial papilloma
Recurrence: 0-8%
Grade or stage progression: 0%
Papillary urothelial neoplasm of low malignant potential
Recurrence: 25-47%
Grade or stage progression: 8%
Low-grade carcinoma
Recurrence: 48-71%
Progression and death due to disease: < 5%
High-grade carcinoma
Almost all disease-related deaths are secondary to high-grade tumors
40-45% of newly diagnosed bladder cancer is high grade
Stage progression: 20% progress to invasion and 12% die of disease
For invasive tumors, outcome depends on stage
Superficial (pT1)
For some patients, conservative management is sufficient
Subset will progress to pT2 disease and require cystectomy
Invasion of muscularis propria and beyond (greater than pT2)
50% of patients with pT2 or greater disease have occult metastases at diagnosis
Most of these develop overt signs of metastasis within 1 year
Distant metastasis
Very poor prognosis
Poor response to adjuvant therapy
Age Range
Typically seen in adults
More common after 60 years of age
In children and adolescents, urothelial papilloma and papillary urothelial neoplasm of low malignant potential may be seen
Urothelial carcinoma is extraordinarily rare in young patients
Environmental Factors
Tobacco smoking
Major established risk factor for bladder cancer
2.6x increased risk in smokers
Risk increases with duration and intensity (pack years)
Occupational exposure
Aniline dye
Aromatic amines
Benzidine
2-naphthylamine
Chronic inflammation
Chronic urinary tract infection and calculi proposed as risk factor
Other drugs
Chronic abuse of analgesics that include phenacetin
Cyclophosphamide for cancer therapy
Chlornaphazine
Infectious Etiology
Schistosomiasis
Squamous cell carcinoma
Urothelial carcinoma
Human papilloma virus
Condyloma
Squamous dysplasia
Squamous cell carcinoma
CLINICAL IMPLICATIONS
Anatomic Considerations
Microscopic anatomy of bladder is key to proper staging
Lamina propria
Connective tissues present between urothelium and detrusor muscle (muscularis propria)
Contains loose stroma and variably sized blood vessels
Includes thin muscle bands of muscularis mucosae
Muscularis propria
Thick aggregated muscle bundles of detrusor muscle
Perivesical soft tissue
Adipose tissue deep to muscularis propria
Adipose tissue does not define extravesical location as it is also present in lamina propria and muscularis propria
Intraoperative (Frozen Section) Evaluation
Usually urothelial margin evaluation
Ureters
Generally sectioned en face
En face sections should include entire wall (urothelium, muscularis, and adventitia)
Examination usually for carcinoma in situ
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


